
Abstract
Background:
To examine changes to whole body and regional lean mass (LM) and fat mass (FM) over 33 months of intermittent androgen suppression therapy (IAST).
Methods:
Phase II cohort study of 72 prostate cancer patients without metastatic bone disease. Patients received flutamide 250 mg tid and leuprolide 22.5 mg three monthly depot for the 9-month initial treatment phase (iTREAT), at which point patients ceased therapy providing PSA <4 ng ml−1 with continued monitoring for further 2 years (POST). AST was recommenced when PSA exceeded pretreatment level or ⩾20 ng ml−1. Body composition was assessed using dual energy X-ray absorptiometry at baseline, completion of treatment phase, and 1 and 2 years post treatment phase (months 21 and 33).
Results:
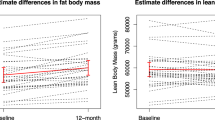
LM decreased by 1.3 kg and FM increased by 2.3 kg (P<0.001) following iTREAT. During the POST period, there were no further adverse effects on LM or FM, but also no recovery to pretreatment levels. Patients who failed to recover testosterone by month 33 experienced a significant increase in FM compared with those who recovered eugonadal levels of testosterone (10 nmol ml−1; P=0.019). Change in testosterone was moderately correlated to changes in % FM (r=−0.314, P<0.028) and LM (r=0.300, P<0.036) during POST phase. Waist circumference progressively increased over time and by 2 years, POST had not recovered to baseline levels.
Conclusions:
Loss of LM and gain in FM during the 9-month iTREAT was not reversed during 2-year POST, although further deterioration was not observed. Subgroup analysis identified those recovering testosterone showed some body composition improvements. These findings suggest potential benefits of IAST, where testosterone levels are able to recover, to reduce the ongoing adverse effects on body composition, such as the acceleration of sarcopenia and risks associated with metabolic disease.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Moyad MA . Promoting general health during androgen deprivation therapy (ADT): a rapid 10-step review for your patients. Urol Oncol 2005; 23: 56–64.
Shahinian VB, Kuo YF, Freeman JL, Goodwin JS . Risk of the ‘androgen deprivation syndrome’ in men receiving androgen deprivation for prostate cancer. Arch Intern Med 2006; 166: 465–471.
Kaisary AV . Evaluating the use of early hormonal therapy in patients with localised or locally advanced prostate cancer. Prostate Cancer Prostatic Dis 2005; 8: 140–151.
McCredie M, Cox B . Prostate-specific antigen testing for prostate cancer: the case for informed consent. Med J Aust 1998; 169: 9–10.
Moul JW . Prostate specific antigen only progression of prostate cancer. J Urol 2000; 163: 1632–1642.
Diamond TH, Higano CS, Smith MR, Guise TA, Singer FR . Osteoporosis in men with prostate carcinoma receiving androgen-deprivation therapy: recommendations for diagnosis and therapies. Cancer 2004; 100: 892–899.
Levine GN, D'Amico AV, Berger P, Clark PE, Eckel RH, Keating NL et al. Androgen-deprivation therapy in prostate cancer and cardiovascular risk: a science advisory from the American Heart Association, American Cancer Society, and American Urological Association: endorsed by the American Society for Radiation Oncology. Circulation 2010; 121: 833–840.
Keating NL, O'Malley AJ, Smith MR . Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J Clin Oncol 2006; 24: 4448–4456.
Smith MR, Finkelstein JS, McGovern FJ, Zietman AL, Fallon MA, Schoenfeld DA et al. Changes in body composition during androgen deprivation therapy for prostate cancer. J Clin Endocrinol Metab 2002; 87: 599–603.
Tunio MA, Rafi M, Qayyum A, Hashmi A . Androgen deprivation therapy increases the risk of diabetes and non- cancer mortality in prostate cancer patients: a meta-analysis. J Diabetol 2010; 2.
Loblaw DA, Mendelson DS, Talcott JA, Virgo KS, Somerfield MR, Ben-Josef E et al. American Society of Clinical Oncology recommendations for the initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer. J Clin Oncol 2004; 22: 2927–2941.
Sato N, Akakura K, Isaka S, Nakatsu H, Tanaka M, Ito H et al. Intermittent androgen suppression for locally advanced and metastatic prostate cancer: preliminary report of a prospective multicenter study. Urology 2004; 64: 341–345.
Spry NA, Kristjanson L, Hooton B, Hayden L, Neerhut G, Gurney H et al. Adverse effects to quality of life arising from treatment can recover with intermittent androgen suppression in men with prostate cancer. Eur J Cancer 2006; 42: 1083–1092.
Rosenberg IH . Sarcopenia: origins and clinical relevance. J Nutr 1997; 127 (Suppl): 990S–991S.
Galvao DA, Spry NA, Taaffe DR, Newton RU, Stanley J, Shannon T et al. Changes in muscle, fat and bone mass after 36 weeks of maximal androgen blockade for prostate cancer. BJU Int 2008; 102: 44–47.
Haseen F, Murray LJ, Cardwell CR, O'Sullivan JM, Cantwell MM . The effect of androgen deprivation therapy on body composition in men with prostate cancer: systematic review and meta-analysis. J Cancer Surviv 2010; 4: 128–139.
Tsai HK, D'Amico AV, Sadetsky N, Chen MH, Carroll PR . Androgen deprivation therapy for localized prostate cancer and the risk of cardiovascular mortality. J Natl Cancer Inst 2007; 99: 1516–1524.
Saigal CS, Gore JL, Krupski TL, Hanley J, Schonlau M, Litwin MS . Androgen deprivation therapy increases cardiovascular morbidity in men with prostate cancer. Cancer 2007; 110: 1493–1500.
D'Amico AV, Denham JW, Crook J, Chen MH, Goldhaber SZ, Lamb DS et al. Influence of androgen suppression therapy for prostate cancer on the frequency and timing of fatal myocardial infarctions. J Clin Oncol 2007; 25: 2420–2425.
Shaw GL, Wilson P, Cuzick J, Prowse DM, Goldenberg SL, Spry NA et al. International study into the use of intermittent hormone therapy in the treatment of carcinoma of the prostate: a meta-analysis of 1446 patients. BJU Int 2007; 99: 1056–1065.
Taaffe DR, Lewis B, Marcus R . Quantifying the effect of hand preference on upper limb bone mineral and soft tissue composition in young and elderly women by dual-energy X-ray absorptiometry. Clin Physiol 1994; 14: 393–404.
Heymsfield SB, Smith R, Aulet M, Bensen B, Lichtman S, Wang J et al. Appendicular skeletal muscle mass: measurement by dual-photon absorptiometry. Am J Clin Nutr 1990; 52: 214–218.
Scafoglieri A, Provyn S, Wallace J, Louis O, Tresignie J, Bautmans I et al. Whole body composition by Hologic QDR 4500/A DXA: system reliability versus user accuracy and precision. In: Ivanov O (ed) Applications and Experiences of Quality Control. CC BY-NC-SA, 2011.
Evans DJ, Hoffmann RG, Kalkhoff RK, Kissebah AH . Relationship of androgenic activity to body fat topography, fat cell morphology, and metabolic aberrations in premenopausal women. J Clin Endocrinol Metab 1983; 57: 304–310.
Lohman T, Roche A, Martorell R . Anthropometrics Standardzation Reference Manual. Human Kinetic Books: Champagne, Illinois, 1988.
Björntorp P . Fat cell distribution and metabolism. Annals of the New York Academy of Sciences 1987; 499: 66–72.
Consultation We. Waist Circumference and Waist-Hip Ratio: report of a WHO expert consultation: Geneva, 2008.
Spry NA, Galvao DA, Davies R, La Bianca S, Joseph D, Davidson A et al. Long-term effects of intermittent androgen suppression on testosterone recovery and bone mineral density: results of a 33-month observational study. BJU Int 2009; 104: 806–812.
Greenspan SL, Coates P, Sereika SM, Nelson JB, Trump DL, Resnick NM . Bone loss after initiation of androgen deprivation therapy in patients with prostate cancer. J Clin Endocrinol Metab 2005; 90: 6410–6417.
Smith MR . Changes in fat and lean body mass during androgen-deprivation therapy for prostate cancer. Urology 2004; 63: 742–745.
Levy ME, Perera S, van Londen GJ, Nelson JB, Clay CA, Greenspan SL . Physical function changes in prostate cancer patients on androgen deprivation therapy: a 2-year prospective study. Urology 2008; 71: 735–739.
See R, Abdullah SM, McGuire DK, Khera A, Patel MJ, Lindsey JB et al. The association of differing measures of overweight and obesity with prevalent atherosclerosis: the Dallas Heart Study. J Am Coll Cardiol 2007; 50: 752–759.
Executive Summary of The Third report of the National Cholesterol Education Program (NCEP). Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Jama 2001; 285: 2486–2497.
Braga-Basaria M, Dobs AS, Muller DC, Carducci MA, John M, Egan J et al. Metabolic syndrome in men with prostate cancer undergoing long-term androgen-deprivation therapy. J Clin Oncol 2006; 24: 3979–3983.
Galvao DA, Taaffe DR, Spry N, Newton RU . Exercise can prevent and even reverse adverse effects of androgen suppression treatment in men with prostate cancer. Prostate Cancer Prostatic Dis 2007; 10: 340–346.
Galvao DA, Nosaka K, Taaffe DR, Peake J, Spry N, Suzuki K et al. Endocrine and immune responses to resistance training in prostate cancer patients. Prostate Cancer Prostatic Dis 2008; 11: 160–165.
Galvao DA, Nosaka K, Taaffe DR, Spry N, Kristjanson LJ, McGuigan MR et al. Resistance training and reduction of treatment side effects in prostate cancer patients. Med Sci Sports Exerc 2006; 38: 2045–2052.
Galvao DA, Taaffe DR, Spry N, Joseph D, Newton RU . Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: a randomized controlled trial. J Clin Oncol 2010; 28: 340–347.
Galvao DA, Taaffe DR, Spry N, Joseph D, Newton RU . Acute versus chronic exposure to androgen suppression for prostate cancer: impact on the exercise response. J Urol 2011; 186: 1291–1297.
Galvao DA, Newton RU, Taaffe DR, Spry N . Can exercise ameliorate the increased risk of cardiovascular disease and diabetes associated with ADT? Nat Clin Pract Urol 2008; 5: 306–307.
Helmrich SP, Ragland DR, Leung RW, Paffenbarger RS . Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 1991; 325: 147–152.
Baker MK, Simpson K, Lloyd B, Bauman AE, Singh MA . Behavioral strategies in diabetes prevention programs: a systematic review of randomized controlled trials. Diabetes Res Clin Pract 2011; 91: 1–12.
Acknowledgements
We would like to thank Abbott Australasia and Schering-Plough for their financial support in running the study. DAG is funded by a Movember New Directions Development Award obtained through Prostate Cancer Foundation of Australia’s Research Program. We would also like to thank the Genito Urinary Oncology Group NSW and Urology Research Centre Perth for their support and direction, Spry JI and Leutenegger S (Perth) for data management and additional analysis, and the following doctors from Perth who contributed patients to the study: Joseph D, Rowling C, Stanley J, Low A, Vivian J, Cassidy B, Chelvanayagam D, Davies R, Harper CS, Hill I, La Bianca S, Mander J, McRae P, Shannon T and Weinstein S.
Clinical Trial Registry: a phase II study to assess the effect of intermittent androgen blockade in the treatment of advanced prostate cancer; ACTRN12608000170325; http://www.ANZCTR.org.au/ACTRN12608000170325.aspx
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Spry, N., Taaffe, D., England, P. et al. Long-term effects of intermittent androgen suppression therapy on lean and fat mass: a 33-month prospective study. Prostate Cancer Prostatic Dis 16, 67–72 (2013). https://doi.org/10.1038/pcan.2012.33
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2012.33
Keywords
This article is cited by
-
A randomized controlled trial comparing changes in fitness with or without supervised exercise in patients initiated on enzalutamide and androgen deprivation therapy for non-metastatic castration-sensitive prostate cancer (EXTEND)
Prostate Cancer and Prostatic Diseases (2022)
-
The effect of exercise training on cardiometabolic health in men with prostate cancer receiving androgen deprivation therapy: a systematic review and meta-analysis
Prostate Cancer and Prostatic Diseases (2021)
-
Efficacy of a multi-component exercise programme and nutritional supplementation on musculoskeletal health in men treated with androgen deprivation therapy for prostate cancer (IMPACT): study protocol of a randomised controlled trial
Trials (2017)
-
Lifestyle guidelines for managing adverse effects on bone health and body composition in men treated with androgen deprivation therapy for prostate cancer: an update
Prostate Cancer and Prostatic Diseases (2017)
-
Exercise medicine for prostate cancer
European Review of Aging and Physical Activity (2013)
