
Abstract
Myocardial growth during fetal life is accomplished by proliferation of the number of myocytes (hyperplasia). Shortly after birth, normal growth of the heart is predominantly due to increase in cell size (hypertrophy), and myocytes largely lose the capability to replicate. This change is characterized by a decrease in myocardial DNA concentration and an increase in protein/DNA concentration ratio. Among many of the events associated with birth is an increase in plasma cortisol concentrations in the few days before delivery of the fetus. To determine the possible role of cortisol in the postnatal change in myocardial growth, we measured DNA and protein concentrations in the free walls of the left (LV) and right (RV) ventricles in normal fetal lambs, normal newborn lambs, and in fetal lambs in which cortisone was infused for 72-80 h into the left coronary artery, which we showed does not perfuse the RV free wall. Normally, fetal RV DNA is higher than LV DNA concentration, and DNA/protein ratio is lower in RV than in LV. It is suggested that this could be related to the greater load on the RV. Postnatally, protein concentrations increase progressively, but DNA remains the same in both ventricles, and protein/DNA ratios increase. Cortisol, infused to achieve normal prenatal levels in LV myocardium, markedly decreases LV DNA without affecting RV DNA concentrations. The present study indicates that cortisol inhibits myocyte replication and that cortisol simulates the change in myocardial growth pattern normally occurring after birth. It raises concerns regarding prenatal administration of glucocorticoids to mothers to mature the fetal lungs before preterm delivery.
Similar content being viewed by others

Main
Prenatally, growth of the heart is characterized by increased myocardial cell numbers or hyperplasia(1). However, soon after birth, myocytes largely lose their capacity to proliferate, and myocardial growth is characterized by an increase in individual cell size or hypertrophy(1). This postnatal change in the mechanism of myocardial growth is also evidenced by the observation that DNA is actively synthesized in the rat immediately after birth, but, by approximately 3 wk postnatal, synthesis ceases almost completely(2). The factors responsible at the time of birth for this differentiation of myocardial growth from a pattern of hyperplasia to one of hypertrophy have not been defined. In addition to the increase in arterial blood oxygen content after birth, many hormonal changes occur perinatally, including an increase in plasma catecholamine(3) and triiodothyronine concentrations(4) and also a rise in glucocorticoid concentrations(5,6).
Prenatal administration of the synthetic glucocorticoid dexamethasone to pregnant rats resulted in a decrease in myocardial DNA content in the neonates in the first week after birth, suggesting that cell division was subnormal(7). However, in a similar study, prenatal dexamethasone administration seemed to increase cellular proliferation in the developing heart, indicating that the differentiation of myocardial growth was delayed by glucocorticoid(8). In both these studies, all fetal tissues and organs were exposed to glucocorticoids, and total body growth was affected. Therefore, it is not possible to infer whether glucocorticoid has a direct influence on the myocardium or whether its effect may be secondary to other mechanisms induced by glucocorticoid. We have examined the effect of infusion of cortisol into the left coronary artery of fetal lambs. In this model, the LV and septum are perfused by the cortisol, but the cortisol concentration is not increased in blood supplying the remainder of the body, including the free wall of the RV. To assess the effects of cortisol, we measured DNA and protein concentrations in the free walls of the LV and RV in a control group of fetal lambs, in a group of lambs in which cortisol was infused into the left coronary artery, and in postnatal lambs.
METHODS
Animals. The study comprised three groups of animals. The first group included 12 fetal lambs with gestational ages of 125-133 (128.5 ± 4.3, mean ± SD) d. These were the undisturbed twins of lambs used for hemodynamic studies or lambs that were used as tissue donors. The second group of animals consisted of seven newborn lambs aged 1-10 d. The third group consisted of nine fetal lambs with gestational ages of 124-131 (128.8 ± 2.6, mean ± SD) d in which the left coronary artery was catheterized. Cortisol was infused in six of these animals, and 0.9% NaCl solution was infused in the remaining three animals. Animal husbandry and study design followed the guidelines of the National Institutes of Health and were approved by the Committee on Animal Research of the University of California, San Francisco.
Surgical procedures for coronary artery catheterization. After fasting for 24 h, the ewes were given 0.3 mg buprenorphine and 750-1000 mg ketamine intramuscularly. With local anesthesia with lidocaine, a catheter was inserted into a pedal vein and 0.9% NaCl was infused; ketamine HCl was injected intravenously in 200-mg doses every 10 min to maintain anesthesia. The uterus was exposed through a midline abdominal incision, the left forelimb was extracted, and, with additional anesthesia with 1% lidocaine HCl, the chest was opened in the third left intercostal space. The pericardium was incised along the course of and caudal to the pulmonary trunk. The left atrial appendage was gently retracted to show the left coronary artery. A short segment of the main coronary artery and a small branch coursing to the right were gently stripped of overlying pericardium.
The coronary arterial catheter was constructed in the same way as the catheter we had designed for renal venous catheterization(9), but a 24-gauge cannula was used. The tip was made only long enough to access the main left coronary artery to avoid allowing it to pass beyond the ostium into the aorta. After placing a stay suture in the myocardium adjacent to where the coronary artery was to be entered, the catheter-cannula assembly was inserted and advanced into the main left artery. In seven animals, the catheter was inserted into the small branch (Fig. 1), and, in two animals, it was inserted into the anterior descending artery close to its origin from the main artery. The suture was ligated behind the sleeve, and a polyvinyl catheter (0.030-in inner diameter, 0.04-in outer diameter) was connected to the cannula. A catheter of the same size was inserted into the left brachial artery and advanced to the subclavian artery. The chest was closed and the uterine incision was sutured. The catheters were exteriorized on the flank, filled with heparin, and sealed. They were protected by a pouch sutured to the flank. In two animals, a catheter was also placed in the coronary sinus via the hemiazygos vein, as we have described previously(10).

Silicone rubber cast of left coronary artery in a 125-d gestation fetal lamb. No branches are distributed to the RV free wall. The small septal branch (Sep A) just beyond the origin of the main vessel was catheterized in most fetuses. AA, ascending aorta; LCCA, left circumflex coronary artery; LAD, left anterior descending branch.
Study design. In the control group, the ewe was anesthetized with intravenous sodium pentobarbital, the fetus was removed and killed with an additional intravenous dose, and the heart was immediately removed and processed as described below. Newborn lambs were also killed with intravenous sodium pentobarbital, and the hearts were removed and processed immediately.
The animals in which the left coronary artery was catheterized were allowed to recover for 24 h. The ewe was placed in a stall and allowed free access to food and water. A continuous infusion of 0.9% NaCl solution at a rate of 0.1 mL/min was given into the coronary arterial catheter. In six fetuses, cortisol was added to the infusate to provide a dose of 1.2 µg/min, whereas the other three fetuses received only 0.9% NaCl. The cortisol infusion rate was calculated on the basis of an estimation of left coronary blood flow of approximately 25 mL/min in fetuses of the age studied and to achieve a concentration of approximately 50-75 ng/mL in blood perfusing the LV. The infusion was maintained for 72-80 h. The ewe and fetus were killed as described above. Before removing the heart, the placement of the catheter tip in the main left coronary artery was confirmed.
Blood gases and pH were measured daily in blood withdrawn from the brachial artery, and cortisol concentrations were measured intermittently. Cortisol concentrations were also measured in coronary sinus blood in the two animals in which the coronary sinus was catheterized. Blood gases and pH were measured with a Corning 175 blood gas analyzer (Medfield, MA). Cortisol concentrations were measured by RIA, using the MAGIC cortisol RIA kit (Chiron Diagnostics, E. Walpole, MA). Norepinephrine concentrations were measured by HPLC and electrochemical detection (ESA model 5700, ESA Inc., Bedford, MA).
Studies of myocardium. In three fetuses, at the end of the study and by procedures similar to those described above, the fetus was again exposed, the chest was opened, and the heart was examined. Methylene blue solution was injected into the catheter in the left coronary artery. The dye was evident over the whole LV surface but was not apparent over the free wall of the RV. Silicone rubber injected into the left coronary artery in four fetuses of gestational age similar to those included in this study also reached only the LV and septum; no cross-branches to the right coronary artery were evident, and the silicone rubber was not distributed to the free wall of the RV (Fig. 1).
The hearts were dissected to separate the free walls of the LV and RV. Several samples were obtained for DNA and protein analysis from each ventricle. Also, samples were obtained for calculation of dry weight to wet weight ratios. The samples were immediately frozen in liquid nitrogen and thawed later for analysis. After homogenizing the tissues, DNA concentrations were measured in duplicate using a modification of the fluorometric method described by Setaro and Morley(11). Protein concentrations were measured in duplicate using the Sigma Chemical Co. bicinchoninic acid protein assay kit (Sigma Chemical Co., St. Louis, MO). Tissues were weighed before and after drying at 80°C for 2 d; further warming did not result in a decrease in weight.
Data analysis. The DNA and protein concentrations and protein/DNA ratios in the different conditions were compared by ANOVA and unpaired t test with Bonferroni correction; when variables did not have a normal distribution, the Kruskal-Wallis ANOVA was used. LV and RV DNA and protein concentrations and protein/DNA ratios were assessed by the Mann-Whitney nonparametric t test. The relationships between DNA and protein concentrations and DNA/protein ratios with postnatal age were examined by linear regression. All data were expressed as mean ± 1 SD. A p value < 0.05 was considered statistically significant.
RESULTS
Control blood gases before infusion of cortisol showed normal values of pH 7.37 ± 0.06, PO2 21.94 ± 2.86 mm Hg, and PCO2 53.33 ± 7.51 mm Hg. These did not change significantly after the infusion and at the end of infusion were 7.37 ± 0.03, 22.20 ± 2.99 mm Hg, and 55.54 ± 5.19 mm Hg, respectively. Also, plasma norepinephrine concentrations showed no significant changes; control levels were 164 ± 111 and postinfusion levels 198 ± 123 pg/mL.
In the two animals in which we measured cortisol concentrations in coronary sinus blood, levels were 55 and 58 ng/mL, which were in the range we attempted to achieve. Cortisol concentrations in arterial blood on the first day after infusion were 9.45 ± 5.34 ng/mL, and on the second and third days were 18.10 ± 6.09 and 18.10 ± 5.59 ng/mL, respectively; these were not significantly higher than those measured in normal fetal lambs at this gestational age(12).
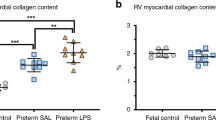
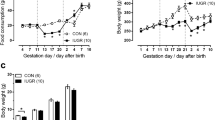
DNA concentrations. LV and RV myocardial concentrations are shown in Table 1 and Fig. 2. LV concentrations in the cortisol-infused lambs were significantly lower than in the other groups (p < 0.04 versus controls). In the control group of fetal lambs, RV DNA concentrations were significantly lower than those in LV myocardium, but in the group with cortisol infusion into the left coronary artery, RV DNA concentrations were significantly higher than those in the LV. In the newborn lambs, there was no significant difference in RV and LV DNA concentrations. In the newborn lambs, the DNA concentrations in both ventricles fell progressively in the first 10 postnatal d (Fig. 3).

DNA and protein concentrations and protein/DNA ratios in the LV and RV are shown for control fetal and newborn lambs and for fetal lambs in which cortisone was infused into the left coronary artery for 72-80 h. Data are presented as mean ± SD.

Relationships between DNA and protein concentrations and protein/DNA ratios and postnatal age are shown in newborn lambs.
Protein concentrations (Table 1). No significant differences in LV or RV myocardial protein concentrations were noted between control fetuses and those in which cortisol was infused into the left coronary artery. Protein concentrations in both LV and RV myocardium were significantly higher in newborn lambs compared with both control and cortisol-infused fetal lambs. The protein concentrations in both the LV and RV were lower in the animals in which saline was infused in the coronary artery; this was not statistically significant, but only three animals were studied.
No significant differences between protein concentrations in LV and RV myocardium were noted in any of the groups. Also, protein concentration in either ventricle did not change significantly with postnatal age (Fig. 3).
Protein/DNA concentration ratios (Table 1 and Fig. 2). LV myocardial protein/DNA ratios were markedly higher in the fetuses in which cortisol was infused into the left coronary artery (p < 0.0001 compared with control fetuses). The ratios were also higher in both the LV and RV in the newborn lambs (p < 0.0005 compared with control fetuses). There was no significant difference between LV protein/DNA ratios in the cortisol-infused fetuses compared with newborn lambs.
RV protein/DNA ratios were not significantly different between the control fetal group and the cortisol-infused fetuses and newborn lambs. Both RV and LV myocardial protein/DNA ratios were lower in the saline-infused group of three fetuses. The RV myocardial protein/DNA concentration ratio was significantly greater than in the LV. Protein/DNA ratios fell progressively in the first 10 postnatal d (Fig. 3).
Dry weight/wet weight ratios. To determine whether cortisol infusion altered water content of the myocardium, the ratios of dry to wet weight were calculated for both ventricles in the control fetuses and those infused with cortisol. No significant differences were noted between the ratios in the LV (0.169 ± 0.107) and RV (0.158 ± 0.007) in the control fetuses or in the ratio in LV (0.169 ± 0.010) or RV (0.170 ± 0.008) in cortisol-infused fetuses. Also, no significant differences were observed in the fetuses that received cortisol compared with controls.
DISCUSSION
In the adult, the heart hypertrophies in response to an increased workload. Numerous studies in several species have shown that this results largely from an increase in myocyte size. In a study in rats in which LV mass was increased by ascending aortic constriction, there was an actual decrease in the number of nuclei in LV muscle, suggesting that myocyte size and not numbers accounted for the increase in mass(13). Although DNA content increased, indicating that total nuclear numbers or size was greater, Grove et al.(14) showed that this was due to proliferation of nonmuscle cells. Little mitosis is observed in the myocardial cells beyond the first few weeks after birth, and numerous observers have concluded that beyond the neonatal period, normal myocardial growth can also be attributed almost exclusively to enlargement of individual myocytes (hypertrophy) without increase in cell numbers (hyperplasia)(15,16).
In contrast with the adult heart, active mitotic division of myocytes has been observed in embryonic and fetal hearts(1,17). Smolich et al.(18) did morphometric studies in hearts of sheep ranging from 115 d gestation to adulthood. During the fetal period, myocyte diameters increased by <20% in late gestation, indicating that muscle grew largely by hyperplasia. After birth, diameter increased rapidly to almost 3 times fetal myocyte diameter in the adult LV and to twice fetal diameter in the RV, showing hypertrophy.
DNA and protein concentrations have been applied to estimation of cell numbers and size in numerous tissues(19,20). DNA concentration has reflected the number of cells, whereas protein/DNA concentration ratio has been considered to indicate cell size. A relatively high DNA concentration, therefore, would indicate a large number of cells but also could result from an increase in nuclear numbers or size within each cell. In the fetus, the vast majority of myocytes are mononucleate, but, after birth, a large proportion of cells (18-25% in the human) are either binucleate or multinucleate(13,21). In accordance with the observation that myocyte numbers increase during the first week after birth in the rat, DNA synthesis is active during this period but declines rapidly and stops by 3 wk(22). These increased DNA concentrations can be explained by both hyperplasia of myocytes and polyploidy(23).
In our studies in the normal sheep fetus, the DNA concentrations in the LV myocardium were approximately 25% higher than in the RV, suggesting that the LV has more myocytes per gram of tissue. Also, the protein/DNA ratio in RV myocardium was approximately 30% higher than that in the LV, suggesting that RV myocytes are larger. This is in agreement with the morphometric studies of Smolich et al.(18) who showed that the cross-sectional area of RV myocytes was approximately 30% greater than that of LV myocytes in fetal lambs at the same gestational age as those we studied. In the newborn lambs, RV and LV myocardial DNA concentrations were not significantly different; nor were protein/DNA ratios different in the two ventricles. These findings also conform with the morphometric findings that by 1 wk after birth, myocyte cross-sectional areas were similar in the two ventricles.
The factors determining cell size and growth in the fetus have not been defined. In the sheep fetus, the RV ejects almost twice the volume ejected by the LV at the same pressure(24). This suggests that even though normal increase in myocardial mass is accomplished by myocyte hyperplasia prenatally, the workload on the ventricle may also stimulate a limited degree of hypertrophy, as it does in the adult heart.
The perinatal factors that could induce the change in the myocardial cell from the prenatal pattern of growth by hyperplasia to growth by hypertrophy postnatally have not been fully defined. Arterial oxygen tension increases from approximately 25 to 90-100 mm Hg. It is unlikely that this has a significant effect on the myocardium; fetal myocardial oxygen supply and consumption are the same as in the adult in relation to muscle weight, because coronary blood flow is high(10). Circulating concentrations of several hormones increase perinatally. Thyroid activity increases at birth, and triiodothyronine concentrations increase within 3-4 h after birth(4). Plasma norepinephrine concentrations increase within minutes after delivery of normal lambs(3) and rise during labor. However, the role of glucocorticoids has evoked the most interest.
Plasma cortisol concentrations have been measured sequentially in fetal lambs; they are low before approximately 120 d gestation, then rise gradually and increase markedly 2-3 d before birth(25). Glucocorticoids have been shown to be involved in perinatal maturation in several fetal organs. They have been shown to accelerate appearance of pulmonary surfactant in fetal lambs(26) and are now widely used clinically for this effect(27). However, Kauffman(28) showed that prenatal administration of dexamethasone enhanced differentiation of pulmonary epithelial cells in rats but interfered with cell proliferation, so that the total number of cells in the lung was reduced. Dexamethasone administered in late gestation to pregnant rats reduced the normal rapid postnatal cell division in the kidney and heart, as manifested by a decrease in DNA content(7). Glucocorticoid administration to neonatal rats(29) as well as to premature human infants(30) induces cardiac hypertrophy.
Because of this ample evidence that glucocorticoids have dramatic effects on cardiac growth, we proceeded to assess whether the normal prenatal rise in circulating cortisol concentrations could be responsible for the change in the pattern of myocardial growth that occurs normally after birth. Further, we wanted to determine whether the effect of glucocorticoid in the heart is direct. In all previous studies, the effects could have been the indirect result of effects on other organs or endocrine functions, because synthetic glucocorticoids were given to the mother.
In one preparation in which we infused cortisone directly into the left coronary artery, only the LV free wall and septum were perfused by glucocorticoid, and none reached the RV. We showed that infusion of saline into the coronary artery had no significant effects on myocardial DNA or protein concentrations. We selected fetuses at the age of 125-130 d at a time before cortisol concentrations began to increase significantly. The amount of cortisone infused was calculated to attempt to expose the LV myocardium to concentrations usually achieved in the lamb in the few days before birth. We simulated this prenatal increase in plasma cortisol concentration by infusing for a 72-80 h period(25). We estimated the rate to be infused from measurements of coronary blood flow to the myocardium perfused by the left coronary artery that we made using indocyanine green (our unpublished observations). This flow was approximately 25 mL/min in lambs of the gestational age used for the cortisol study. By infusing 1.2 µg/min, we estimated that the concentration in coronary blood would be approximately 50 ng/mL; in the two lambs in which we measured cortisol concentrations in coronary sinus blood, the concentrations were 55 and 58 ng/mL, respectively. The total infusion rate per 24 h was 1.7 mg; this is well below the infusion rate of cortisol used by Jack et al.(31) to induce labor in sheep. They started with 2.8 mg/24 h and doubled the infusion rate daily, reaching 22.4 mg/24 h. We measured cortisol in fetal arterial blood; concentrations did not rise significantly over the period of infusion and were within the normal range for the age of the fetuses.
We have clearly shown that cortisol, when selectively infused into the left coronary artery, reduced DNA concentration and markedly increased protein/DNA concentration in LV myocardium, but did not decrease DNA concentrations or alter protein/DNA ratios in the RV myocardium. This confirms that cortisol has a direct local effect on myocardial growth. The normal pattern in which the LV DNA concentration is higher than that in the RV and the LV protein/DNA ratio is lower than in the RV was also changed by cortisol. LV DNA concentration fell below that in the RV, and protein/DNA ratio increased significantly above that in the RV. The significant increase in RV myocardial DNA concentration compared with the decrease in concentration in the LV myocardium is of considerable interest. It could be related to a change in loading conditions. We have shown that infusion of isoproterenol into the left coronary artery of fetal lambs increases LV stroke volume and reduces RV stroke volume (our unpublished observations). It is possible that cortisol infusion into the left coronary artery altered LV performance with a resultant increase in loading of the RV. This requires further exploration.
The normal newborn lambs, which had presumably been exposed to the prenatal rise in cortisol concentrations, showed no differences in DNA or protein concentrations or in protein/DNA ratios between the two ventricles. However, protein concentrations were much increased over normal fetal levels, as were protein/DNA ratios. Interestingly, the protein/DNA ratio in the fetal LV exposed to cortisol was the same as that in the normal newborn. Examination of the rates of change after birth shows a linear decrease in DNA concentrations in both ventricles and an increase in protein/DNA ratios.
These studies have shown the important role of glucocorticoids in differentiation of myocardial cells after birth, but possibly other factors also could be involved. They also raise questions regarding the widespread use of glucocorticoid administration to pregnant women to mature the lungs of infants in threatened preterm delivery, because such use may limit the ultimate complement of myocytes that is achieved in the heart by restricting hyperplasia. It is still to be determined, however, whether the myocyte can revert its pattern of growth to hyperplasia in the fetus or neonate after the surge of glucocorticoids has receded or whether the change is permanent.
Abbreviations
- LV:
-
left ventricle
- RV:
-
right ventricle
References
Oparil S, Bishop SP, Clubb FJ Jr 1984 Myocardial cell hypertrophy or hyperplasia. Hypertension 6: III-38–III-43
Chacko S 1973 DNA synthesis, mitosis, and differentiation in cardiac myogenesis. Dev Biol 35: 1–18
van Bel F, Roman C, Iwamoto HS, Rudolph AM 1993 Sympathoadrenal, metabolic, and regional blood flow responses to cold in fetal sheep. Pediatr Res 34: 47–50
Breall JA, Rudolph AM, Heymann MA 1984 Role of thyroid hormone in postnatal circulatory and metabolic adjustments. J Clin Invest 73: 1418–1424
Dupouy JP, Coffigny H, Magre S 1975 Maternal and foetal corticosterone levels during late pregnancy in rats. J Endocrinol 65: 347–352
Murphy PAE, Branchard LCT 1983 Fetal metabolism of cortisol. Curr Top Exp Endocrinol 5: 197–223
Slotkin TA, Seidler FJ, Kavlock RJ, Bartolome JV 1991 Fetal dexamethasone exposure impairs cellular development in neonatal rat heart and kidney: effects on DNA and protein in whole tissues. Teratology 43: 301–306
Torres A, Belser WW III, Umeda PK, Tucker D 1997 Indicators of delayed maturation of rat heart treated prenatally with dexamethasone. Pediatr Res 42: 139–144
Iwamoto HS, Rudolph AM 1983 Chronic renal venous catheterization in fetal sheep. Am J Physiol 245:H524–H527
Fisher DJ, Rudolph AM, Heymann MA 1980 Myocardial oxygen and carbohydrate consumption in fetal lambs in utero and in adult sheep. Am J Physiol 238:H399–H405
Setaro F, Morley CG 1976 A modified fluorometric method for the determination of microgram quantities of DNA from cell or tissue cultures. Analyt Biochem 71: 313–317
Wood CE, Keil LC, Rudolph AM 1982 Hormonal and hemodynamic responses to vena caval obstruction in fetal sheep. Am J Physiol 243:E278–E286
Grove D, Nair KG, Zak R 1969 Biochemical correlates of cardiac hypertrophy. 3. Changes in DNA content; the relative contributions of polyploidy and mitotic activity. Circ Res 25: 463–471
Grove D, Zak R, Nair KG, Aschenbrenner V 1969 Biochemical correlates of cardiac hypertrophy. 4. Observations on the cellular organization of growth during myocardial hypertrophy in the rat. Circ Res 25: 473–485
Korecky B, Rakusan K 1978 Normal and hypertrophic growth of the rat heart: changes in cell dimensions and number. Am J Physiol 234:H123–H128
Zak R 1973 Cell proliferation during cardiac growth. Am J Cardiol 31: 211–219
Manasek FJ 1968 Mitosis in developing cardiac muscle. J Cell Biol 37: 191–196
Smolich JJ, Walker AM, Campbell GR, Adamson TM 1989 Left and right ventricular myocardial morphometry in fetal, neonatal, and adult sheep. Am J Physiol 257:H1–H9
Enesco M, Leblond CP 1962 Increase in cell number as a factor in the growth of the organs of the young male rat. J Embryol Exp Morph 10: 530–562
Winik M, Noble A 1965 Quantitative changes in DNA, RNA, and protein during prenatal and postnatal growth in the rat. Dev Biol 12: 451–466
Korecky B, Sweet S, Rakusan K 1979 Number of nuclei in mammalian cardiac myocytes. Can J Physiol Pharmacol 57: 1122–1129
Claycomb WC 1979 DNA synthesis and DNA enzymes in terminally differentiating cardiac muscle cells. Exp Cell Res 118: 111–114
Sasaki R, Watanabe Y, Morishita T, Yamagata S 1968 Estimation of the cell number of heart muscles in normal rats. Tohoku J Exp Med 95: 177–184
Rudolph AM, Heymann MA 1967 The course of the circulation of the fetus in utero. Circ Res 21: 163–184
Nathanielsz PW 1994 A time to be born: implications of animal studies in maternal-fetal medicine. Birth 21: 163–169
DeLemos RA, Shermeta DW, Knelson JH, Kotas R, Avery ME 1970 Acceleration of appearance of pulmonary surfactant in the fetal lamb by administration of corticosteroids. Am Rev Respir Dis 102: 459–461
Collaborative Group on Antenatal Steroid Treatment 1981 Effect of antenatal dexamethasone administration on the prevention of respiratory distress syndrome. Am J Obstet Gynecol 141: 276–287
Kauffman SL 1977 Proliferation, growth, and differentiation of pulmonary epithelium in fetal mouse lung exposed transplacentally to dexamethasone. Lab Invest 37: 497–501
Sicard RE, Werner JC 1992 Dexamethasone induces a transient relative cardiomegaly in neonatal rats. Pediatr Res 31: 359–363
Werner JC, Sicard RE, Hansen TW, Solomon E, Cowett RM, Oh W 1992 Hypertrophic cardiomyopathy associated with dexamethasone therapy for bronchopulmonary dysplasia. J Pediatr 120: 286–291
Jack PM, Nathanielsz PW, Rees LH, Thomas AL 1975 Plasma adrenocorticotrophin concentration during induction of parturition by the intravascular infusion of physiological amounts of cortisol into the sheep foetus. J Physiol (Lond) 245:P76–P78
Author information
Authors and Affiliations
Additional information
Supported by United States Public Health Service Grant HL 35842.
Rights and permissions
About this article
Cite this article
Rudolph, A., Roman, C. & Gournay, V. Perinatal Myocardial DNA and Protein Changes in the Lamb: Effect of Cortisol in the Fetus. Pediatr Res 46, 141–146 (1999). https://doi.org/10.1203/00006450-199908000-00002
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199908000-00002
