
Abstract
The purpose of this study was to determine the association between visceral adipose tissue (VAT) and all-cause mortality. The sample included 1089 white men and women 18–84 years of age from the Pennington Center Longitudinal Study, a prospective cohort of participants assessed between 1995 and 2008, and followed for mortality until 31 December 2009. Abdominal VAT was measured at the L4–L5 vertebral level using computed tomography. There were 27 deaths during an average of 9.1 years of follow-up. Abdominal VAT was significantly associated with mortality after adjustment for age, sex and year of examination (hazards ratio (HR) 1.46; 95% confidence interval 1.05–2.05). The association was stronger after the inclusion of abdominal subcutaneous adipose tissue (SAT), smoking status, alcohol consumption and leisure-time physical activity as additional covariates (HR 1.74; 1.17–2.59). Limiting the sample to participants who were free of stroke, heart disease and cancer at baseline reduced the strength of the relationship slightly (HR 1.62; 1.07–2.47). Abdominal SAT was not associated with mortality, either alone or in combination with VAT and other covariates. The results support the assertion that abdominal VAT is an important therapeutic target for obesity reduction efforts.
Similar content being viewed by others

Introduction
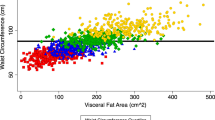
Abdominal visceral adipose tissue (VAT) is considered to be one of the most dangerous fat depots in the body, as it is strongly related to cardiometabolic risk factors and insulin resistance.1 Waist circumference is often considered to be the best anthropometric proxy for VAT;2, 3 however, correlations between the two are typically on the order of 0.6–0.8.4, 5 Thus, waist circumference is at best an imprecise estimate of VAT, and it is more highly correlated with total adiposity.5
There is consistent evidence for a relationship between waist circumference and diabetes, cardiovascular disease and all-cause mortality.6 However, to our knowledge, only two studies have examined the association between directly measured VAT and mortality in humans.7, 8 The first study, using a nested case–control design in men, demonstrated that VAT is a strong, independent predictor of all-cause mortality, after adjustment for age, subcutaneous adipose tissue (SAT) and liver fat.7 The second study, using a prospective design, showed that VAT was a significant predictor of all-cause mortality in Japanese Americans, independent of age, smoking and SAT.8 Thus, given the paucity of data on the association between directly measured VAT and mortality rates, the purpose of this study was to determine the association of abdominal VAT with all-cause mortality in white adults using a prospective cohort design.
Subjects and methods
Sample
The Pennington Center Longitudinal Study (PCLS) is an on-going investigation of the effects of obesity and lifestyle factors on the development of chronic diseases and premature mortality.9 The sample is composed of volunteers who have participated in a variety of clinical studies conducted at the Pennington Biomedical Research Center in Baton Rouge, Louisiana between 1995 and 2008. The current analysis included 1089 white men (n=492) and women (n=597) 18–84 years of age who had undergone a computed tomography (CT) scan of the abdomen. Not having a CT scan available was the primary exclusionary criterion for this study. Although PCLS also includes African Americans, the sample size was not sufficient for analysis. Each participant provided their written informed consent, and all PCLS procedures were approved by the Pennington Biomedical Research Center Institutional Review Board.
Baseline examination
Height and weight were measured using a wall-mounted stadiometer and a digital scale, respectively, after the volunteer removed outer clothing, heavy pocket items and shoes. The body mass index was calculated as weight in kg/height in m2. Abdominal VAT and SAT areas (cm2) were measured using CT, as previously described.9, 10 For the measurement, participants lay in a supine position with arms overhead to obtain a cross-sectional image at the L4–L5 intervertebral space. Three different CT scanners were used for the PCLS: GE High Speed Advantage (1996–2000), GE Light-Speed Plus (2000–2007) and GE LightSpeed VCT (2007–2011; General Electric Company, Fairfield, CT, USA). The CT scanners were calibrated daily to air, and the CT images were analyzed with commercially available software (Analyze; Analyze Direct, Rochester, MN, USA). The intra-rater reliability of VAT measurement by the technician is quite good (0.25%).
Covariates
Information on several covariates was collected at baseline for inclusion in the statistical models. Participant age was computed from birth and observation dates, and year of examination was included as a covariate to account for potential temporal trends in baseline measurements. Smoking status, alcohol consumption and engagement in leisure-time physical activity (from a list of six to nine common physical activities provided) were self-reported during the baseline data collection.
Ascertainment of mortality status
The vital status of all participants and causes of death were determined by linkage to the National Death Index.11 The primary endpoint for this analysis was death from all causes. All deaths occurring between 6 months after the baseline assessment and 31 December 2009 were included in the analysis. The average length of follow-up was 9.1 years (s.d. 3.3 years; maximum 14.0 years). The first death occurred 2.2 years after baseline.
Statistical analysis
Cox proportional hazards regression was used to assess the association between VAT, SAT and all-cause mortality rates, adjusting for a variety of covariates as described below. We present the results of five models: Model 1 includes VAT as the primary exposure, adjusted for age, sex and exam year; Model 2 includes SAT as the primary exposure adjusted for age, sex and exam year; Model 3 includes both VAT and SAT as exposures, adjusted for age, sex and exam year; Model 4 includes both VAT and SAT as exposures, adjusted for age, sex, exam year, smoking status (never, former, current and unknown), alcohol consumption (no, yes and unknown) and leisure-time physical activity (<4 h per week, ⩾4 h per week, unknown); Model 5 includes both VAT and SAT, and is limited to participants without a history of stroke, heart disease or cancer at baseline (n=1044, n=26 decedents), adjusted for the same covariates as Model 4. All hazards ratios (HRs) are expressed per s.d. of the exposure variable (70.1 cm2 for VAT and 151 cm2 for SAT) to facilitate comparisons. All analyses were conducted with SAS, version 9.2 (SAS Institute, Inc., Cary, NC, USA).
Results
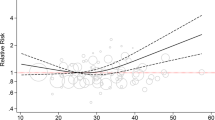
The mean age of the sample at baseline was 46.0 years (s.d. 12.5 years). The decedents were significantly older and had higher VAT than survivors (Table 1). A total of 27 deaths (5 cardiovascular disease, 9 cancer and 13 other) occurred over 9860 person-years of follow-up. The results of the five proportional hazards regression models are presented in Table 2. Abdominal VAT was a significant predictor of mortality both alone and in combination with SAT (HR=1.72; 1.20–2.47). The inclusion of additional covariates did not attenuate the relationship between VAT and mortality; however, limiting the sample to participants who were free of stroke, heart disease and cancer at baseline reduced the strength of the relationship slightly (HR=1.62; 1.07–2.47). Abdominal SAT was not a significant predictor of mortality in any of the models, either alone or in combination with VAT and other covariates.
Discussion
The results of this study demonstrate an independent effect of VAT on all-cause mortality rates in a sample of white men and women. The magnitude of the association after adjustment for SAT (HR=1.72; 1.20–2.47) is similar to that obtained by Kuk et al.7 (RR=1.93; 1.15–3.23) in men, and McNeely et al.8 (HR=1.47 (1.14–1.89) in Japanese Americans. All three studies have demonstrated that the association between VAT and mortality is independent of several covariates. Among Japanese Americans, the association between VAT and mortality was reduced somewhat after adjustment for body mass index (RR=1.34 (0.99–1.82); however, in this study, the inclusion of body mass index as an additional covariate in Model 2 did not reduce the strength of the association (HR=1.66; 1.07–2.57). These human studies are supported by research that shows that the surgical removal of VAT in rats results in higher mean and maximum lifespan, compared with ad libitum fed rats.12
These results support the use of VAT as a primary target for obesity-reduction strategies. Lifestyle-based interventions such as diet and physical activity have been shown to significantly reduce VAT even in the absence of weight loss.13 VAT is currently not routinely measured in clinical practice, in part due to the requirement of magnetic resonance imaging or CT. However, recent technological advances may allow for the quantification of VAT using other modalities such as dual-energy X-ray absorptiometry.14
The strengths of this study include the precise measurement of VAT and SAT using CT, the prospective research design and the ascertainment of mortality through the National Death Index. However, the small sample size and non-representativeness of the sample limit the generalizability of the results. Although we were able to control for self-reported physical activity and alcohol intake, we did not have a measure of overall dietary intake. Future studies should seek to replicate these results using larger, more representative samples of the population.
In conclusion, this study has demonstrated a significant positive association between VAT and all-cause mortality in this sample of white adults. The assessment of VAT should be a priority for the clinical assessment of obesity and related comorbidities.
References
Després J-P, Lemieux I . Abdominal obesity and metabolic syndrome. Nature 2006; 444: 881–887.
Pouliot MC, Despres JP, Lemieux S, Moorjani S, Bouchard C, Tremblay A et al. Waist circumference and abdominal sagittal diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol 1994; 73: 460–468.
Rankinen T, Kim SY, Perusse L, Despres JP, Bouchard C . The prediction of abdominal visceral fat level from body composition and anthropometry: ROC analysis. Int J Obes Relat Metab Disord 1999; 23: 801–809.
Barreira TV, Staiano AE, Harrington DM, Heymsfield SB, Smith SR, Bouchard C et al. Anthropometric correlates of total body fat, abdominal adiposity, and cardiovascular disease risk factors in a biracial sample of men and women. Mayo Clin Proc 2012; 87: 452–460.
Bouchard C . BMI, fat mass, abdominal adiposity and visceral fat: where is the 'beef'? Int J Obes Relat Metab Disord 2007; 31: 1552–1553.
Ross R, Berentzen T, Bradshaw AJ, Janssen I, Kahn HS, Katzmarzyk PT et al. Does the relationship between waist circumference, morbidity and mortality depend on measurement protocol for waist circumference? Obes Rev 2008; 9: 312–325.
Kuk JL, Katzmarzyk PT, Nichaman MZ, Church TS, Blair SN, Ross R . Visceral fat is an independent predictor of all-cause mortality in men. Obesity 2006; 14: 336–341.
McNeely MJ, Shofer JB, Leonetti DL, Fujimoto WY, Boyko EJ . Associations among visceral fat, all-cause mortality, and obesity-related mortality in Japanese Americans. Diabetes Care 2012; 35: 296–298.
Katzmarzyk PT, Bray GA, Greenway FL, Johnson WD, Newton RL, Ravussin E et al. Racial differences in abdominal depot-specific adiposity in white and African American adults. Am J Clin Nutr 2010; 91: 7–15.
Smith SR, Lovejoy JC, Greenway F, Ryan D, deJonge L, de la Bretonne J et al. Contributions of total body fat, abdominal subcutaneous adipose tissue compartments, and visceral adipose tissue to the metabolic complications of obesity. Metabolism 2001; 50: 425–435.
MacMahon B . The National Death Index. Am J Public Health 1983; 73: 1247–1248.
Muzumdar R, Allison DB, Huffman DM, Ma X, Atzmon G, Einstein FH et al. Visceral adipose tissue modulates mammalian longevity. Aging Cell 2008; 7: 438–440.
Kay SJ, Fiatarone Singh MA . The influence of physical activity on abdominal fat: a systematic review of the literature. Obes Rev 2006; 7: 183–200.
Kaul S, Rothney MP, Peters DM, Wacker WK, Davis CE, Shapiro MD et al. Dual-energy X-ray absorptiometry for quantification of visceral fat. Obesity 2012; 20: 1313–1318.
Acknowledgements
We gratefully acknowledge the contributions of the many clinical scientists and staff of the Pennington Biomedical Research Center who have contributed data to the PCLS. PK is supported, in part, by the Louisiana Public Facilities Authority Endowed Chair in Nutrition and CB is funded, in part, by the John W Barton, Sr Endowed Chair in Genetics and Nutrition. This work was partially supported by a NORC Center grant no. 2P30-DK072476-06 entitled ‘Nutritional Programming: Environmental and Molecular Interactions’ sponsored by NIDDK. The PCLS is registered at ClinicalTrials.gov (identifier NCT00959270).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Katzmarzyk, P., Mire, E. & Bouchard, C. Abdominal obesity and mortality: The Pennington Center Longitudinal Study. Nutr & Diabetes 2, e42 (2012). https://doi.org/10.1038/nutd.2012.15
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2012.15
Keywords
This article is cited by
-
Investigation the interaction of dietary fat quality indices and the MC4R gene in metabolically healthy and unhealthy overweight and obese women
Scientific Reports (2023)
-
Body fat and risk of all-cause mortality: a systematic review and dose-response meta-analysis of prospective cohort studies
International Journal of Obesity (2022)
-
Comparison of abdominal visceral adipose tissue measurements in adolescents between magnetic resonance imaging and dual-energy X-ray absorptiometry
International Journal of Obesity (2021)
-
Effects of lutein supplementation on inflammatory biomarkers and metabolic risk factors in adults with central obesity: study protocol for a randomised controlled study
Trials (2020)
-
Contribution of genetics to visceral adiposity and its relation to cardiovascular and metabolic disease
Nature Medicine (2019)
