
Abstract
Twenty children older than 2 y infected with human immunodeficiency virus (HIV) were examined by in vivo proton magnetic resonance spectroscopy (1H MRS) to study their cerebral metabolism and to identify metabolic profiles in relation with different stages of the disease. Patients were rated regarding their clinical and immunologic status according to the Centers for Disease Control classification and were divided into two groups: without encephalopathy (E-, n = 15) and with progressive encephalopathy (E+, n = 5). The acquisition was performed in the centrum semiovale using the short echo stimulated echo acquisition mode 20-ms sequence. The MRS profile was abnormal in all HIV-infected children compared with healthy age-matched controls (n = 7), even when magnetic resonance images were normal. A significant increase of the proportion of the lipid signals (ANOVA, p < 0.05) was found in all HIV-infected children. In addition, a significant decrease of the proportion of the N-acetylaspartate signal and a significant increase of the proportion of the myo-inositol signal (ANOVA, p < 0.05) characterized the E+ group. The principal component analysis performed on eight variables on 30 spectra confirms that the spectra of HIV-infected children differ from control spectra. The E+ group and the E- group are clearly separated on the map of subjects on the principal plane. The E- group lies in an intermediate position between the E+ group and the control group. The evolution of metabolic alterations in the brain of HIV-infected children can clearly be monitored by 1H MRS and associated with the occurrence of an encephalopathy.
Similar content being viewed by others


Main
The HIV displays both immunotropism and neurotropism. Mother-to-child transmission accounts for the most common mode of transmission of pediatric HIV infection (1). In children, the early invasion of the virus in the CNS of HIV-infected patients takes place during the development of the brain and during the process of myelination.
HIV-related encephalopathy occurs in more than 20% of the children with perinatally acquired AIDS, and the median age at diagnosis has been reported to be 19 mo (2). The most common form, the so-called "progressive encephalopathy," is characterized by a predominant motor syndrome with pyramidal tract anomalies, cognitive impairment, developmental retardation or regression, and ultimately spastic paraparesis. MR images classically show brain atrophy. Calcifications of basal ganglia and increased white matter signal in T2-weighted images have been described in relation with severe encephalopathy (3).
Localized brain 1H MRS is now accepted as a useful complementary tool in the evaluation of cerebral metabolism in various diseased or nondiseased states of the brain (4,5). Its interest has been clearly demonstrated in adult HIV-related encephalopathy in many reports (6–12). 1H MRS depicts reproducibly and reliably modifications of brain metabolism, which can be used for early diagnosis of HIV-related encephalopathy in adults. The same approach is expected to detect the onset of HIV progressive encephalopathy in children. A few studies have been performed using 1H MRS in children with AIDS to identify the modifications of brain metabolism occurring in basal ganglia (13,14) or in white matter (13,15).
We have examined by single voxel brain 1H MRS 20 HIV-infected children, mainly with a mother-to-child contamination, with or without HIV encephalopathy. The aim of this study is to identify metabolic profiles in relation with different stages of the disease with 1) the definition of a metabolic pattern of HIV-related encephalopathy in children to diagnose it at its onset, and 2) the characterization of the brain metabolic status of HIV-infected children without encephalopathy.
METHODS
Subjects. The study was conducted on 20 HIV-infected children (11 boys and 9 girls) and 7 healthy children (3 boys and 4 girls) constituting the control group. The children presented in this study were more than 2 y of age to avoid any interference with the metabolic consequences of physiologic myelination (16). All HIV children were infected during the perinatal period, 19 from mother-to-child transmission and 1 after a blood transfusion. Among the 19 mothers, 14 had a history of known i.v. drug abuse.
Clinical and immunologic data are summarized in Table 1 according to the classification of the Centers for Disease Control and Prevention (17). The clinical categories are n = no symptoms, A = mild symptoms, B = moderate symptoms, and C = severe symptoms. The immunologic categories are 1 = no evidence of immunosuppression, 2 = evidence of moderate immunosuppression, and 3 = severe immunosuppression. Moreover children have been classified in patients with (E+) and without (E-) encephalopathy. E+ children (n = 5) are categorized in the group C of the classification of the Centers for Disease Control and Prevention. Clinical, neurologic, and immunologic status were rated at the time of MRS. All children had antiretroviral therapy (zidovudine ± didanosine) at the time of the MRS examination. A second MRS examination was performed on patients 3, 5, and 20 1 y later. Five children (patients 1-5) had a severe progressive encephalopathy (E+) characterized by loss of previously acquired developmental milestones and symmetric motor deficits with spastic paresis.
Age was from 2 to 4.5 in the E+ group, from 2 to 9 in the E- group, and from 4.5 to 11 in the control group. Consequently, age matching is not perfect and the age of the control populations is statistically different. It was difficult to obtain spectra from younger control children without anesthesia, because of difficulties to sustain immobility. It was not possible to record spectra from anesthetized control children for obvious ethical reasons. All parents gave their informed consent in accordance to the local Ethics Committee guidelines.
MRI and localized 1H MRS. MR examination was conducted on a Siemens Magnetom SP63 (Erlangen, Germany) equipped with a 1.5-T magnet, at the Timone Hospital in Marseille. Anesthesia was induced in some patients to obtain MR examinations of good quality. When there was no anesthesia, an adult was attending with the child by the magnet during the acquisition to prevent any movement of his head. Standard spin-echo imaging was performed using a "turbo spin-echo" sequence (TE = 90 ms, TR = 4200 ms, slice thickness = 5 mm). 1H MRS was performed at 63 MHz using the STEAM sequence combined with a chemical shift selective excitation sequence to suppress the water signal, as described by Frahm et al. (18). The STEAM sequence was preferred because this sequence leads to a lower contamination from outer volumes than the point resolved spectroscopy sequence (19). Stimulated echo time was 20 ms, TR was 1500 ms, and a spectrum was acquired in 256 scans. The size of the volume of interest was 2 cm × 2 cm × 2 cm = 8 cm3. The volume of interest was always selected in the centrum semiovale. Spectra were recorded in the same location in control subjects. The total duration of the combined MRI-MRS exploration never exceeded 50 min.
Processing of spectra. All spectra were processed by two experienced spectroscopists following a standardized processing procedure based on the GIFA software (M. A. Delsuc, CBS, Faculté de Pharmacie, Montpellier, France) on a Silicon Graphics Indigo work station. After 4K zero-filling and gaussian filtering (2 Hz), the phase of the spectra was carefully corrected, and baseline was corrected manually (spline method using polynomial function between selected points). The areas of the MR signals were measured, and the resonances were assigned according to literature (20). The signal from lipids originating from outside the volume of interest could be identified, because it is usually in opposition of phase with the other signals. A great attention was paid to the quality of spectra. Spectra were carefully examined with regard to the water suppression, the signal-to-noise ratio, the phase of lipid resonance, and the half-height line width of the Cr-PCr resonance (which must be <5 Hz) to have the same quality of spectra in all groups. When spectra did not meet these requirements, they were eliminated.
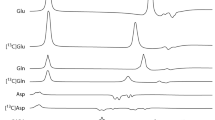
In the STEAM spectra with a 20-ms echo time (see Fig 1), the following signals were monitored: Ins (3.54 ppm), Tau (3.33 ppm), Cho (3.20 ppm), Cr-PCr (3.04 ppm), Glx (2.10-2.45 ppm), NAA (2.02 ppm), and Lip (between 1.9 and 0.2 ppm). The Cr-PCr signal at 3.04 ppm was used as an internal chemical shift reference. In the absence of automatic curve fitting, and because the high frequency parts of the NAA and Ins resonance overlap with resonances from other amino acids (Glx), we used the integration method described by Alger et al. (21) by beginning the integration at the top of the signal and continuing in the low frequency direction until the baseline was reached, and multiplying the result by two. The Glx signal was calculated by deducting the total NAA area resonance value from the area measured between 1.95 ppm and 2.45 ppm. The possible presence or absence of lactate (doublet with 7 Hz J-coupling centered at 1.33 ± 0.02 ppm) was carefully examined on each spectrum.

Brain proton MR spectra obtained in HIV-infected children. Brain proton MR spectra obtained on a Siemens Magnetom SP 63, using a STEAM sequence with a 20-ms stimulated echo time (TR = 1500 ms, spectroscopic volume of interest = 8 mL) in a control child (A) and in a child with a progressive HIV encephalopathy (patient 2a) (B).
We have chosen to use "relative quantitation," i.e. ratios of metabolite areas. The data are displayed as ratios (proportions) of the area of the signal of the Mi over the sum of signals of low molecular weight metabolites (S = Ins + Tau + Cho + Cr-PCr + Glx + NAA) as previously described in Confort-Gouny et al. (22). The quality of the spectra (water suppression, signal-to-noise ratio, half-height line width of the Cr-PCr resonance) was the same in patients and control subjects.
Statistical analysis. Two statistical analyses of data have been used, classical comparison of means of metabolite ratios and PCA. In classical statistical analysis, results are presented as means ± SD. Graphical description of statistical populations uses Tukey boxes. Each box summarizes the distribution of the statistical population in each group, displaying the median (with a confidence interval of 95%), the 25th and 75th percentiles, adjacent values, and outliers (23). Comparison of means was based on variance analysis (ANOVA) followed by a Fisher's test, after Bonferroni correction.
We have analyzed patients with abnormal spectra defined by Mi/S ratios measured with STEAM (TE, 20 ms) sequence. A spectrum was considered as abnormal when at least one ratio (NAA/S, Cho/S, Cr/S, Tau/S, Glx/S, Ins/S, Lip/S) was more or less than the limit values determined in the control group. To obtain a display of the metabolic profile of each patient, each value of his/her metabolic ratios is reported on a "simplified normal model spectrum" consisting of a diagram which includes seven histograms displaying the mean value and the lowest and highest values of each Mi/S ratio of the control group.
Data from spectra were also analyzed by a PCA package (STAT-I.T.C.F., Paris, France), as previously described by Confort-Gouny et al. (22). PCA is a method that looks for a few linear combinations which can capture simultaneous variations in many parameters, losing in the process as little information as possible. This method transforms the matrix of the n subjects with the p variables Xi, into a new matrix of n subjects with p new variables Zi. The PCA gives information about: 1) the correlation between the initial variables Xi (table of correlation coefficients); 2) the explained variance in the new reference system and the weight of each axis in the representation corresponding to the percentage of total variance. The first three axes must explain more than 50% of the total variance; 3) the coordinates of the variables Xi on the new axes (map of variables); and 4) the coordinates of each subjects in the new system of representation (map of subjects).
In this study, PCA was conducted on seven metabolic variables Ins/S, Tau/S, Cho/S, Cr-PCr/S, Glx/S, NAA/S, and Lip/S. Because age was significantly different between groups, it was also included as a variable to evaluate its potential impact.
RESULTS
In the five E+ patients, MR images of the brain showed mainly a moderate atrophy and nonspecific periventricular and deep white matter hyperintensities in T2-weighted images. No corticospinal tract degeneration was observed, and no specific alteration was present. In the other patients, MRI displayed nonspecific white matter hyperintensities or was normal (Table 1).
Figure 1 shows typical localized proton MR spectra recorded from a control child (A), and from a child with HIV progressive encephalopathy (patient 2) (B).
Mean metabolic variations in HIV-infected children population. All HIV-infected children (with or without progressive encephalopathy) displayed a significant increase of mean Lip/S value (8.4 ± 2.67 in E+ children, 7.09 ± 1.49 in E- children versus 5.07 ± 2.28 in control subjects, ANOVA, p = 0.02) (Fig. 2). This feature was detected in E- children whether or not there was a maternal history of drug abuse.

Mean values of NAA/S, Ins/S, and Lip/S in HIV-infected children. The mean values of the three metabolic ratios were calculated in brain MR spectra obtained in control subjects (n = 7), HIV-infected children without encephalopathy (n = 15), and HIV-infected children with with progressive encephalopathy (n = 5). Results are presented as Tukey boxes; mean and SD are indicated. Statistical significance is given with p ≤ 0.05.
E+ children displayed a significant decrease of the mean NAA/S value (21.25 ± 3.44 in E+ children, versus 28.95 ± 3.38 in E- children and 29.84 ± 3.61 in control subjects, ANOVA, p = 0.0004) (Fig. 2) versus control subjects. The mean Ins/S value was significantly increased in E+ children when compared with control subjects and with E- children (16.08 ± 1.86 in E+ children versus 12.86 ± 2.49 in E- children and 11.12 ± 3.04 in control subjects, ANOVA, p = 0.01). Neither the mean Cho/S nor Glx/S ratios were significantly modified in children with encephalopathy. In HIV-infected E- children, the mean Ins/S and NAA/S (Fig. 2) values were not different from the values obtained in the control population.
Table 2 displays the values of the main metabolic ratios in children according to their immunologic grading. E+ children were removed to eliminate any interference with the occurrence of encephalopathy and to evaluate a possible effect of the immunosuppression itself on brain metabolism. Children from groups 2 and 3 were pooled to perform a statistical analysis. Both children with and without immunosuppression displayed a significant increase of mean Lip/S value.
When patients were classified according to their clinical grading, no additional information was obtained because of the small size of the clinical groups, and because E+ patients were obviously all in group C. One could only observe that, in infected patients, the Lip/S value was always increased with statistical significance (p ≤ 0.01) with respect to control children (n = 7, 5.07 ± 2.28); children with no symptoms (n = 3, 6.87 ± 1.42), children with mild symptoms (n = 6, 7.59 ± 1.82), children with moderate symptoms (n = 3, 7.09 ± 1.80), and children with severe symptoms (n = 8, 7.62 ± 2.31).
Individual variations of brain metabolism in HIV-infected children. When each spectrum was individually analyzed and positioned on the diagram of the simplified normal model spectrum (histogram), it appears that all HIV-infected children (E+ and E-) displayed an abnormal spectrum with an increase or a decrease out of the limit values of one or more Mi/S ratios (Fig. 3). The most frequent modifications of the spectrum were the increase of Lip/S ratio (23/23) and the decrease of NAA signal (12/23). There was no signal from lactate on the spectra. Figure 3 displays the metabolic profiles of two E+ patients (patients 2 and 3a).

Individual metabolic profiles of two HIV-infected E+ children. Values of the metabolic ratios of patients are reported on a "simplified normal model spectrum," used as a reference, which includes seven histograms displaying the mean values and the lowest and highest values of each Mi/S ratio of the control group. ▪, patient 2; □, patient 3a.
Multivariate analysis. The processing of metabolic variables by PCA yields the contribution of each variable to each axis. The total variance explained by the first three axes was 70.7%. The most contributing variables to axis 1 were NAA/S (-0.86), age (-0.80), Ins/S (0.65), and Lip/S (0.65). The most contributing variables to axis 2 were Cho/S (0.83) and Glx/S (-0.74). The numbers in parentheses are the correlation of variables to the axes, expressed in arbitrary units. There was no significant correlation between metabolic variables. Figure 4 (inset) displays the map of variables on the principal plane (axes 1 and 2).

PCA of data obtained from MR spectra. Map of subjects of PCA performed on 30 brain localized MR from 20 HIV-infected children and 7 control subjects. Each point corresponds to a proton MR spectrum. Only the first PCA plane (axis 1-axis 2) is presented. The circle of variables is presented above the map of subjects. ○, controls; □, HIV-infected E- children, and ▪, HIV-infected E+ children.
The analysis of the 30 observations (spectra) demonstrated that the spectra of HIV-infected children differed from those recorded in control subjects. All spectra from E+ children were clearly separated from both control subjects and children without encephalopathy. The E+ group is located mainly along the Ins and Lip axes, whereas the control group is along the NAA axis. The E- group lies in an intermediate position between the E+ group and the control group.
DISCUSSION
All HIV-infected children displayed an abnormal MRS examination even when MRI was normal or when there were no specific modifications of signal on T2-weighted images. The results obtained with classical statistical analyses on HIV-infected children are in agreement with the results of the PCA, validating the use of multivariate analyses as previously reported in other diseases (22,24). The main results of this study are: 1) the detection of brain metabolic anomalies in HIV-infected children even when there is no encephalopathy, and 2) the finding of a typical metabolic profile of progressive encephalopathy characterized by a decrease of NAA/S ratio and an increase of Ins/S and Lip/S ratios.
MRS in HIV-infected children without encephalopathy. A striking result is that E- children display an abnormal brain MRS profile. Metabolic anomalies have already been reported in HIV-infected children without encephalopathy (14) but the MRS examination was performed using long echo sequences (TE = 136 ms), which are less informative. The increased Lip/S ratio seems to be related to HIV infection and not to drug exposure during pregnancy, because there is no significant difference between the group of E- children with drug exposure and the group of E- children with no drug exposure.
HIV infection induces metabolic modifications of brain parenchyma. The metabolic profile is characterized by an increase of the proportion of the Lip signal on the spectra. The E- group is located on the PCA map in an intermediary position between the control group and the E+ group. The apparent dispersion of the E- subjects on the PCA map can be explained by the variety of the individual metabolic profiles. HIV infection in children seems to be characterized by an increased Lip/S ratio. Because this increase is not accompanied by an abnormal choline signal, the hypothesis of a demyelination can be ruled out. One has to keep in mind that the "Lip" signal is a broad resonance assigned to lipids and/or proteins. The augmentation of this signal might be in relation to the presence of the virus in the brain during development, leading to a disorganization of the proteo-lipidic structure of the brain.
In adults, no such significant increase of the Lip signal has been found in neuroasymptomatic HIV-infected patients using the same STEAM sequence on the same equipment under the same conditions (12). The MRS anomalies found in children might well reflect the presence of the virus in brain parenchyma during maturation.
A typical metabolic profile associated with progressive encephalopathy. The brain metabolic profile of children of the E+ group includes the anomalies detected in the E- group (i.e. increased Lip/S ratio) and is additionally characterized by an increased Ins/S ratio and a decreased NAA/S ratio. This metabolic profile is in relation with the neurologic defects and not with the clinical or immunologic status, because 1) patients in the same clinical or immunologic category do not constitute a separate set in the PCA and 2) there are no significant modifications of Ins/S and/or NAA/S ratios in children with moderate or severe immunosuppression (cf. Table 2). A previous study (13) has reported that the MRS anomalies observed in HIV-infected children were not related to the CD4 lymphocyte count. It is a constant, but not surprising, observation, already made in adults (9,12), that the metabolic status of the brain is not simply related to variations of the peripheral lymphocyte functions. The metabolic variations observed in children with progressive HIV encephalopathy explain the location of the E+ group at the right of the subjects map in the PCA, clearly separated from the E- group. Although the effect of age cannot be totally ruled out, its own impact cannot explain the position of the subjects on the map. For example, patients 12 and 13 (E- patients, respectively, 2 and 3 y old) are closer to the control group than patients 2 and 3 (E+ patients, age 4). Moreover, the literature describes that the most significant changes in metabolites occur before the age of 2 (16).
Reduced NAA signal has already been described in progressive HIV encephalopathy (13,14). The intensity of the NAA resonance is known to be low during the first year of life (16). Because this study was conducted on children older than 2 y, the low NAA values cannot be related to the physiologic myelination process. Delayed myelination can be ruled out because the choline signal is not modified in these children, and MRI results do not evoke delayed myelination. A reduced NAA proportion in the spectrum can be rather related to neuronal suffering (5), taking into consideration the pathogenesis of progressive HIV encephalopathy characterized by apoptotic neurons (25).
Ins is exclusively present in glial cell cultures (26) and is assumed to be a glial marker (27). Increased Ins has previously been reported in the literature in diseases where glial activation occurs (12,28,29). Inasmuch as astrocytes have been described as a reservoir for HIV in the CNS of children with AIDS-associated leukoencephalopathy (30), the increased Ins signal in the E+ group might reflect the metabolic activation of the glial cells.
An increased Ins signal and decreased NAA signal are detected in adults with HIV-related encephalopathy (12,29) and are in relation to the occurrence of HIV-related encephalopathy. Despite the differences between the clinical manifestations observed in adults and in children (1), the occurrence of HIV encephalopathy is characterized by the same metabolic anomalies on short echo sequences.
In conclusion, in HIV-infected children older than 2 y, brain metabolism is always affected, in spite of a normal clinical examination and/or normal (or subnormal) MR images. These modifications are characterized by an increase of brain lipids. When a progressive encephalopathy occurs, additional modifications are detected including a decrease of NAA signal and an increase of the Ins signal. At the present time, we have not enough follow-up studies to describe the early variations of brain metabolism at the onset of a progressive encephalopathy. However, the clinicians have to be aware of the fact that brain metabolism of HIV-infected children is not normal even in the asymptomatic phase of the HIV brain infection. Our results advocate the use of brain MRS to follow-up HIV-infected children to monitor the efficacy of new or existing drugs.
Abbreviations
- Cho:
-
choline-containing compounds
- Cr-PCr:
-
creatine/phosphocreatine
- E-:
-
without encephalopathy
- E+:
-
with progressive encephalopathy
- Glx:
-
glutamate-glutamine
- 1H MRS:
-
proton magnetic resonance spectroscopy
- Ins:
-
myo-inositol
- Lip:
-
lipids and/or proteins
- MR:
-
magnetic resonance
- MRI:
-
magnetic resonance imaging
- Mi:
-
metabolite of interest
- NAA:
-
N-acetylaspartate
- PCA:
-
principal component analysis
- S:
-
sum of signals of low molecular weight metabolites
- STEAM:
-
stimulated echo acquisition mode
- Tau:
-
taurine and/or scyllo-inositol
- TE:
-
echo time
- TR:
-
repetition time
References
Mintz M 1994 Clinical comparison of adult and pediatric neuroAIDS. Adv Neuroimmunol 4: 207–221
Lobato MN, Caldwell MB, Ng P, Oxtoby MJ 1995 The pediatric spectrum of disease clinical consortium. Encephalopathy in children with perinatally acquired human immunodeficiency virus infection. J Pediatr 126: 710–715
Burns DK 1992 The neuropathology of pediatric acquired immunodeficiency syndrome. J Child Neurol 7: 332–346
Ross B, Kreis R, Ernst T 1992 Clinical tools for the 90s: magnetic resonance spectroscopy and metabolite imaging. Eur J Radiol 14: 128–140
Vion-Dury J, Meyerhoff DJ, Cozzone PJ, Weiner MW 1994 What might be the impact on neurology of the analysis of brain metabolism by in vivo magnetic resonance spectroscopy? J Neurol 241: 354–371
Chong WK, Sweeney B, Wilkinson ID, Paley M, Hall-Craggs MA, Kendall BE, Shepard JK, Beecham M, Miller RF, Weller IVD, Newman SP, Harrison MJG 1993 Proton spectroscopy of the brain in AIDS infection: correlation with clinical, immunologic and MR imaging findings. Radiology 188: 119–124
Meyerhoff DJ, McKay S, Bachman L, Poole N, Dillon WP, Weiner MW, Fein G 1993 Reduced brain N-acetylaspartate suggests neuronal loss in cognitively impaired human immunodeficiency virus-seropositive individuals. In vivo1H magnetic resonance spectroscopic imaging. Neurology 43: 509–515
Vion-Dury J, Confort-Gouny S, Nicoli F, Dhiver C, Gastaut JA, Gastaut JL, Cozzone PJ 1994 Localized brain proton MRS metabolic patterns in AIDS-related encephalopathies. CR Acad Sci (Paris) 317: 833–840
Chang L, Miller BL, McBride D, Cornford M, Oropilla G, Buchtal S, Chiang F, Aronow H, Ersnt T 1995 Brain lesions in patients with AIDS: 1H MR spectroscopy. Radiology 197: 525–531
Paley M, Cozzone PJ, Alonso J, Vion-Dury J, Confort-Gouny S, Wilkinson ID, Chong WK, Hall-Craggs M, Harrison MJG, Gili J, Rovira A, Cappellades J, Rio J, Ocana I, Nicoli F, Dhiver C, Gastaut JL, Gastaut JA, Wicklow K, Sauter R 1996 A multicenter proton magnetic resonance spectroscopy study of neurological complications of AIDS. AIDS Res Hum Retroviruses 12: 213–222
Salvan AM, Vion-Dury J, Confort-Gouny S, Nicoli F, Lamoureux S, Cozzone PJ 1997 Brain proton MR spectroscopy in HIV-related encephalopathy. Identification of evolving metabolic patterns in relation to dementia and therapy. AIDS Res Hum Retroviruses 13: 1055–1066
Salvan AM, Vion-Dury J, Confort-Gouny S, Nicoli F, Lamoureux S, Cozzone PJ 1997 Cerebral metabolic alterations in HIV-related encephalopathy detected by brain proton MR spectroscopy: comparison between sequences using short and long echo times. Invest Radiol 32: 485–495
Pavlakis SG, Lu D, Frank Y, Bakshi S, Pahwa S, Barnett TA, Porricolo ME, Gould RJ, Nozyce ML, Hyman RA 1995 Magnetic resonance spectroscopy in childhood AIDS encephalopathy. Pediatr Neurol 12: 277–282
Dongfeng L, Pavlakis SG, Frank Y, Bakshi S, Pahwa S, Gould RJ, Sison C, Hsu C, Lesser M, Hoberman M, Barnett T, Hyman RA 1996 Proton MR spectroscopy of the basal ganglia in healthy children and children with AIDS. Radiology 199: 423–428
Vion-Dury J, Nicoli F, Salvan AM, Confort-Gouny S, Lamoureux S, Dhiver C, Gastaut JA, Gastaut JL, Michel G, Cozzone PJ 1996 >Why do clinicians effectively need localized brain proton MRS in HIV related encephalopathies? In: Podo F, Bovée WMMJ, De Certaines JD, Henriksen O, Leach MO, Leibfritz D (eds) Eurospin Annual 1995-1996. Instituto Superiore di Sanita, Roma, Italy, pp 369–385
Van der Knaap MS, Valk J 1995 Magnetic Resonance of Myelin, Myelination, and Myelin Disorders. Springer, Berlin, pp 445–456.
Centers for Disease Control and Prevention 1994 Revised classification system for human immunodeficiency virus infection in children less than 13 years of age. MMWR 43: 1–10
Frahm J, Bruhn H, Gyngell ML, Merboldt KD, Hänicke W, Sauter R 1989 Localized high-resolution proton NMR spectroscopy using stimulated echoes: initial application to human brain in vivo. Magn Reson Med 9: 79–93
Yongbi NM, Payne GS, Collins DJ, Leach MO 1995 Quantification of signal selection efficiency, extra volume suppression and contamination for ISI, STEAM and PRESS localized 1H NMR spectroscopy using an EEC localization test object. Phys Med Biol 40: 1293–1303
Michaelis T, Merboldt KD, Hänicke W, Gyngell ML, Bruhn H, Frahm J 1991 On the identification of cerebral metabolites in localized 1H NMR spectra of human brain in vivo. NMR Biomed 4: 90–98
Alger JR, Symko SC, Bizzi A, Posse S, DesPres DJ, Amstrong MR 1993 Absolute quantitation of short TE brain H1-MR spectra and spectroscopic imaging data. J Comput Assist Tomogr 17: 191–199
Confort-Gouny S, Vion-Dury J, Nicoli F, Dano P, Donnet A, Grazziani N, Gastaut JL, Grisoli F, Cozzone PJ 1993 A multiparametric data analysis showing the potential of localized proton MR spectroscopy of the brain in the metabolic characterization of neurological diseases. J Neurol Sci 118: 123–133
Cleveland S, McGill R 1983 Graphical perception and graphical methods for analyzing scientific data. Science 229: 828–833
Chabrol B, Salvan AM, Confort-Gouny S, Vion-Dury J, Cozzone PJ 1995 Localized proton magnetic resonance spectroscopy differentiates the inborn metabolic encephalopathies in children. CR Acad Sci (Paris) 318: 985–92
Gelbard HA, James HJ, Sharer LR, Perry SW, Saito Y, Kazee AM, Blumberg BM, Epstein LG 1995 Apoptotic neurons in brains from paediatric patients with HIV-1 encephalitis and progressive encephalopathy. Neuropathol Appl Neurobiol 21: 208–217
Brand A, Richter-Landsberg C, Leibfritz D 1993 Multinuclear NMR studies on the energy metabolism of glial and neuronal cells. Dev Neurosci 15: 289–298
Kauppinen RA 1993 1H Nuclear magnetic resonance spectroscopy identifies neural cell types: a promising step for neuroimaging? Trends Neurosci 16: 384–386
Moats RA, Ernst T, Shonk TK, Ross BD 1994 Abnormal cerebral metabolite concentrations in patients with probable Alzheimer disease. Magn Reson Med 32: 110–115
Laubenberger J, Häussinger D, Bayer S, Thielemann S, Schneider B, Mundinger A, Hennig J, Langer M 1996 HIV-related metabolic abnormalities in the brain: depiction with proton MR spectroscopy with short echo times. Radiology 199: 805–810
Tornatore C, Chandra R, Berger JR, Major EO 1994 HIV-1 infection of subcortical astrocytes in the pediatric central nervous system. Neurology 44: 481–487
Author information
Authors and Affiliations
Additional information
Supported by CNRS (UMR 6612), AP-HM (Assistance Publique Hôpitaux de Marseille), the Programme Hospitalier de Recherche Clinique (Ministère de la Santé), the Agence Nationale contre le SIDA (ANRS), and Sidaction (Ensemble Contre le SIDA).
Rights and permissions
About this article
Cite this article
Salvan, AM., Lamoureux, S., Michel, G. et al. Localized Proton Magnetic Resonance Spectroscopy of the Brain in Children Infected with Human Immunodeficiency Virus with and without Encephalopathy. Pediatr Res 44, 755–762 (1998). https://doi.org/10.1203/00006450-199811000-00019
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199811000-00019
This article is cited by
-
Case control study: magnetic resonance spectroscopy of brain in HIV infected patients
BMC Neurology (2016)
-
Neuropsychological Function and Cerebral Metabolites in HIV-infected Youth
Journal of Neuroimmune Pharmacology (2012)
-
The Role of Medical Imaging in Defining CNS Abnormalities Associated with HIV-Infection and Opportunistic Infections
Neurotherapeutics (2011)
