
Abstract
The regulation of adrenarche is one of the enigmas of pediatric endocrinology. Adrenarche is thought to be governed by a dual control mechanism in which an adrenal androgen secretagogue acts upon a zona reticularis primed by ACTH. We hypothesized that corticotropin-releasing hormone (CRH) may serve as adrenal androgen secretagogue. We tested the concept by infusing either saline or human (h) CRH (1 µg/kg/h in saline) over 3 h, after overnight dexamethasone pretreatment, into eight young men within a randomized, cross-over study design. Serum ACTH and dehydroepiandrosterone-sulfate were measured once hourly; DHEA, androstenedione and 17-hydroxy-progesterone were determined at baseline and after 3 h of saline/hCRH infusion. ACTH levels remained unaltered during saline infusion and average ACTH responses amounted to 13 pg/mL (3.3 pmol/L) during hCRH infusion. Neither saline nor hCRH infusion altered 17-hydroxy-progesterone levels. Serum dehydroepi-androsterone-sulfate rose swiftly within 3 h of hCRH infusion and remained unchanged after saline (mean increase 37 versus 1%; p < 0.01). On average, serum DHEA doubled and androstenedione tripled during hCRH infusion, although no changes were observed during saline infusion (p < 0.01). In conclusion, CRH appears to have the capacity to act as adrenal androgen secretagogue. We suggest that the enigma of adrenarche may have an elegant solution, with CRH and ACTH coupled in sequence at the hypothalamic-pituitary level, and in parallel within the zona reticularis, just as they presumably are within the fetal adrenal, which is exposed to CRH of placental origin.
Similar content being viewed by others

Main
The regulation of adrenarche continues to be one of the enigmas of endocrinology. We explored a novel hypothesis based on three premises. First, clinical evidence indicates that adrenarche is governed by a dual control mechanism in which an adrenal androgen secretagogue is thought to act upon a zona reticularis primed by ACTH(1–4). Second, in many respects, adrenarche is reminiscent of fetal adrenal function; key characteristics shared by the fetal adrenal and the zona reticularis are a low level of expression of 3β-HSD, and abundant DHEA sulfotransferase activity, and a relative increase in 17,20-lyase to 17α-hydroxylase activity of cytochrome P450c17, the enzyme that catalyzes both activities(1,5,6). Third, CRH was recently found to increase DHEAS production by human fetal adrenal cells in culture(7). Accordingly, we hypothesized that CRH might be an adrenal androgen secretagogue that participates directly in the dual control mechanism thought to regulate adrenarche.
We report on a first challenge of the concept. The study examined whether exogenous CRH is capable of eliciting an adrenal androgen response in young men, when the CRH-driven ACTH response is blunted by pretreatment with dexamethasone.
STUDY DESIGN AND METHODS
Either saline or hCRH in saline was infused (1 µg/kg/h iv for 3 h, start at 0800 h) after pretreatment with dexamethasone (1 mg at midnight, before infusion) into eight healthy males (age 16-22 y) within a randomized, cross-over design (2-4 wk between infusions). None of the subjects had a body mass index above 26 kg/m2 or had received steroid medication during the months before study.
Serum ACTH, cortisol, and DHEAS were measured once hourly; DHEA, androstenedione, and 17-OHP were determined at baseline and after 3 h of saline/hCRH infusion.
ACTH and DHEAS were determined by a solid-phase, two-site chemiluminescent enzyme immunometric assay for use with Immulite Automated analyzer; the intra- and interassay CVs were 6.1 and 8.3%, respectively, 8.1 and 13%. The minimally detectable ACTH concentration was 10 pg/mL (2.2 pmol/L).
DHEA was assayed using a tritiated kit (ICN Biomedical Inc., Carson, CA). The intra- and interassay CVs were 7 and 14%. Cortisol was measured by radioimmunoassay (Immunotech, France). The intra- and interassay CVs were 6.5 and 6.9%. Serum 17-OHP and androstenedione levels were measured by radioimmunoassay(8). Results are expressed as means ± SEM, unless stated otherwise. Mann-Whitney U test was used for statistical comparisons (significance at p < 0.05). The study protocol was approved by the Institutional Review Board of the Barcelona Hospital. Written informed consent was obtained before study start.
RESULTS
Serum ACTH concentrations remained unaltered during saline infusion, but increased gradually during hCRH infusion from 22 ± 5 to 35 ± 6 pg/mL (4.9 ± 1.1 to 7.8 ± 1.3 pmol/L).
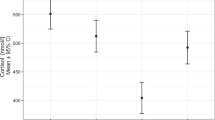
Neither saline nor hCRH infusion altered 17-OHP levels; median values and interquartile ranges for cortisol were all less than 1 µg/dL (<27.6 nmol/L) at baseline and after saline infusion, and were no more than 11.6 µg/dL [range 7.1 to 17.2 µg/dL] (320; 196 to 475 nmol/L) after 3 h of hCRH infusion. The intraindividual difference between baseline DHEAS concentrations averaged 2 ± 3%, a finding corroborating DHEAS as a robust marker of the individual hormonal milieu. After 3 h of infusion, DHEAS responses to hCRH (increment of 37 ± 17%) were higher (p = 0.003) than to saline (1 ± 4%) (Fig. 1). Similarly, within 3 h of infusion, hCRH elicited a doubling of serum DHEA (increment of 121 ± 41%) and a tripling of androstenedione (increment of 189 ± 43%), each of these rises being pronounced (p = 0.006 and 0.0007) when compared with the changes after saline (respectively -4 ± 6% and -12 ± 8%) (Fig. 2).

Serum DHEAS concentrations in men receiving an infusion with either saline (CRH -) or hCRH in saline (CRH +) in a randomized sequence with an interval of 2-4 wk. Note the similarity of baseline concentrations; hCRH infusion evokes a swift rise of DHEAS levels.

Relative changes in serum concentrations of DHEAS, DHEA, and androstenedione between the start and end of a 3-h infusion with either saline (CRH -) or hCRH in saline (CRH +) into young men.
DISCUSSION
CRH infusion into young men who had been pretreated with dexamethasone was found to evoke a small rise in circulating ACTH followed by a consistent increment of cortisol (but not of 17-OHP), and to elicit a brisk increase in the serum concentrations of DHEAS, DHEA, and androstenedione. Recently, it has been convincingly established that ACTH rises in the observed range fail to induce the aforementioned constellation of responses, in particular the striking increases of DHEAS and androstenedione(9–15). Accordingly, CRH itself is thought to serve as adjuvant adrenal androgen secretagogue.
The origin of CRH as a potential adrenal androgen secretagogue and the mechanisms by which CRH appears to stimulate adrenal androgen release are currently unknown. For example, data are lacking on changes in the pattern of plasma CRH during postnatal development and aging, and its correlation with the concentration of plasma DHEAS. It is possible that the endogenous CRH, hypothesized to be physiologically involved, has an intraadrenal origin and acts through a paracrine pathway(16,17).
The presence of CRH receptors in the zona reticularis has hitherto not been explored; CRH receptors were found to be expressed in the human fetal adrenal(7). At present, it is also uncertain whether CRH has the capacity to increase 17,20 lyase activity within the zona reticularis, e.g. by increasing expression or serine phosphorylation of P450c17, either directly or indirectly(18).
Fetal growth restriction has been linked to the subsequent development of exaggerated adrenarche and/or precocious pubarche(19–22). CRH may be one of the missing links involved in this poorly understood association, because growth-retarded fetuses are characterized by markedly elevated serum concentrations of CRH and by low circulating levels of DHEAS(23,24).
In conclusion, we found that exogenous hCRH, unlike ACTH alone, is a potent adrenal androgen secretagogue and speculate that it may be a key regulator of adrenarche. The enigma may thus prove to have an elegant solution with CRH and ACTH being coupled in sequence at the hypothalamic-pituitary level and in parallel within the zona reticularis, just as they presumably are within the fetal adrenal, which is exposed to CRH of placental origin.
Abbreviations
- CRH:
-
corticotropin-releasing hormone
- hCRH:
-
human CRH
- DHEA:
-
dehydroepiandrosterone
- DHEAS:
-
dehydroepiandrosterone-sulfate
- 3β-HSD:
-
3β-hydroxysteroid dehydrogenase-isomerase
- 17-OHP:
-
17-hydroxy-progesterone
- CV:
-
coefficients of variation
References
Grumbach MM, Styne DM 1998 Puberty: ontogeny, neuroendocrinology, physiology, and disorders. In: Wilson JD, Foster DW, Kronenberg HM, Larsen PR (eds) Williams Textbook of Endocrinology. WB Saunders, Philadelphia, 1548–1550.
Weber A, Clark AJL, Perry LA, Honour JW, Savage MO 1997 Diminished adrenal androgen secretion in familial glucocorticoid deficiency implicates a significant role for ACTH in the induction of adrenarche. Clin Endocrinol 46: 431–437.
Gell JS, Carr BR, Sasano H, Atkins B, Margraf L, Mason JI, Rainey WE 1998 Adrenarche results from development of a 3β-hydroxysteroid dehydrogenase-deficient adrenal reticularis. J Clin Endocrinol Metab 83: 3695–3701.
Endoh A, Kristiansen SB, Casson PR, Buster JE, Hornsby PJ 1996 The zona reticularis is the site of biosynthesis of dehydroepiandrosterone and dehydroepiandrosterone sulfate in the adult human adrenal cortex resulting from its low expression of 3β-hydroxysteroid dehydrogenase. J Clin Endocrinol Metab 81: 3558–3565.
Doody KM, Carr BR, Rainey WE, Byrd W, Murry BA, Strickler RC, Thomas JL, Mason JI 1990 3β-hydroxysteroid dehydrogenase-isomerase in the fetal zone and neocortex of the human fetal adrenal gland. Endocrinology 126: 2493–2498.
Pepe GJ, Albrecht ED 1990 Regulation of the primate fetal adrenal cortex. Endocrinol Rev 11: 151–176.
Smith R, Mesiano S, Chang EC, Brown S, Jaffe RB 1998 Cortocotropin-releasing hormone directly and preferentially stimulates dehydroepiandrosterone sulfate secretion by human fetal adrenal cortical cells. J Clin Endocrinol Metab 83: 2916–2920.
Ib´ñz L, Potau N, Zampolli M, Prat N, Virdis R, Vicens Calvet E, Carrascosa A 1996 Hyperinsulinemia in postpubertal girls with a history of premature pubarche and functional ovarian hyperandrogenism. J Clin Endocrinol Metab 81: 1237–1243.
Parker LN 1991 Control of adrenal androgen secretion. Endocrinol Metab Clin North Am 20: 401–421.
Daidoh H, Morita H, Mune T, Murayama M, Hanafusa J, Ni H, Shibata H, Yasuda K 1995 Responses of plasma adrenocortical steroids to low dose ACTH in normal subjects. Clin Endocrinol 43: 311–315.
Bridges NA, Hindmarsh PC, Pringle PJ, Honour JW, Brook CGD 1998 Cortisol, androstenedione (A4), dehydroepiandrosterone sulphate (DHEAS) and 17-hydroxyprogesterone (17-OHP) responses to low doses of 1:24 ACTH. J Clin Endocrinol Metab 83: 3750–3753.
Lashansky G, Saenger P, Fishman K, Gautier T, Mayes D, Berg G, Di Martino Nardi J, Reiter E 1991 Normative data for adrenal steroidogenesis in a healthy population: age- and sex-related changes after adrenocorticotropin stimulation. J Clin Endocrinol Metab 73: 674–686.
Crowley S, Hindmarsh PC, Holownia P, Honour JW, Brook CGD 1991 The use of low doses of ACTH in the investigation of adrenal function in man. J Endocrinol 130: 475–479.
Griffing GT, Allen J, Pratt H, Melby JC 1985 Discordance of plasma DHEA-S, DHEA, and cortisol responses with various ACTH regimens. Metabolism 34: 631–636.
Ambrosi B, Barbetta L, Re T, Passini E, Faglia G 1998 The one microgram adrenocorticotropin test in the assessment of hypothalamic-pituitary-adrenal function. Eur J Endocrinol 139: 575–579.
Andreis PG, Neri G, Nussdorfer GG 1991 Corticotropin-releasing hormone (CRH) directly stimulates corticosterone secretion by the rat adrenal gland. Endocrinology 128: 1198–1200.
Ehrhart-Bornstein M, Hinson JP, Bornstein SR, Scherbaum WA, Vinson GP 1998 Intraadrenal interactions in the regulation of adrenocortical steroidogenesis. Endocr Rev 19: 101–143.
Miller WL 1998 Early steps in androgen biosynthesis: from cholesterol to DHEA. Baillière Clin Endocrinol Metab 12: 67–81.
Clark PM, Hindmarsh PC, Shiell AW, Law CM, Honour JW, Barker DJP 1996 Size at birth and adrenocortical function in childhood. Clin Endocrinol 45: 721–726.
Francois I, de Zegher F 1997 Adrenarche and fetal growth. Pediatr Res 41: 440–442.
Ibaáñez L, Potau N, Francois I, de Zegher F 1998 Precocious pubarche, hyperinsulinism, and ovarian hyperandrogenism in girls: relation to reduced fetal growth. J Clin Endocrinol Metab 83: 3558–3562.
Dahlgren J, Boguzewski M, Rosberg S, Albertsson-Wikland K 1998 Adrenal steroid hormones in short children born small for gestational age. Clin Endocrinol 49: 353–361.
Turnispeed MR, Bentley K, Reynolds JW 1976 Serum dehydroepiandrosterone sulfate in premature infants and infants with intrauterine growth retardation. J Clin Endocrinol Metab 43: 1219–1225.
Goland RS, Jozak S, Warren WB, Conwell IM, Stark RI, Tropper PJ 1993 Elevated levels of umbilical cord plasma corticotropin-releasing hormone in growth-retarded fetuses. J Clin Endocrinol Metab 77: 1174–1179.
Acknowledgements
The authors thank Dr. Eric Mehuys (Ferring, Belgium) for the gift of hCRH, and Ms. Karin Vanweser, RN for editorial assistance. F.d.Z. is a Clinical Research Investigator, Fund for Scientific Research, Flanders, Belgium.
Author information
Authors and Affiliations
Additional information
Supported by a scholarship from the European Society For Paediatric Endocrinology.
Rights and permissions
About this article
Cite this article
Ibáñez, L., Potau, N., Marcos, M. et al. Corticotropin-Releasing Hormone as Adrenal Androgen Secretagogue. Pediatr Res 46, 351–353 (1999). https://doi.org/10.1203/00006450-199909000-00018
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199909000-00018
This article is cited by
-
Preclinical models of prostate cancer — modelling androgen dependency and castration resistance in vitro, ex vivo and in vivo
Nature Reviews Urology (2023)
-
A cross-sectional survey of adrenal steroid hormones among overweight/obese boys according to puberty stage
BMC Pediatrics (2019)
-
Clinical spectrum of premature pubarche: Links to metabolic syndrome and ovarian hyperandrogenism
Reviews in Endocrine and Metabolic Disorders (2009)
