
Abstract
Objective:
The aim was to investigate adipose tissue vascular and metabolic effects of an adrenaline infusion in vivo in subjects with and without type 2 diabetes mellitus (T2DM).
Design:
Clinical intervention study with 1-h intravenous adrenaline infusion.
Subjects:
Eight male overweight T2DM subjects and eight male weight-matched, non-T2DM subjects were studied before, during and after an 1-h intravenous adrenaline infusion. Adipose tissue blood flow (ATBF) was determined by 133Xenon wash-out technique, and microvascular volume in the adipose tissue was studied by contrast-enhanced ultrasound imaging. Adipose tissue fluxes of glycerol, non-esterified fatty acids (NEFA), triacylglycerol and glucose were measured by Fick’s principle after catherisation of a radial artery and a vein draining the abdominal, subcutaneous adipose tissue.
Results:
ATBF increased similarly in both groups during the adrenaline infusion. One hour post adrenaline, ATBF was still increased in overweight T2DM subjects. Adrenaline increased microvascular volume in non-T2DM subjects while this response was impaired in overweight T2DM subjects. Adrenaline-induced increase in lipolysis was similar in both groups, but NEFA output from adipose tissue was delayed in overweight T2DM subjects. Glucose uptake in adipose tissue increased in non-T2DM subjects during adrenaline infusion but was unchanged in overweight T2DM subjects. This results in a delayed excess release of NEFA from the adipose tissue in overweight T2DM subjects after cessation of the adrenaline infusion.
Conclusion:
Capillaries in the adipose tissue are recruited by adrenaline in non-T2DM subjects; however, this response is impaired in overweight T2DM subjects. NEFA, released in adipose tissue during adrenaline stimulation, is insufficiently re-esterified in situ in overweight T2DM subjects, probably owing to increased ATBF after adrenaline infusion and inability to increase adipose tissue glucose uptake.
Similar content being viewed by others

Introduction
Adipose tissue blood flow (ATBF) has a fundamental role in the regulation of the adipose tissue metabolism. In healthy subjects, the ATBF increases when lipid is mobilised from the tissue, for example, during prolonged exercise,1, 2 as well as in conditions in which lipid is deposited in the tissue, for example, postprandially.3, 4, 5 In both situations, sympatho-adrenergic activity is one of the mechanisms that helps eliciting the vasodilation.6, 7 During lipid mobilisation, the vasodilation facilitates the fatty acid release from the tissue by increasing the supply of albumin to the tissue and thereby enabling the water-insoluble fatty acids to be removed by the blood. During lipid deposition, the vasodilation helps increasing the supply of triacylglycerol (TAG)-rich lipoproteins for hydrolysis and enhanced lipid deposition in the tissue.8, 9 However, the dynamics of ATBF changes are reduced in obesity and, especially, in type 2 diabetes mellitus (T2DM) subjects,10, 11 and it has been shown that the postprandial changes in ATBF are closely correlated to insulin sensitivity.12, 13
We have recently shown that in the abdominal, subcutaneous adipose tissue of healthy, normal-weight subjects, capillaries are recruited and microvascular volume is increased in response to an oral glucose load.14 The capillary recruitment exposes more of the capillary-bound lipoprotein lipase to substrate. It follows that capillary recruitment may have a key role in the regulation of the postprandial lipid metabolism. In another recent study, we showed that the glucose-induced capillary recruitment is impaired in T2DM subjects.15 Whether capillary recruitment also takes place in adipose tissue during lipid mobilisation is unknown. Therefore, the aim of the study was to investigate the adipose tissue vascular and metabolic effects of an infusion of adrenaline in physiological amounts in overweight subjects with T2DM and in weight-matched non-T2DM control subjects.
Subjects and methods
Subjects
Two groups were included in the study. One group consisted of eight overweight male T2DM subjects that were all treated with diet and oral antidiabetic medication. The known duration of diabetes was 6.5 years (range 2–20 years). Eight healthy male subjects were matched with the overweight T2DM subjects according to age, height, weight and body composition (Table 1). None of the subjects exercised on a regular basis. The study was performed according to the ‘Declaration of Helsinki II’ and was approved by the Scientific Ethical Committees of the Capital Region, Denmark (project no. H-B-2009-044). All subjects gave informed consent to participate in the study.
Experimental protocol
Approximately 2 weeks before the experimental day, the subjects were scanned by dual-energy X-ray absorptiometry to determine lean body mass and fat mass (Lunar DPX-IQ, software version 4.6c; Madison, WI, USA) (Table 1). Forty-eight hours before the experiment, subjects avoided strenuous physical activity. After an overnight fast of about 12 h, during which subjects were only allowed to drink water, the subjects attended the laboratory at 0800 hours. In the overweight T2DM subjects, the antidiabetic medication was discontinued 24 h before beginning the experiment.
The subjects were placed in the supine position in a bed and catheterised in a superficial medial cubital vein (18G BD Venflon, PRO, Becton Dickinson, Singapore). Another catheter (Artflon (BD, Becton Dickinson, Singapore)) was inserted percutaneously into the radial artery of the non-dominant arm during local anaesthesia (1 ml 1% lidocaine). The catheter was kept patent with regular flushing with isotonic sodium chloride. A subcutaneous, abdominal vein was catheterised during ultrasound/colour-Doppler imaging of the vein as previously described.16 A 22G 10 cm polyurethane catheter (Arrow International, Reading, PA, USA) was inserted using the Seldinger technique. After insertion, the catheter was kept patent throughout the study by continuous infusion of isotonic sodium chloride at a rate of 40 ml h−1. Contra-laterally to the catheter position, ATBF was determined in the periumbilical, subcutaneous adipose tissue by washout of 133Xenon.14, 17 The washout rate of 133Xenon was measured continuously by a scintillation counter system strapped to the skin surface above the 133Xenon depot (Oakfield Instruments, Oxford, UK). The ATBF was calculated from the mean washout rate determined in 10-min periods coinciding with the time of ultrasound recordings. The tissue-to-blood partition coefficient λ used was 10 g ml−1.18
An ultrasound scanning setup was made as explained in detail earlier.14 In short, this setup included a L9–3MHz linear array ultrasound transducer placed horizontally at the right side of the abdomen ∼5 cm above the iliac crest in the mid-axial line. The ultrasound transducer was fixed to prevent displacement as well as any pressure of the transducer on the underlying tissue, and it was made sure that the subject did not change body position during the measurements.
An iU22 ultrasound scanner (Phillips Medical Systems, Bothell, WA, USA) was set to operate in contrast harmonic mode and at a mechanical index of 0.06, with the depth set at 3 cm, and focus and gain optimised at the beginning of the experiment and held constant throughout.
Ultrasound gel was applied liberally and an initial baseline measurement was obtained using a bolus of 1.5 ml of ultrasound contrast agent (SonoVue, Bracco S.p.A, Milan, Italy) that was injected intravenously followed by an immediate flush of 10 ml isotonic sodium chloride.14
B-mode imaging was created from broadband spectra of acoustic frequencies from 3–9 MHz. First harmonic contrast signals were received at 8 MHz. Twenty-millisecond images were captured consecutively for 2 min after bolus injections.
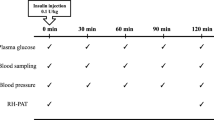
The experiment consisted of a baseline (pre-adrenaline) period of ∼60 min, where equilibrium of the injected 133Xenon was achieved followed by a 60-min continuous intravenous adrenaline infusion (0.15 nmol kg−1 lean body weight min−1) and 60 min after cessation of the adrenaline infusion (post adrenaline). Room temperature was kept at 24 °C.
The contrast-enhanced ultrasound recordings in adipose tissue were preceded by abdominal vein and radial artery blood sampling and done immediately before the adrenaline infusion at 0 min and again at 30, 60 and 120 min.
Image analysis
Image analysis was performed offline using ultrasound quantification and analysis software (QLAB version 8, Phillips Medical Systems). The analysis consisted of examination of a region of interest for each recording in the abdominal, subcutaneous adipose tissue. In a region of interest, the relative microvascular volume in the tissue was determined as the mean signal intensity in decibels during the first plateau phase after subtraction of the mean signal intensity registered immediately before the contrast bolus injection.14
Blood analysis
Plasma non-esterified fatty acids (NEFA) concentrations were measured in arterial and venous blood in duplicates in heparinised plasma with enzymatic methods using a Wako NEFA-C test kit (TriChem Aps-interkemi, Copenhagen, Denmark), in a Beckman Coulter (Brea, CA, USA) Synchron Cx Systems. TAG and glycerol were measured in arterial and venous plasma in duplicates using TG-B, Triglycerides GPO Blanked Kit TG-B (Ramcon A/S, Birkeroed, Denmark) and determined on an automated analyser (Hitachi 612 Automatic Analyser; Roche, Basel, Switzerland). Arterial plasma adrenaline was measured in duplicates with an Adrenaline Research Elisa kit (Labor Diagnostic Nord, Nordhorn, Germany), and determined on an Elisa reader Multiskan GO (Multiscan, Labsystem, Vienna, VA, USA). Samples for analysis of glucose and haematocrit in arterial and venous blood were taken anaerobically in gas-tight heparinised syringes and analysed immediately in duplicates using an ABL 725 (Radiometer, Copenhagen, Denmark).
Calculations
Net metabolite fluxes over the abdominal, subcutaneous adipose tissue were calculated by multiplying the venous-arterial (output) or the arterio-venous (uptake) difference in metabolite concentrations by the appropriate blood or plasma flow (whole blood for the calculations of glucose and glycerol and plasma flow for the calculations of NEFA fluxes). The NEFA/glycerol release ratio was calculated from the net NEFA and net glycerol outputs.
Statistical analyses
These were performed with GraphPad Prism version 4 (GraphPad Software, Inc., CA, USA). Results are presented as mean±s.e.m. Differences were assessed by a paired t-test and one-way analysis of variance test with Tukey post-hoc test. P<0.05 was considered statistically significant in two-tailed testing.
Results
Vascular responses
Abdominal, subcutaneous ATBF
The ATBF in the pre-adrenaline period was similar in the healthy subjects and the overweight T2DM subjects (Table 2). During the adrenaline infusion, ATBF increased significantly in both groups and peaked at 60 min (P<0.05). Sixty minutes post adrenaline, the ATBF was still significantly increased in the overweight T2DM subjects compared with the pre-adrenaline value. In addition, it was significantly higher than the ATBF in the overweight, non-T2DM subjects (P<0.05). In these subjects, ATBF had returned to the pre-adrenaline level 60 min post adrenaline.
Abdominal, subcutaneous adipose tissue microvascular volume
In the overweight, non-T2DM subjects adrenaline induced an increase in the microvascular volume, and this remained increased throughout the infusion (P<0.05). In contrast to this, the microvascular volume did not change significantly in the overweight T2DM subjects during the whole experiment (P=0.36 at 30 min during adrenaline infusion).
Arterial concentrations
Glycerol and NEFA concentrations were not significantly different in the pre-adrenaline period in the two groups (Table 3). They increased similarly and peaked after 30 min in both groups during the adrenaline infusion (P<0.05). Post adrenaline the arterial glycerol and NEFA concentrations decreased to values below pre-adrenaline (P<0.05).
The arterial TAG concentrations were equal in the two groups and remained constant throughout the experiment.
During the whole experiment, the arterial glucose concentration was significantly higher in the overweight T2DM subjects compared with the overweight, non-T2DM subjects. During the adrenaline infusion, blood glucose concentrations increased significantly in both groups.
Similar arterial adrenaline concentrations were found in the two groups. The concentrations increased ∼10-fold from pre-adrenaline concentrations during the infusion.
Adipose tissue concentration differences and fluxes of metabolites
The net glycerol and net NEFA output increased significantly in both groups during the adrenaline infusion (Table 4). However, while the glycerol outputs increased in parallel, there was a delayed rise in NEFA output in the overweight T2DM subjects compared with the overweight, non-T2DM subjects. After the cessation of the infusion, the glycerol and NEFA output decreased to values below pre-adrenaline in the overweight, non-T2DM subjects but not in the overweight T2DM subjects. In these latter subjects, the NEFA output remained significantly higher than the pre-adrenaline value and was also higher than the concomitant value in the overweight, non-T2DM subjects.
The pre-adrenaline NEFA/glycerol release ratios were similar in the two groups. During the adrenaline infusion, this ratio decreased initially in both groups, however, more pronounced in overweight T2DM subjects. Post adrenaline it increased to more than 3 in both groups but was 25% higher in the overweight T2DM subjects than in the overweight, non-T2DM subjects. However, these changes did not reach statistical significance, probably owing to the low number of subjects.
It was not possible to demonstrate a significant TAG uptake during the experiments in any of the subject groups (data not shown).
Pre-adrenaline there was a significant glucose uptake in the subcutaneous, abdominal adipose tissue in both groups. During the adrenaline infusion, the glucose uptake increased significantly in the overweight, non-T2DM subjects but not in the overweight T2DM subjects.
Discussion
The main findings of this study are:
-
1
During a physiological adrenaline stimulus, the abdominal, subcutaneous adipose tissue microvascular volume increases in overweight, non-T2DM subjects, but this response is impaired in overweight subjects with T2DM.
-
2
The lipolytic rate in the abdominal, subcutaneous adipose tissue is similar in overweight, non-T2DM subjects and in overweight T2DM subjects, during a physiological adrenaline infusion. However, in overweight subjects with T2DM the rise in ATBF as well as in NEFA release is delayed and, in contrast to findings in overweight, non-T2DM subjects are maintained for 60 min after cessation of the adrenaline stimulation.
-
3
Adrenaline stimulation results in an increase in adipose tissue glucose uptake in overweight, non-T2DM subjects but not in overweight subjects with T2DM.
The strength of our study is that the applied experimental techniques allow direct detailed measurements of vascular and metabolic effects in vivo. A weakness of the study is the low number of experimental subjects.
In a recent study, we have demonstrated that capillary recruitment takes place in the adipose tissue simultaneously with an increase in ATBF during an oral glucose load in healthy, normal-weight subjects.14 The increase in ATBF and the microvascular volume in the abdominal, subcutaneous adipose tissue is impaired in overweight subjects with T2DM under similar experimental conditions when compared with healthy overweight, non-T2DM subjects.15 We have previously found that the glucose-induced vasodilatation in adipose tissue is mainly elicited via beta-adrenergic mechanisms.7 In line with these findings, we now show that adrenaline increases both ATBF and capillary recruitment in the abdominal, subcutaneous adipose tissue in overweight, non-T2DM subjects. Furthermore, in overweight T2DM subjects the rise in ATBF is delayed and the increase in adipose tissue microvascular volume is impaired.
The adrenaline infusion rate we applied in this experiment resulted in blood concentrations equivalent to those seen during strenuous exercise,19 and to the same level as we have applied previously in healthy lean subjects.20 In the healthy lean subjects, we found a twofold increase in ATBF during adrenaline infusion, and after cessation of the infusion the ATBF returned to pre-adrenaline level. However, in the present experiment the post-adrenaline ATBF did not decrease to the same extent in the overweight T2DM subjects as in the overweight, non-T2DM subjects. Furthermore, in contrast to the events in overweight, non-T2DM subjects, the ATBF increase in the overweight T2DM subjects took place without a concomitant increase in capillary recruitment. This indicates that during a physiological adrenaline stimulus, in overweight T2DM subjects, the increase in ATBF is accompanied by a faster blood flow rate, that is, shorter transit time through the adipose tissue vascular bed. The mechanisms responsible for the changes in the abdominal, subcutaneous adipose tissue microvascular volume have not yet been identified. However, Georgescu et al.21 have found that in subjects with T2DM and to lesser extent in obese subjects, the arterioles in abdominal, subcutaneous adipose tissue are dysfunctional with increased contractility and reduced endothelium-dependent vasorelaxation. Furthermore, a recent study comparing lean healthy and insulin-resistant subjects found that in the abdominal, subcutaneous adipose tissue there is fewer capillaries and more large microvessels in the insulin-resistant subjects.22 The described functional and structural remodelling of the adipose tissue microcirculation may explain our finding of impaired ability to increase the microvascular volume in the overweight T2DM subjects. We did not measure insulin in the present experiments as we and others previously have shown that insulin per se does not influence adipose tissue total blood flow.23, 24, 25 However, we cannot exclude that insulin may have a role in the adipose tissue capillary recruitment. If so, this could explain the difference in capillary recruitment between the present experimental groups. In order to test this hypothesis additional experiments have to be performed.
In a previous study of subjects with overweight T2DM, we have found that these subjects have a blunted increase in ATBF during prolonged exercise of moderate intensity. In addition, the ability to increase the NEFA mobilisation was significantly reduced while the glycerol release increased to the same extent as found in healthy, lean subjects.11, 2 Usually, net glycerol release from adipose tissue is taken to be equal to the lipolytic rate in the tissue, although a small re-uptake of glycerol has been demonstrated.26, 27 Therefore, a NEFA/glycerol release ratio <3 normally is interpreted as NEFA re-esterification intracellulary.28 However, we have previously shown that post exercise, NEFA is released in excess from adipose tissue compared with the lipolytic rate as evidenced by a NEFA/glycerol release ratio higher than 3.11, 2 This indicates that either some of the NEFA released by lipolysis during exercise may be transiently trapped intracellularly without being re-esterified or that incomplete triglyceride hydrolysis takes place after exercise. A similar pattern was found in the present experiment during adrenaline infusion in both groups, although, to a larger extent in the overweight T2DM subjects.
Adrenaline caused a significant increase in the adipose tissue glucose uptake in the overweight, non-T2DM subjects, while the glucose uptake did not change in the overweight T2DM subjects during the infusion. Adipose tissue glucose uptake has been shown to be stimulated via α1-adrenergic receptors both in man29, 30 and in rat.31 The present experiment indicates that α1-adrenergic receptors have a role in the regulation of adipose tissue glucose uptake in the intact organism. In skeletal muscle, it has been demonstrated that the ability to increase glucose uptake is partly dependent on the ability to recruit capillaries.32 In muscle, an adrenaline-induced increase in metabolic rate33 as well as direct enhancement by adrenaline of glucose transport34 may also contribute in explaining adrenaline-induced augmentation of glucose uptake. Our results suggest that also adipose tissue capillary recruitment contribute to increase glucose uptake. The fact that adrenaline-stimulated glucose uptake was lower in the overweight T2DM than in the overweight, non-T2DM subjects may partly reflect the absence of capillary recruitment in the former. Another explanation may be that in overweight subjects with T2DM, the glucose uptake in adipose tissue is decreased owing to decreased insulin sensitivity and/or the α1-adrenergic receptor sensitivity is downregulated. The inability to increase adipose tissue glucose uptake may result in an insufficient supply of the necessary substrate for NEFA re-esterification in situ as suggested in Boschmann et al.29 and Cahova et al.31 This is supported by the more pronounced increase in the NEFA/glycerol release ratio post adrenaline in the overweight T2DM subjects compared with the overweight, non-T2DM subjects, which indicates that the NEFA re-esterification in the adipose tissue in situ during the adrenaline infusion is lower in the former compared with the latter subjects. The higher ATBF in overweight T2DM compared with overweight, non-T2DM subjects after cessation of adrenaline infusion probably also contributed to a difference in re-esterification between groups, because removal of NEFA from the tissue is directly dependent on flow.8 As the arterial NEFA concentrations post adrenaline at the same time decreased to values significantly lower than the pre-adrenaline concentrations, this implies that fatty acids are diverted from adipose tissue to be taken up in other tissues, for example, liver and skeletal muscles in this period.
After cessation of the adrenaline infusion, the lipolytic rate was suppressed in adipose tissue to values below pre-adrenaline in the non-T2DM subjects but not in the overweight T2DM subjects. The suppressed post-adrenaline lipolysis is in accordance with our previous findings in healthy subjects.20 It can be speculated if the missing suppression in the overweight T2DM subjects is due to decreased sensitivity to the insulin antilipolytic effect in these subjects. Alternatively, in healthy subjects the decrease in lipolysis during and after adrenaline is due to a desensitisation of the beta-adrenoceptors,35 but not the α2-receptors giving rise to a delayed antilipolytic effect of adrenaline.36 This phenomenon may be blunted in overweight T2DM subjects. However, it will demand additional experiments to elucidate these hypotheses.
Conclusion
In the abdominal, subcutaneous adipose tissue, capillaries are recruited in response to an adrenaline stimulus in overweight, non-T2DM subjects; however, this response is impaired in overweight T2DM subjects. NEFA, released in adipose tissue during adrenaline stimulation, is after cessation of the stimulation insufficiently re-esterified in situ in overweight T2DM subjects, probably owing to prolonged increase in ATBF and to impaired increase in adipose tissue glucose uptake.
References
Bulow J . Adipose tissue blood flow during exercise. Dan Med Bull 1983; 30: 85–100.
Mulla NA, Simonsen L, Bulow J . Post-exercise adipose tissue and skeletal muscle lipid metabolism in humans: the effects of exercise intensity. J Physiol 2000; 524 (Pt 3): 919–928.
Enevoldsen LH, Simonsen L, Macdonald IA, Bulow J . The combined effects of exercise and food intake on adipose tissue and splanchnic metabolism. J Physiol 2004; 561: 871–882.
Fielding BA, Frayn KN . Lipoprotein lipase and the disposition of dietary fatty acids. Br J Nutr 1998; 80: 495–502.
Frayn KN . Adipose tissue as a buffer for daily lipid flux. Diabetologia 2002; 45: 1201–1210.
Ardilouze JL, Fielding BA, Currie JM, Frayn KN, Karpe F . Nitric oxide and beta-adrenergic stimulation are major regulators of preprandial and postprandial subcutaneous adipose tissue blood flow in humans. Circulation 2004; 109: 47–52.
Simonsen L, Bulow J, Astrup A, Madsen J, Christensen NJ . Diet-induced changes in subcutaneous adipose tissue blood flow in man: effect of beta-adrenoceptor inhibition. Acta Physiol Scand 1990; 139: 341–346.
Bulow J, Madsen J . Influence of blood flow on fatty acid mobilization form lipolytically active adipose tissue. Pflugers Arch 1981; 390: 169–174.
Samra JS, Simpson EJ, Clark ML, Forster CD, Humphreys SM, Macdonald IA et al. Effects of epinephrine infusion on adipose tissue: interactions between blood flow and lipid metabolism. Am J Physiol 1996; 271: E834–E839.
Summers LK, Samra JS, Humphreys SM, Morris RJ, Frayn KN . Subcutaneous abdominal adipose tissue blood flow: variation within and between subjects and relationship to obesity. Clin Sci (Lond) 1996; 91: 679–683.
Simonsen L, Henriksen O, Enevoldsen LH, Bulow J . The effect of exercise on regional adipose tissue and splanchnic lipid metabolism in overweight type 2 diabetic subjects. Diabetologia 2004; 47: 652–659.
Jansson PA, Larsson A, Lonnroth PN . Relationship between blood pressure, metabolic variables and blood flow in obese subjects with or without non-insulin-dependent diabetes mellitus. Eur J Clin Invest 1998; 28: 813–818.
Karpe F, Fielding BA, Ilic V, Macdonald IA, Summers LK, Frayn KN . Impaired postprandial adipose tissue blood flow response is related to aspects of insulin sensitivity. Diabetes 2002; 51: 2467–2473.
Tobin L, Simonsen L, Bulow J . Real-time contrast-enhanced ultrasound determination of microvascular blood volume in abdominal subcutaneous adipose tissue in man. Evidence for adipose tissue capillary recruitment. Clin Physiol Funct Imaging 2010; 30: 447–452.
Tobin L, Simonsen L, Bulow J . The dynamics of the microcirculation in the subcutaneous adipose tissue is impaired in the postprandial state in type 2 diabetes. Clin Physiol Funct Imaging 2011; 31: 458–463.
Simonsen L, Bulow J, Madsen J . Adipose tissue metabolism in humans determined by vein catheterization and microdialysis techniques. Am J Physiol 1994; 266: E357–E365.
Simonsen L, Enevoldsen LH, Bulow J . Determination of adipose tissue blood flow with local 133Xe clearance. Evaluation of a new labelling technique. Clin Physiol Funct Imaging 2003; 23: 320–323.
Bulow J, Jelnes R, Astrup A, Madsen J, Vilmann P . Tissue/blood partition coefficients for xenon in various adipose tissue depots in man. Scand J Clin Lab Invest 1987; 47: 1–3.
Galbo H, Holst JJ, Christensen NJ . Glucagon and plasma catecholamine responses to graded and prolonged exercise in man. J Appl Physiol 1975; 38: 70–76.
Stallknecht B, Simonsen L, Bulow J, Vinten J, Galbo H . Effect of training on epinephrine-stimulated lipolysis determined by microdialysis in human adipose tissue. Am J Physiol 1995; 269: E1059–E1066.
Georgescu A, Popov D, Constantin A, Nemecz M, Alexandru N, Cochior D et al. Dysfunction of human subcutaneous fat arterioles in obesity alone or obesity associated with Type 2 diabetes. Clin Sci (Lond) 2011; 120: 463–472.
Spencer M, Unal R, Zhu B, Rasouli N, McGehee RE, Peterson CA et al. Adipose tissue extracellular matrix and vascular abnormalities in obesity and insulin resistance. J Clin Endocrinol Metab 2011; 96: E1990–E1998.
Stallknecht B, Larsen JJ, Mikines KJ, Simonsen L, Bulow J, Galbo H . Effect of training on insulin sensitivity of glucose uptake and lipolysis in human adipose tissue. Am J Physiol Endocrinol Metab 2000; 279: E376–E385.
Karpe F, Fielding BA, Ardilouze JL, Ilic V, Macdonald IA, Frayn KN . Effects of insulin on adipose tissue blood flow in man. J Physiol 2002; 540: 1087–1093.
Asmar M, Simonsen L, Madsbad S, Stallknecht B, Holst JJ, Bulow J . GIP may enhance fatty acid re-esterification in subcutaneous, abdominal adipose tissue in lean humans. Diabetes 2010; 59: 2160–2163.
van Hall G, Bulow J, Sacchetti M, Al MN, Lyngso D, Simonsen L . Regional fat metabolism in human splanchnic and adipose tissues; the effect of exercise. J Physiol 2002; 543: 1033–1046.
Jocken JW, Goossens GH, van Hees AM, Frayn KN, van Baak M, Stegen J et al. Effect of beta-adrenergic stimulation on whole-body and abdominal subcutaneous adipose tissue lipolysis in lean and obese men. Diabetologia 2008; 51: 320–327.
Frayn KN, Humphreys SM . Metabolic characteristics of human subcutaneous abdominal adipose tissue after overnight fast. Am J Physiol Endocrinol Metab 2012; 302: E468–E475.
Boschmann M, Krupp G, Luft FC, Klaus S, Jordan J . In vivo response to alpha(1)-adrenoreceptor stimulation in human white adipose tissue. Obes Res 2002; 10: 555–558.
Flechtner-Mors M, Jenkinson CP, Alt A, Biesalski HK, Adler G, Ditschuneit HH . Sympathetic regulation of glucose uptake by the alpha1-adrenoceptor in human obesity. Obes Res 2004; 12: 612–620.
Cahova M, Palenickova E, Papackova Z, Dankova H, Skop V, Kazdova L . Epinephrine-dependent control of glucose metabolism in white adipose tissue: the role of alpha- and beta-adrenergic signalling. Exp Biol Med (Maywood ) 2012; 237: 211–218.
Vincent MA, Clerk LH, Lindner JR, Klibanov AL, Clark MG, Rattigan S et al. Microvascular recruitment is an early insulin effect that regulates skeletal muscle glucose uptake in vivo. Diabetes 2004; 53: 1418–1423.
Richter EA, Christensen NJ, Ploug T, Galbo H . Endurance training augments the stimulatory effect of epinephrine on oxygen consumption in perfused skeletal muscle. Acta Physiol Scand 1984; 120: 613–615.
Richter EA, Ruderman NB, Galbo H . Alpha and beta adrenergic effects on metabolism in contracting, perfused muscle. Acta Physiol Scand 1982; 116: 215–222.
Stallknecht B, Bulow J, Frandsen E, Galbo H . Desensitization of human adipose tissue to adrenaline stimulation studied by microdialysis. J Physiol 1997; 500: 271–282.
Lafontan M, Bousquet-Melou A, Galitzky J, Barbe P, Carpéné C, Langin D et al. Adrenergic receptors and fat cells: differential recruitment by physiological amines and homologous regulation. Obes Res 1995; 3 (Suppl 4): 507S–514S.
Acknowledgements
This study is supported by a grant from The Novo Nordisk Foundation. Technical assistance was kindly provided by Lisbeth Kall.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Tobin, L., Simonsen, L., Galbo, H. et al. Vascular and metabolic effects of adrenaline in adipose tissue in type 2 diabetes. Nutr & Diabetes 2, e46 (2012). https://doi.org/10.1038/nutd.2012.19
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2012.19
Keywords
This article is cited by
-
Lymphatic drainage affects lipolytic activity of femoral adipose tissue in women
International Journal of Obesity (2020)
-
Increased levels of FFA during passive heat loading after a 2-week repeated heat load in Koreans
International Journal of Biometeorology (2015)
