
Key Points
-
The main fields of use of robotic technology in cardiovascular medicine are endoscopic cardiac and vascular surgery, endovascular surgery, catheter-based ablation therapy for atrial fibrillation, and percutaneous coronary intervention
-
Robotic devices enable complex endoscopic reconstructive manoeuvres in narrow spaces and can increase surgical precision; however, robotically assisted totally endoscopic approaches in cardiac and vascular surgery are technically challenging
-
In catheter-based interventions, robotic technology leads to improved catheter stability and reduced radiation exposure to both intervention teams and patients
-
All robotically assisted cardiovascular surgical procedures and catheter-based interventions involve a learning curve, during which conversion rates to conventional techniques and operative times are reduced
-
Prospective, randomized trials to compare robotic and conventional approaches are lacking; observational studies and nonrandomized comparative studies show basic feasibility and safety of robotic interventions and intermediate-term results are promising
Abstract
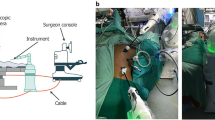
Robotic technology has been used in cardiovascular medicine since the late 1990s. Interventional cardiology, electrophysiology, endovascular surgery, minimally invasive cardiac surgery, and laparoscopic vascular surgery are all fields of application. Robotic devices enable endoscopic reconstructive surgery in narrow spaces and fast, very precise placement of catheters and devices in catheter-based interventions. In all robotic systems, the operator manipulates the robotic arms from a control station or console. In the field of cardiac surgery, mitral valve repair, CABG surgery, atrial septal defect repair, and myxoma resection can be achieved using robotic technology. Furthermore, vascular surgeons can perform a variety of robotically assisted operations to treat aortic, visceral, and peripheral artery disease. In electrophysiology, ablation procedures for atrial fibrillation can be carried out with robotic support. In the past few years, robotically assisted percutaneous coronary intervention and abdominal aortic endovascular surgery techniques have been developed. The basic feasibility and safety of robotic approaches in cardiovascular medicine has been demonstrated, but learning curves and the high costs associated with this technology have limited its widespread use. Nonetheless, increased procedural speed, accuracy, and reduced exposure to radiation and contrast agent in robotically assisted catheter-based interventions, as well as reduced surgical trauma and shortened patient recovery times after robotic cardiovascular surgery are promising achievements in the field.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others


References
Granada, J. F. et al. First-in-human evaluation of a robotic-assisted coronary angioplasty system. JACC Cardiovasc. Interv. 4, 460–465 (2011).
Weisz, G. et al. Safety and feasibility of robotic percutaneous coronary intervention: PRECISE (Percutaneous Robotically-Enhanced Coronary Intervention) Study. J. Am. Coll. Cardiol. 61, 1596–1600 (2013).
Saliba, W. et al. Novel robotic catheter remote control system: feasibility and safety of trans-septal puncture and endocardial catheter navigation. J. Cardiovasc. Electrophysiol. 17, 1102–1105 (2006).
Saliba, W. et al. Atrial fibrillation ablation using a robotic catheter remote control system: initial human experience and long-term follow-up results. J. Am. Coll. Cardiol. 51, 2407–2411 (2008).
Wazni, O. M. et al. Experience with the Hansen robotic system for atrial fibrillation ablation—lessons learned and techniques modified: Hansen in the real world. J. Cardiovasc. Electrophysiol. 20, 1193–1196 (2009).
Bai, R. et al. Worldwide experience with the robotic navigation system in catheter ablation for atrial fibrillation: methodology, efficacy and safety. J. Cardiovasc. Electrophysiol. 23, 820–826 (2012).
Valderrábano, M., Dave, A. S., Báez-Escudero, J. L. & Rami, T. Robotic catheter ablation of left ventricular tachycardia: initial experience. Heart Rhythm 8, 1837–1846 (2011).
Di Biase, L. et al. Mapping and ablation of ventricular arrhythmias with magnetic navigation: comparison between 4- and 8-mm catheter tips. J. Interv. Card. Electrophysiol. 26, 133–137 (2009).
Bradfield, J., Tung, R., Mandapati, R., Boyle, N. G. & Shivkumar, K. Catheter ablation utilizing remote magnetic navigation: a review of applications and outcomes. Pacing Clin. Electrophysiol. 35, 1021–1034 (2012).
Kleine P. et al. Robotically enhanced placement of left ventricular epicardial electrodes during implantation of a biventricular implantable cardioverter defibrillator system. Pacing. Clin. Electrophysiol. 25, 989–991 (2002).
Jansens, J. L. et al. Robotic-enhanced biventricular resynchronization: an alternative to endovenous cardiac resynchronization therapy in chronic heart failure. Ann. Thorac. Surg. 76, 413–417 (2003).
DeRose, J. et al. Robotically assisted left ventricular epicardial lead implantation for biventricular pacing: the posterior approach. Ann. Thorac. Surg. 77, 1472–1474 (2004).
Mair, H. et al. Epicardial lead implantation techniques for biventricular pacing via left lateral mini-thoracotomy, video-assisted thoracoscopy, and robotic approach. Heart Surg. Forum 6, 412–417 (2003).
Kamath, G. S. et al. Long-term outcome of leads and patients following robotic epicardial left ventricular lead placement for cardiac resynchronization therapy. Pacing Clin. Electrophysiol. 34, 235–240 (2010).
Bismuth, J., Kashef, E., Cheshire, N. & Lumsden, A. B. Feasibility and safety of remote endovascular catheter navigation in a porcine model. J. Endovasc. Ther. 18, 243–249 (2011).
Riga, C. V., Cheshire, N. J., Hamady, M. S. & Bicknell, C. D. The role of robotic endovascular catheters in fenestrated stent grafting. J. Vasc. Surg. 51, 810–819 (2010).
Riga, C. V., Bicknell, C. D., Hamady, M. S. & Cheshire, N. J. Evaluation of robotic endovascular catheters for arch vessel cannulation. J. Vasc. Surg. 54, 799–809 (2011).
Riga, C., Bicknell, C., Cheshire, N. & Hamady, M. Initial clinical application of a robotically steerable catheter system in endovascular aneurysm repair. J. Endovasc. Ther. 16, 149–153 (2009).
Lumsden, A. B. et al. Robot-assisted stenting of a high-grade anastomotic pulmonary artery stenosis following single lung transplantation. J. Endovasc. Ther. 17, 612–616 (2010).
Carrell, T., Dastur, N., Salter, R. & Taylor, P. Use of a remotely steerable “robotic” catheter in a branched endovascular aortic graft. J. Vasc. Surg. 55, 223–225 (2012).
Riga, C. V., Bicknell, C. D., Rolls, A., Cheshire, N. J. & Hamady, M. S. Robot-assisted fenestrated endovascular aneurysm repair (FEVAR) using the Magellan system. J. Vasc. Interv. Radiol. 24, 191–196 (2013).
Bismuth, J., Duran, C., Stankovic, M., Gersak, B. & Lumsden, A. B. A first-in-man study of the role of flexible robotics in overcoming navigation challenges in the iliofemoral arteries. J. Vasc. Surg. 57 (Suppl. 2), 14S–19S (2013).
Riga, C. V. et al. Endovascular robotic intervention: clinical feasibility and safety profiles. Presented at The British Society of Endovascular Therapy 2013 Annual Meeting.
Stevens, J. H. et al. Port-access coronary artery bypass with cardioplegic arrest: acute and chronic canine studies. Ann. Thorac. Surg. 62, 435–440 (1996).
Loulmet, D. et al. Endoscopic coronary artery bypass grafting with the aid of robotic assisted instruments. J. Thorac. Cardiovasc. Surg. 118, 4–10 (1999).
Damiano, R. J. Robotics in cardiac surgery: the emperor's new clothes. J. Thorac. Cardiovasc. Surg. 134, 559–561 (2007).
Robicsek, F. Robotic cardiac surgery: time told! J. Thorac. Cardiovasc. Surg. 135, 243–145 (2008).
Mihaljevic, T. et al. Robotic posterior mitral leaflet repair: neochordal versus resectional techniques. Ann. Thorac. Surg. 95, 787–794 (2013).
Nifong, L. W., Rodriguez, E. & Chitwood, W. R. 540 consecutive robotic mitral valve repairs including concomitant atrial fibrillation cryoablation. Ann. Thorac. Surg. 94, 38–42 (2012).
Murphy, D. et al. Multicenter mitral valve study: a lateral approach using the da Vinci surgical system. Innovations (Phila.) 2, 56–61 (2007).
Mihaljevic T. et al. Robotic repair of posterior mitral valve prolapse versus conventional approaches: potential realized. J. Thorac. Cardiovasc. Surg. 141, 72–80 (2011).
Sutter, F. P., Berry, T. & Wertan, T. Precision incision: robotic coronary revascularization via 3.9 cm minithoracotomy. Innovations (Phila.) 7, 223–228 (2012).
Srivastava, S. et al. Beating heart totally endoscopic coronary artery bypass. Ann. Thorac. Surg. 89, 1873–1880 (2010).
Srivastava, S., Barrera, R. & Quismundo, S. One hundred sixty-four consecutive beating heart totally endoscopic coronary artery bypass cases without intraoperative conversion. Ann. Thorac. Surg. 94, 1463–1468 (2012).
Bonaros, N. et al. Five hundred cases of robotic totally endoscopic coronary artery bypass grafting: predictors of success and safety. Ann. Thorac. Surg. 95, 803–812 (2013).
Bonatti, J. et al. Totally endoscopic quadruple coronary artery bypass grafting is feasible using robotic technology. Ann. Thorac. Surg. 93, e111–e112 (2012).
de Cannière, D. et al. Feasibility, safety, and efficacy of totally endoscopic coronary artery bypass grafting: multicenter European experience. J. Thorac. Cardiovasc. Surg. 134, 710–716 (2007).
Balkhy, H. H., Wann, L. S., Krienbring, D. & Arnsdorf, S. E. Integrating coronary anastomotic connectors and robotics toward a totally endoscopic beating heart approach: review of 120 cases. Ann. Thorac. Surg. 92, 821–827 (2011).
Dhawan, R. et al. Multivessel beating heart robotic myocardial revascularization increases morbidity and mortality. J. Thorac. Cardiovasc. Surg. 143, 1056–1061 (2012).
Bonatti, J. et al. Hybrid coronary revascularization using robotic totally endoscopic surgery: perioperative outcomes and 5-year results. Ann. Thorac. Surg. 94, 1920–1926 (2012).
Torracca, L., Ismano, G. & Alfieri, O. Totally endoscopic computer-enhanced atrial septal defect closure in six patients. Ann. Thorac. Surg. 72, 1354–1357 (2001).
Wimmer-Greinecker, G. et al. Totally endoscopic atrial septal repair in adults with computer-enhanced telemanipulation. J. Thorac. Cardiovasc. Surg. 126, 465–468 (2003).
Argenziano, M. et al. Totally endoscopic atrial septal defect repair with robotic assistance. Circulation 108 (Suppl. 1), II-191–II-194 (2003).
Bonaros, N. et al. Robotically assisted totally endoscopic atrial septal defect repair: insights from operative times, learning curves, and clinical outcome. Ann. Thorac. Surg. 82, 687–693 (2006).
Gao, C. et al. Totally endoscopic robotic ventricular septal defect repair. Innovations (Phila.) 5, 278–280 (2010).
Chakraborty, B., Burkhart, H. M., Warnes, C. A. & Suri, R. Successful robotic-assisted division of symptomatic vascular ring. Heart Surg. Forum 15, E306 (2012).
Gao, C. et al. Excision of atrial myxoma using robotic technology. J. Thorac. Cardiovasc. Surg. 139, 1282–1285 (2010).
Schilling, J., Engel, A. M., Hassan, M. & Smith, J. M. Robotic excision of atrial myxoma. J. Card. Surg. 27, 423–426 (2012).
Štádler, P., Šebesta, P., Vitásek, P., Matouš, P. & El Samman, K. A modified technique of transperitoneal direct approach for totally laparoscopic aortoiliac surgery. Eur. J. Vasc. Endovasc. Surg. 3, 266–269 (2006).
Stádler, P., Dvoracek, L., Vitasek, P. & Matous, P. Robotic vascular surgery, 150 cases. Int. J. Med. Robot. 4, 394–398 (2010).
Novotný, T., Dvorák, M. & Staffa, R. The learning curve of robot-assisted laparoscopic aortofemoral bypass grafting for aortoiliac occlusive disease. J. Vasc. Surg. 2, 414–420 (2011).
Lin, J. C. et al. Robotic-assisted aortic surgery with and without minilaparotomy for complicated occlusive disease and aneurysm. J. Vasc. Surg. 1, 16–22 (2012).
Bonaros, N. et al. Quality of life improvement after robotically assisted coronary artery bypass grafting. Cardiology 114, 59–66 (2009).
Schachner, T. et al. Training surgeons to perform robotically assisted totally endoscopic coronary surgery. Ann. Thorac. Surg. 88, 523–527 (2009).
Author information
Authors and Affiliations
Contributions
All the authors researched data for the article, contributed substantially to the discussion of content, wrote the manuscript, and reviewed/edited the article before submission.
Corresponding author
Ethics declarations
Competing interests
G.V. is an investigator in the PECISE trial for Corindus Vascular Robotics. C.R. is a consultant for Hansen Medical, and has received educational fees from Gore Medical and Medtronic. The other authors declare no competing interests.
Rights and permissions
About this article
Cite this article
Bonatti, J., Vetrovec, G., Riga, C. et al. Robotic technology in cardiovascular medicine. Nat Rev Cardiol 11, 266–275 (2014). https://doi.org/10.1038/nrcardio.2014.23
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrcardio.2014.23
This article is cited by
-
Dip-coating electromechanically active polymer actuators with SIBS from midblock-selective solvents to achieve full encapsulation for biomedical applications
Scientific Reports (2022)
-
Comparison of manual versus robot-assisted contralateral gate cannulation in patients undergoing endovascular aneurysm repair
International Journal of Computer Assisted Radiology and Surgery (2020)
-
Aortic dissection
Nature Reviews Disease Primers (2016)
