
Abstract
Youth with diabetes are at an increased risk of cardiovascular disease (CVD). Adherence to the Dietary Approaches to Stop Hypertension (DASH) diet has been shown to improve CVD risk. In this study, we evaluated whether changes in diet quality as characterized by DASH are associated with changes in CVD risk factors in youth with diabetes over time. Longitudinal mixed models were applied to data from 797 participants in the SEARCH for Diabetes in Youth Study representing three time points: baseline, 12- and 60-month follow-up. Data were restricted to youth whose diabetes was first diagnosed in 2002–2005. DASH-related adherence was poor and changed very little over time. However, an increase in DASH diet score was significantly associated with a decrease in HbA1c levels in youth with type 1 diabetes (β=−0.20, P-value=0.0063) and a decrease in systolic blood pressure among youth with type 2 diabetes (β=−2.02, P-value=0.0406). Improvements in dietary quality may be beneficial in youth with type 1 or type 2 diabetes. However, further work in larger groups of youth with type 1 and 2 diabetes is desirable.
Similar content being viewed by others
Introduction
Observational studies and clinical trials have shown that adherence to the Dietary Approaches to Stop Hypertension (DASH) diet is associated with improved cardiovascular health and cardiovascular disease (CVD) risk in adults and youth.1, 2, 3, 4 Youth with diabetes are at an increased risk of developing CVD.5 In a cross-sectional analysis, the SEARCH for Diabetes in Youth Study (SEARCH) previously reported that consumption of a more DASH-like diet was inversely related to CVD risk factors including hypertension, total cholesterol, low-density lipoprotein, low-density lipoprotein/high-density lipoprotein ratio and hemoglobin A1c (HbA1c).6, 7 The DASH diet emphasizes fruits, vegetables, low-fat milk products, whole grains, fish/poultry/nuts, lean red meats and limited intake of sugar and sweets, resulting in low-saturated fat, cholesterol, total fat and sodium intake.8 Thus, good adherence to the diet plan equates to a higher dietary quality. A few studies have examined the association of a DASH-like diet and hypertension in youth and adolescents;7, 9, 10, 11 however, no study has examined several CVD risk factors and DASH prospectively in youth with or without diabetes. This study investigated whether change in a DASH diet score was associated with change in CVD risk over multiple time points.
Methods
SEARCH is an ongoing multicenter study of physician-diagnosed diabetes mellitus in youth aged <20 years at diagnosis beginning in 2001. Study design details have been published.12 The study has been approved by all participating local institutional review boards. The sample included data from an initial (baseline) visit and two subsequent follow-up visits targeting 12 and 60 months. Follow-up visits were, on average, 14.7 months after the initial visit (s.d.=3.1 months; range=6–26 months) and 62.9 months (6.3 months; range=29–87 months), respectively.
Data collection followed SEARCH standardized protocols.6, 7, 12 Cardiovascular risk measures included diastolic blood pressure (BP), systolic BP, HDL, low-density lipoprotein, total cholesterol, triglycerides, HbA1c, waist circumference and body mass index calculated as weight per height2 (kg m−2) and converted to body mass index-Z score.6 DASH adherence was assessed with an index score ranging from 0 to 80 comprised of the sum of meeting recommendations on eight food groups (grains, vegetables, fruits, dairy, meat, nuts/seeds/legumes, fats/oils and sweets) based on the SEARCH 85-item food frequency questionnaire.6, 7 A maximum score of 10 could be achieved for each food group when the intake met the recommendation and lower intakes were scored proportionally. Previous reports describe diet intake according to DASH food groups and illustrate the scoring algorithm.6, 7 Food groups were created by either collapsing food items on the basis of their major components or by disaggregating composite foods into constituent foods. Duration of diabetes, age, gender, race/ethnicity, income, study site, height, weight, waist circumference and physical activity was also obtained for each participant based on SEARCH protocols.6, 7, 12
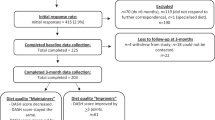
This analysis was restricted to youth whose diabetes was first diagnosed in 2002–2005, were ⩾10 years of age (n=1386), had diabetes for at least 6 months at their initial visit (n=1014) and had completed a baseline food frequency questionnaire. Of the 969 participants who met these criteria, youth were also excluded sequentially for missing CVD-related measures (n=130) and those fasting <8 h at any visit (n=42).
The final sample consisted of 797 participants. Of the 617 youth with type 1 diabetes, 278 had a complete 12-month follow-up visit (i.e. including diet information) and 231 had a complete 60-month follow-up visit. A total of 65 and 53 participants, respectively, had complete follow-up visits of the 180 youth with type 2 diabetes.
Statistical analyses
Statistical analyses were conducted using SAS 9.2 (SAS Institute, Cary, NC, USA) stratified by diabetes type. Longitudinal mixed-models with a random intercept to account for within-subject dependence were used to assess the relationship between the DASH diet score and CVD risk factors. Available CVD risk factor measurements were modeled as a function of baseline DASH score and change in DASH from baseline; these two captured the relationship between DASH score at baseline and the outcome as well as whether a change in DASH score was associated with the outcome longitudinally. Each model also adjusted for age, disease duration, race/ethnicity, sex, study site, income, height, body mass index-Z score and waist circumference.
Results
Mean values of CVD risk factors and change in DASH diet score are shown by visit and diabetes type in Table 1. Dietary quality at baseline was poor with a mean of 39.8 (s.d.=9.0) for youth with type 1 diabetes and 36.4 (s.d.=9.6) for youth with type 2 diabetes. Additionally, DASH score did not appear to change systematically over time, with a mean change of -0.18 (s.d.=10.1), for follow-up visit 1 and −0.41 (s.d.=11.2) for follow-up visit 2 in youth with type 1 diabetes. In youth with type 2 diabetes, the overall mean change in DASH score was also small, with -0.36 (s.d.=10.7) at follow-up visit 1 and 1.99 (s.d.=11.4) at follow-up visit 2. Several CVD risk factors increased over time in youth with type 1 diabetes, including BP, total cholesterol, triglycerides and HbA1c levels. HDL and HbA1c also significantly increased over time in youth with type 2 diabetes.
For each risk factor, Table 2 displays the results of the longitudinal mixed-models which separate the effect of diet at baseline from the effect of change in diet and included time-varying covariates. In youth with type 1 diabetes, change in DASH-related diet score was inversely associated with HbA1c levels. Thus, a 10-point positive change (increase) in DASH score resulted in a 0.20% decrease in HbA1c levels. In youth with type 2 diabetes, change in DASH score was inversely associated with systolic BP. Here, a 10-point increase in DASH score resulted in a 2.02-mm Hg decrease in systolic BP. Additionally, a significant cross-sectional relationship was observed between DASH score at baseline and low-density lipoprotein/high-density lipoprotein ratio (β1=−0.14, P-value=0.0443) and DASH score at baseline and total cholesterol (β1=−7.78, P-value=0.0093).
Discussion
To the best of our knowledge, the effects of dietary changes characterized by a DASH diet score on CVD risk factors in youth with diabetes have not been evaluated in observational studies. In adults, greater adherence to a DASH diet has been associated with significantly reduced risk of heart failure, CVD and stroke in longitudinal studies.1, 2, 13, 14 However, these studies focused on the occurrence of an event rather than change in CVD risk factors over time. In adolescents, one study has shown that a DASH-style diet can help curb gains in body mass index15 and in two others, a DASH-style diet was associated with improved BP.9, 11 In general, a high-quality diet has been shown to positively affect energy intake, vascular flow and glucose control.16
This study found that a positive change in diet was associated with improvements in HbA1c levels among youth with type 1 diabetes and systolic BP in youth with type 2 diabetes. Strengths of this study include the longitudinal modeling to examine the change in DASH diet and the cross-sectional effect of baseline diet. Limitations include a small sample size; however, the modeling approach accounted for loss of follow-up by the inclusion of multiple time points. Conclusions were the same when restricting analyses to only those individuals with both baseline and follow-up 1 or follow-up 2 data. Lastly, this study did not provide information on specific changes in macro- or micronutrients.
Given the results and nutritional components of the DASH diet plan, sustaining good quality dietary intake as characterized by a DASH diet may serve as a benefit especially in youth with type 1 and type 2 diabetes.
References
Fung TT, Chiuve SE, McCullough ML, Rexrode KM, Logroscino G, Hu FB . Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch Intern Med 2001; 168: 713–720.
Levitan EB, Wolk A, Mittleman MA . Relation of consistency with the dietary approaches to stop hypertension diet and incidence of heart failure in men aged 45 to 79 years. Am J Cardiol 2009; 104: 1416–1420.
Hinderliter AL, Babyak MA, Sherwood A, Blumenthal JA . The DASH diet and insulin sensitivity. Curr Hypertens 2011. Rep 13: 67–73.
Bhupathiraju SN, Tucker KL . Coronary heart disease prevention: nutrients, foods, and dietary patterns. Clin Chim Acta 2011; 412: 1493–1514.
Rodriguez BL, Fujimoto WY, Mayer-Davis EJ, Imperatore G, Williams DE, Bell RA et al. Prevalence of cardiovascular disease risk factors in US. children and adolescents with diabetes: the SEARCH for diabetes in youth study. Diabetes Care 2006; 29: 1891–1896.
Liese AD, Bortsov A, Gunther AL, Dabelea D, Reynolds K, Standiford DA et al. Association of DASH diet with cardiovascular risk factors in youth with diabetes mellitus: the SEARCH for Diabetes in Youth study. Circulation 2011; 123: 1410–1417.
Gunther AL, Liese AD, Bell RA, Dabelea D, Lawrence JM, Rodriguez BL et al. Association between the dietary approaches to hypertension diet and hypertension in youth with Diabetes mellitus. Hypertension 2009; 53: 6–12.
U.S. Department of Health and Human Services. Your Guide to Lowering Your Blood Pressure: DASH Eating Plan, 2009. http://www.nhlbi.nih.gov/health/public/heart/hbp/dash/new_dash.pdf.
Moore LL, Bradlee ML, Singer MR, Qureshi MM, Buendia JR, Daniels SR . Dietary Approaches to Stop Hypertension (DASH) eating pattern and risk of elevated blood pressure in adolescent girls. Br J Nutr 2012; 108: 1678–1685.
Moore LL, Singer MR, Bradlee ML, Djoussé L, Proctor MH, Cupples LA et al. Intake of fruits, vegetables, and dairy products in early childhood and subsequent blood pressure change. Epidemiology 2005; 16: 4–11.
Couch SC, Saelens BE, Levin L, Dart K, Falciglia G, Daniels SR . The efficacy of a clinic-based behavioral nutrition intervention emphasizing a DASH-type diet for adolescents with elevated blood pressure. J Pediatr 2008; 152: 494–501.
SEARCH for Diabetes in Youth Study Group. SEARCH for Diabetes in Youth: a multicenter study of the prevalence, incidence and classification of diabetes mellitus in youth. Control Clin Trials 2004; 25: 458–471.
Levitan EB, Wolk A, Mittleman MA . Consistency with the DASH diet and incidence of heart failure. Arch Intern Med 2009; 169: 851–857.
Folsom AR, Parker ED, Harnack LJ . Degree of concordance with DASH diet guidelines and incidence of hypertension and fatal cardiovascular disease. Am J Hypertens 2007; 20: 225–232.
Berz JP, Singer MR, Guo X, Daniels SR, Moore LL . Use of a DASH food group score to predict excess weight gain in adolescent girls in the National Growth and Health Study. Arch Pediatr Adolesc Med 2011; 165: 540–546.
Mirmiran P, Noori N, Zavareh MB, Azizi F . Fruit and vegetable consumption and risk factors for cardiovascular disease. Metabolism 2009; 58: 460–468.
Acknowledgements
The SEARCH for Diabetes in Youth Study is indebted to the many youth and their families and their health care providers, whose participation made this study possible. SEARCH for Diabetes in Youth is funded by the Centers for Disease Control and Prevention (PA numbers 00097, DP-05-069, and DP-10-001) and supported by the National Institute of Diabetes and Digestive and Kidney Diseases. Site contract numbers: Kaiser Permanente Southern California (U48/CCU919219, U01 DP000246, and U18DP002714), University of Colorado Denver (U48/CCU819241-3, U01 DP000247, and U18DP000247-06A1), Kuakini Medical Center (U58CCU919256 and U01 DP000245), Children’s Hospital Medical Center (Cincinnati) (U48/CCU519239, U01 DP000248, and 1U18DP002709), University of North Carolina at Chapel Hill (U48/CCU419249, U01 DP000254, and U18DP002708-01), University of Washington School of Medicine (U58/CCU019235-4, U01 DP000244, and U18DP002710-01), Wake Forest University School of Medicine (U48/CCU919219, U01 DP000250 and 200-2010-35171). We wish to acknowledge the involvement of General Clinical Research Centers (GCRC) at the South Carolina Clinical & Translational Research (SCTR) Institute, at the Medical University of South Carolina (NIH/NCRR Grant number UL1RR029882); Children’s Hospital and Regional Medical Center (Grant Number M01RR00037); Colorado Pediatric General Clinical Research Center (Grant Number M01 RR00069) and the Barbara Davis Center at the University of Colorado at Denver (DERC NIH P30 DK57516); and the Institutional Clinical and Translational Science Award (CTSA), NIH/NCRR at the University of Cincinnati (Grant Number 1UL1RR026314-01).
DISCLAIMER
The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
AUTHOR CONTRIBUTIONS
TLB researched data and wrote manuscript. JLC assisted in data analyses and reviewed manuscript. RAB, EJM, DD and ADL contributed to discussion and reviewed/edited the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Barnes, T., Crandell, J., Bell, R. et al. Change in DASH diet score and cardiovascular risk factors in youth with type 1 and type 2 diabetes mellitus: The SEARCH for Diabetes in Youth Study. Nutr & Diabetes 3, e91 (2013). https://doi.org/10.1038/nutd.2013.32
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2013.32
Keywords
This article is cited by
-
Adherence to healthy diet and risk of cardiovascular disease in adult survivors of childhood cancer in the St. Jude Lifetime Cohort: a cross-sectional study
BMC Medicine (2023)
-
The Effects of Magnesium Supplementation on Blood Pressure and Obesity Measure Among Type 2 Diabetes Patient: a Systematic Review and Meta-analysis of Randomized Controlled Trials
Biological Trace Element Research (2021)
-
Diet quality indices and their associations with health-related outcomes in children and adolescents: an updated systematic review
Nutrition Journal (2020)
-
Modifiable Risk Factors for Cardiovascular Disease in Children with Type 1 Diabetes: Can Early Intervention Prevent Future Cardiovascular Events?
Current Diabetes Reports (2017)
-
Association of adherence to a Mediterranean diet with glycemic control and cardiovascular risk factors in youth with type I diabetes: the SEARCH Nutrition Ancillary Study
European Journal of Clinical Nutrition (2016)
