
Abstract
The neurochemical underpinnings of sleep’s contribution to the establishment and maintenance of memory traces are largely unexplored. Considering that intranasal insulin administration to the CNS improves memory functions in healthy and memory-impaired humans, we tested whether brain insulin signaling and sleep interact to enhance memory consolidation in healthy participants. We investigated the effect of intranasal insulin on sleep-associated neurophysiological and neuroendocrine parameters and memory consolidation in 16 men and 16 women (aged 18–30 years), who learned a declarative word-pair task and a procedural finger sequence tapping task in the evening before intranasal insulin (160 IU) or placebo administration and 8 h of nocturnal sleep. On the subsequent evening, they learned interfering word-pairs and a new finger sequence before retrieving the original memories. Insulin increased growth hormone concentrations in the first night-half and EEG delta power during the second 90 min of non-rapid-eye-movement sleep. Insulin treatment impaired the acquisition of new contents in both the declarative and procedural memory systems on the next day, whereas retrieval of original memories was unchanged. Results indicate that sleep-associated memory consolidation is not a primary mediator of insulin’s acute memory-improving effect, but that the peptide acts on mechanisms that diminish the subsequent encoding of novel information. Thus, by inhibiting processes of active forgetting during sleep, central nervous insulin might reduce the interfering influence of encoding new information.
Similar content being viewed by others

Introduction
The consolidation of memory contents, ie, the strengthening and reprocessing of encoded information, has been shown to strongly rely on the brain’s offline processing during sleep (Diekelmann and Born, 2010). It is assumed that neuronal ensembles involved in information encoding during wakefulness are reactivated during subsequent sleep, strengthening respective memory representations (Diekelmann and Born, 2010). This concept relies on findings in rodents that firing patterns of hippocampal and cortical neurons observed during task performance while the animal is awake re-emerge during non-rapid-eye-movement (NonREM) sleep (Ji and Wilson, 2007; Wilson and McNaughton, 1994) and that re-exposing human participants during slow wave sleep to cues associated with the prior learning experience enhances sleep-dependent memory consolidation (Oudiette and Paller, 2013). Notwithstanding intense research efforts, the neurochemical mechanisms underlying sleep-dependent memory consolidation have only been partially unraveled (Abel et al, 2013). Sleep provides a unique neurochemical milieu, and fluctuations in plasticity-promoting neuromodulators like cortisol, acetylcholine, serotonin, and norepinephrine have been found to contribute to sleep-dependent memory consolidation (eg, Gais and Born, 2004; Groch et al, 2011; Plihal and Born, 1999; Rasch et al, 2009), which moreover is subject to a modulatory influence by glutamatergic and GABAergic transmission (eg, Feld et al, 2013a, b; Gais et al, 2008).
The pancreatic hormone insulin, a major factor in the maintenance of energy homeostasis, has turned out to be an important neuromodulator, regulating among others metabolic function (Bruning et al, 2000) and neuronal plasticity (Chiu and Cline, 2010). Insulin reaches the CNS via saturable transport mechanisms but does not appear to be released in large amounts within the brain (Gray et al, 2014), although indicators of local insulin production in the cerebral cortex have been found in animals (Molnar et al, 2014). Central nervous insulin receptors are expressed in high densities in structures like the olfactory bulb, the hypothalamus, and, notably, the hippocampal formation (Devaskar et al, 1994), which is essential for the initial formation and storage of declarative memory, ie, memory for episodes that is accessible to conscious recollection. Accordingly, central nervous insulin administration via the intranasal pathway (Born et al, 2002; Dhuria et al, 2010) has been repeatedly found to improve memory function in healthy subjects when delivered acutely (Benedict et al, 2008; Brunner et al, 2015) or for 8 weeks (Benedict et al, 2004, 2007) and, moreover, in patients suffering from mild cognitive impairments and early Alzheimer’s disease (Craft et al, 2012; Reger et al, 2008a, for review see De Felice, 2013). Memory-improving effects of insulin have been suggested to be mediated via changes in hippocampal synaptic plasticity including long-term depression and potentiation (Moult and Harvey, 2008), with potential contributions from enhanced neuronal glucose utilization (Doyle et al, 1995). However, the exact preconditions and mechanisms of insulin-induced memory improvements have remained largely unexplored.
Considering that insulin interacts with neuroendocrine factors like cortisol (Benedict et al, 2004; Bohringer et al, 2008) and growth hormone (Gahete et al, 2013), which are secreted in a circadian/sleep-dependent manner, in the present study, we aimed to clarify whether brain insulin signaling contributes to sleep-dependent memory formation, and how central nervous insulin administration via the intranasal pathway affects sleep-associated neuroendocrine regulation. Since previous studies have indicated that men and women respond differently to insulin’s central nervous effects (Benedict et al, 2008; Hallschmid et al, 2004; Krug et al, 2010), we investigated the impact of pre-sleep intranasal insulin administration in male and female participants.
Materials and methods
Participants
A total of 32 young healthy, non-smoking, native German speaking participants (16 males and 16 females) completed the study (for details, see Supplementary Methods), which was approved by the local ethics committee. Written informed consent was obtained from all participants before participation.
Study Design and Procedure
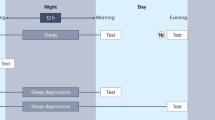
The experiment followed a balanced, double-blind, placebo-controlled, within-subject, crossover design. All participants took part in two experimental sessions, which were identical except for the intranasal administration of insulin (Actrapid, Novo Nordisk, Bagsværd, Denmark) or placebo (insulin carrier solution). During participation, all the women were taking estrogen-dominant oral contraceptives. Experimental sessions were scheduled to be apart as close to 28 days as possible (men, median, 28 days, range 27–35 days; women, median, 28 days, range 25–28 days), ensuring that the women were tested during the same phase of contraceptive intake in both sessions (see Supplementary Methods for details). Sessions were performed in a balanced order, ie, half of the sample received first placebo and then the active agent, with the reversed order for the other half of the sample. The experimental procedure is summarized in Figure 1a and described in detail in the Supplementary Methods. In brief, at 2120 hours of the first evening, participants memorized declarative (word-pairs) and procedural (finger sequence tapping) contents before receiving intranasal insulin (or placebo) via 16 0.1-ml puffs (8 per nostril) in 1-min intervals, amounting to a total dose of 1.6 ml insulin (160 IU) or placebo at 2220 hours. Subjects went to bed at 2300 hours for 8 h of sleep that was recorded polysomnographically. At 1800 hours on the subsequent evening they learned interfering contents before retrieval of the contents learned before sleep and of the interfering information. Throughout the session, blood was repeatedly sampled for the determination of relevant parameters and mood and vigilance were assessed.

(a) Overview over the experimental procedure. (b) Mean (+SEM) absolute amounts of word-pairs remembered in the interference learning task in the evening after sleep, tested at learning and retrieval in the insulin (red) and placebo (black) conditions. (c) Mean (±SEM) differences between learning and retrieval performances of the interference word-pair task for insulin (red) and placebo (black). (d) Mean (±SEM) absolute amounts of correct sequences tapped in the interference learning task in the evening after sleep for each tapping block in the insulin (red) and placebo (black) conditions. Bar-plot inserts depict mean (±SEM) numbers of correct sequences during blocks 10–12 of learning and blocks 1–3 of retrieval. **P⩽0.01, *P⩽0.05, tP⩽0.10. N=32 (16 men and 16 women).
Memory Tasks
Declarative memory was investigated with a word-pair interference paradigm (see Supplementary Methods for details). During the first evening, participants learned a list of 20 cue words associated with unrelated target words (A-B) up to a criterion of 90% correct responses. On the subsequent evening they learned 20 interfering associations of the original cue words with completely new, unrelated target words (A-C), again until a criterion of 90% correct answers was reached. Afterwards, the original and the new associations were retrieved. For procedural memory testing, a finger sequence tapping task was used (for details see Supplementary Methods). On the first evening, participants learned a 5-element finger sequence by tapping it on a keyboard during 12 30-s blocks. On the subsequent evening, the participants learned a different 5-element sequence. Afterwards, both sequences were tested independently during additional three blocks.
Blood Analyses
Blood glucose levels and circulating concentrations of growth hormone and insulin were determined at two time points before substance administration and repeatedly thereafter (see Supplementary Methods). To adjust for baseline concentrations, individual averages across the 2115 hours and 2215 hours baseline values were subtracted from post-administration concentrations. For display purposes, the resulting differences were referenced to a common baseline. Pairwise comparisons between conditions were performed for each sampling time point as well as for the peak in growth hormone concentrations during the first night-half expressed as the area under the curve (AUC) calculated according to the trapezoidal rule between 2320 hours and 0320 hours.
Sleep Analyses
Sleep architecture was determined according to standard polysomnographic criteria using EEG recordings from C3 and C4, diagonal EOG, and chin EMG (Rechtschaffen and Kales, 1968, details provided in the Supplementary Methods). For each night, total sleep time, ie, the time between the first detection of transition from sleep stage 1 to 2 and lights on, was used to calculate relative time spent in the different sleep stages, ie, wake, rapid eye movement (REM) sleep, and NonREM sleep stages 1, 2, 3, and 4.
Average power spectra were calculated at C3 and C4 for the first and the second 90 min of NonREM sleep. Normalized power spectra (ie, each frequency bin was normalized by the total power between 0.5 and 50 Hz) were calculated by Fast Fourier Transformation with a Hanning window applied to subsequent blocks of 2048 data points (~10.24 s, 3 blocks per 30 s epoch). The averaged spectra for each participant were filtered by a 5-point moving average to produce a smoothing of the FFT outcome. In the averaged spectra, mean power was determined for 0.5–1 Hz slow oscillations, 1–4 Hz delta and the 12–15 Hz sleep spindle frequency bands for NonREM sleep and in the 4–8 Hz theta band for REM sleep.
Control Measures
Vigilance, sleepiness, mood, hunger, and thirst were repeatedly assessed with a reaction time task, the Stanford Sleepiness Scale, and visual analogue scales, respectively. General retrieval function was measured at retrieval using a word generation task (for details, see Supplementary Methods). At the end of each experimental session, participants were asked whether they thought they had received insulin or placebo.
Statistical Analysis
For the analysis of sleep stages one female and one male participant were excluded because of partial data loss due to recorder malfunction. One male and three female participants were excluded from the EEG power analyses because of insufficient amounts of artifact-free data. For the analyses of blood parameters, two female participants were excluded because of insufficient data and one male participant was excluded from growth hormone analysis because 7 out of 20 values in the placebo condition were identified as outliers (ie, deviated from the mean by more than two standard deviations). Vigilance task data from four female participants could not be analyzed because of data loss. Exclusion of these participants did not alter the overall structure of the results. Statistical analyses generally relied on analyses of variance (SPSS version 21.0.0 for Windows) including the repeated measures factors ‘treatment’ (insulin vs placebo) and ‘time point’ as appropriate, and the between-subjects factor sex (men vs women). Degrees of freedom were corrected according to the Greenhouse-Geisser procedure where appropriate. Pairwise comparisons were specified by t-tests unless stated otherwise. Pearson product-moment correlations were calculated to assess relationships between neuroendocrine, sleep-related, and behavioral parameters.
Results
Memory Tasks
Whereas intranasal insulin administration did not affect the retrieval of declarative and procedural memory traces acquired before sleep, it impaired the capacity to encode interfering material in the evening following the experimental sleep night. Thus, intranasal insulin did not affect the number of recalled word-pairs learned before sleep (all F(1,30)⩽1, p⩾0.62; see Table 1 for descriptive data and pairwise comparisons). In general, participants produced less word-pairs at retrieval than at encoding (F(1,30)=111.45 and p⩽0.001) and women outperformed men (F(1,30)=23.22, p⩽0.001), especially at retrieval (F(1,30)=23.08, p⩽0.001). Women also performed better at the retrieval of the interfering word-pairs learned in the evening (F(1,30)=6.03 and p=0.02; Figure 1b). Across all subjects, insulin treatment induced a trend-wise reduction in the amount of interfering word-pairs retrieved after sleep (F(1,30)=3.07, p=0.09), which was driven by the men showing significantly impaired retrieval of the newly acquired interference word-pairs in the insulin condition (F(1,30)=7.41, p=0.011 for treatment × sex × time point). Accordingly, men in contrast to women displayed a trend toward an insulin-induced impairment, whereas women showed signs of an improvement in performance occurring between encoding and retrieval of the interfering word-pairs (Figure 1c). There was a trend toward a positive relationship between the overnight retention of word-pairs encoded before sleep and the retention of interfering word-pairs for treatment-induced differences in the men (r=0.48, p=0.06).
In the finger sequence tapping task learned before sleep, participants improved across the retention interval in both conditions (F(1,30)=29.59 and p⩽0.001), indicating that insulin did not affect its consolidation (all F(1,30)⩽1, p⩾0.43; Table 1). However, insulin impaired performance on the interfering finger sequence tapping task learned in the subsequent evening (F(1,30)=6.47 and p=0.016; Figure 1d), whereas all participants still improved from learning to retrieval (F(1,30)=28.52 and p⩽0.001). This effect was independent of sex (all F(1,30)⩽1.39, p⩾0.25). There was no effect of insulin on error rates in the finger sequence tapping task learned before sleep (all F⩽1.4, p⩾0.23) or after sleep (all F⩽2.74, p⩾0.11; see Supplementary Table 1).
Blood Parameters
Baseline values of all blood parameters determined at 2115 hours and 2215 hours did not differ between conditions (all p>0.14). Intranasal insulin administration induced a sustained increase in growth hormone concentrations depending on point of time (F(19,513)=4.66, p⩽0.01; Figure 2a). Accordingly, growth hormone AUC values for the first night-half (2320–0320 h; Figure 2b) were increased by insulin (F(1,27)=5.14, p=0.03). Sex did not significantly modulate this effect (F⩽1, p=0.34 for treatment × sex; men, t(14)=2.90, p=0.012; women, t⩽1, p=0.46).

(a) Mean (±SEM) serum growth hormone concentrations following the intranasal administration of insulin (160 IU; red lines) and placebo (black lines). N=29 (15 men and 14 women). Substance administration from 2220 to 2235 hours is indicated by the green bar. (b) AUC (+SEM) of serum growth hormone concentrations during the first half of the night (2320–0320 hours) in the insulin (red bars) and placebo (black bars) conditions. (c, d) Mean (±SEM) serum insulin and blood glucose concentrations in the insulin (red lines) and placebo (black lines) conditions. N=30 (16 men and 14 women). All data were individually baseline adjusted with reference to measurements at 2115 and 2215 hours. **P⩽0.01, *P⩽0.05, tP⩽0.10.
Serum insulin levels in general slightly decreased throughout the night (F(19,532)=12.13, p⩽0.001; Figure 2c and Supplementary Figure 1A). Intranasal insulin in comparison to placebo administration induced a transient increase in insulin concentrations immediately after substance administration at 2235 hours (t(29)=4.32, p⩽0.001; F(19,532)=5.27 p⩽0.001 for treatment × time point), whereas insulin levels were closely comparable between conditions during the rest of the night. At retrieval testing on the subsequent afternoon, insulin levels tended to be lower in the insulin compared with the placebo condition (t(29)=−1.84, p=0.08). Blood glucose concentrations decreased until dawn (F(19,532)=9.50 p⩽0.001; Figure 2d and Supplementary Figure 1B) and showed a transient decrease after intranasal insulin compared with placebo administration (2300 hours: t(29)=−2.96, p⩽0.01; 2320 hours: t(29)=−2.14, p=0.04; F(19,532)=2.78, p=0.012 for treatment × time point). Signs of decreased blood glucose levels in the insulin compared with the placebo condition in the male participants (Supplementary Figure 1B) were not confirmed by respective overall analyses (p>0.42), which neither indicated systematic treatment-related differences between sexes (p>0.17).
Correlational analyses covering the whole sample of participants revealed that the treatment-induced increases observed for growth hormone during the first night-half (AUCgrowth hormone 2320–0320 hours) and for serum insulin immediately after substance administration (2235 hours) were inversely related (r=−0.43, p⩽0.05). Respective correlations between the growth hormone AUC and the treatment-induced drop in blood glucose levels (mean level at 2300 hours and 2320 hours) did not reach significance (r=−0.32, p=0.09).
Sleep
Intranasal insulin administration did not influence polysomnographically determined sleep stages in the whole sample of subjects (all t⩽1, p⩾0.71; Table 2). The female participants showed a trend toward less REM sleep in the insulin compared with the placebo condition (t(14)=−1.82, p=0.096; see Supplementary Tables 2 and 3 for results in men and women, respectively). Control measures indicated that subjective sleepiness assessed in the afternoon after the experimental night was decreased in the insulin condition (see Supplementary Results).
A more fine-grained polysomnographic analysis of EEG power between 0.1 and 35 Hz revealed that intranasal insulin increased the amount of delta power in the second 90 min cycle of NonREM sleep in males. Thus, insulin induced a significant increase in EEG power in the delta range (1–4 Hz) at both electrode locations (C3 and C4) during the second 90 min of NonREM sleep, and a reduction in the spindle band (12–15 Hz) at C3 during the first 90 min of NonREM sleep (see Figure 3 for the total sample and Supplementary Figures 2 and 3 for men and women, respectively). The insulin-induced increase in delta band power during the second 90 min of NonREM sleep was driven by an effect in the male participants (C3: t(14)=3.08, p⩽0.01; C4: t(14)=3.24, p⩽0.01; Figure 3d). Accordingly, there was a significant interaction between the factors treatment, sex, and time point (F(1,25)=4.36, p⩽0.05). There was no significant relation between the insulin-induced increase in growth hormone concentrations during the first night-half and the increase in delta power during the second NonREM cycle (p>0.38). There was also no effect of insulin on theta power during REM sleep (all p>0.20). See Table 3 for a summary of the observed effects.

EEG power during NonREM sleep. (a, c) Mean (±SEM) normalized EEG power between 0.5 and 20 Hz for electrode positions C3 (left) and C4 (right) in the insulin (red) and placebo (black) conditions during (a) the first 90 min and (c) the second 90 min of NonREM sleep; respective inserts show EEG power between 1.5 and 3 Hz. Below each panel, p-values for pairwise comparisons between conditions for each frequency bin (0.01 Hz) are indicated. (b, d) Mean (±SEM) cumulative EEG power in the delta band (1–4 Hz) at C3 and C4 electrode positions in the insulin (red) and placebo (black) condition during (b) the first 90 min and (d) the second 90 min of NonREM sleep recorded in the total sample of subjects as well as the men and women. N=28 (15 men and 13 women). **P⩽0.01, *P⩽0.05.
Discussion
The present study aimed at investigating whether central nervous insulin signaling interacts with the beneficial effect of sleep on memory consolidation by administering intranasal insulin to healthy subjects between learning declarative and procedural memory contents and a retention interval containing 8 h of nocturnal sleep. Insulin treatment increased growth hormone concentrations during the first night-half and relative EEG delta band power during the second NonREM sleep cycle. Insulin did not directly affect measures of sleep-dependent declarative or procedural memory consolidation but impaired the delayed acquisition of new declarative and procedural memory contents that interfered with the memory traces learned before sleep. These findings suggest that the improving effect of intranasal insulin administration on memory function observed in previous studies (Benedict et al, 2004, 2007; Craft et al, 2012; Reger et al, 2008b) is not primarily conveyed by sleep-dependent mechanisms, although central nervous insulin delivery impacts neuroendocrine and neurophysiological sleep patterns.
The predominance in men rather than women of insulin’s effects on sleep-associated neurophysiology and subsequent cognitive function ties in with previous observations of sex differences in the response to intranasal insulin in the metabolic and cognitive domain (Benedict et al, 2008; Hallschmid et al, 2004; Krug et al, 2010). Notably, immediate improving effects of intranasal insulin on declarative memory were found in healthy women (on estrogen-dominant oral contraceptives), whereas men did not benefit (Benedict et al, 2008). Fittingly, in the insulin condition of the present study, female participants showed a trend toward enhanced memory for interfering declarative contents, whereas men rather displayed deterioration. Interestingly, sex differences and an influence of the menstrual cycle have also been found for the general effect of sleep on memory function (Genzel et al, 2012). As all female participants of the present study were taking contraceptives, additional studies in free cycling women are needed to obtain further insight into this pattern. Here, the inclusion of wake control groups, which was not done in the present study, would further substantiate the critical involvement of sleep-dependent processes. Moreover, it remains to be seen whether long-term intranasal insulin administration impacts sleep-related memory formation.
Beneficial effects of insulin on memory function can be attributed to insulin receptors located in brain regions relevant for memory formation, such as the hippocampus and connected limbic brain structures (Unger et al, 1991). Insulin can induce AMPA receptor internalization, which leads to long-term depression (Man et al, 2000). Also, insulin phosphorylates AMPA receptors and leads to the overexpression of PKMζ (Adzovic and Domenici, 2014), and downregulating hippocampal insulin receptor function impairs long-term potentiation and spatial memory (Grillo et al, 2015). Since both long-term depression and long-term potentiation contribute to the establishment of memory traces in the hippocampus (Goh and Manahan-Vaughan, 2015; Born and Feld, 2012), insulin may exert some of its memory-improving effects by modulating these plastic processes. The strong effect of estrogen on synaptic plasticity (Baudry et al, 2012) may also interact with respective insulin effects and yield the sex differences found here and in other studies (Benedict et al, 2008; Krug et al, 2010). Insulin also potentiates NMDA receptor activity (Liu et al, 1995) via delivery of NMDA receptors to the cell surface (Skeberdis et al, 2001) and NMDA receptor phosphorylation (Christie et al, 1999). Shifts in NMDA receptor activity like this may induce long-lasting meta-plastic changes (Hulme et al, 2013). Of note, NMDA and AMPA receptors are essential for the sleep-dependent consolidation of cortical-procedural tasks (Gais et al, 2008) and NMDA receptors are involved in the sleep-dependent consolidation of declarative memories (Feld et al, 2013a). Our finding that the retrieval of memory contents is not altered by central nervous insulin administration before a retention interval containing around 7.5 h of sleep—which was obtained in a sample of sufficient size to detect also more subtle effects—suggests that insulin does not directly act on sleep-related neurochemical changes with relevance for memory formation. Alternatively, the peptide might improve memory function by enhancing regional glucose turnover (Osborne et al, 2015). Thus, four months of daily intranasal insulin delivery to adults with mild cognitive impairment or mild Alzheimer’s disease not only improved memory function but also prevented the decrease in brain glucose uptake observed in placebo-treated participants (Craft et al, 2012). Similar mechanisms might be behind acute (and therefore sleep-unrelated) enhancements of memory function in healthy (Benedict et al, 2008) and cognitively impaired subjects (Reger et al, 2008a) and also contribute to effects of long-term treatments (Benedict et al, 2004, 2007; Reger et al, 2008b).
The intranasal insulin-induced increase in growth hormone concentrations is a new and interesting finding. In accordance with previous experiments (Benedict et al, 2011; Krug et al, 2010), intranasal insulin delivery was associated with a transient spillover of insulin into the circulation and a respective drop in blood glucose levels, which, however, clearly remained above the hypoglycemic threshold of 3.6–3.8 mmol/l where hormonal counter regulatory responses including an increase in growth hormone release are elicited (Cryer, 1997). The decrease in blood glucose did not correlate with the rise in growth hormone levels, which, moreover, was inversely rather than positively related to the increase in circulating insulin, an observation in line with animal studies indicating that insulin suppresses growth hormone release at the level of the pituitary (Gahete et al, 2013). Thus, the promotion of somatotropic activity by intranasal insulin administration to the brain most likely can be attributed to central nervous mechanisms, which to our knowledge have not been investigated so far. Interestingly, the strong increase in growth hormone concentrations—as well as central nervous insulin delivery per se—remained without immediate effect on sleep-dependent memory consolidation. Fittingly, the infusion of somatostatin during sleep effectively blocks growth hormone and insulin release in healthy humans but does not affect memory formation (Gais et al, 2006), although somatotropic activity has been repeatedly indicated to be positively related to memory function (Vitiello et al, 2006; Hallschmid et al, 2011).
As growth hormone release is strongly related to NonREM sleep (Van Cauter et al, 1998), it is tempting to speculate that the insulin-induced increase in growth hormone concentrations might have triggered the subsequent enhancement in EEG delta band power. However, the two effects were statistically unrelated, and systemic application of growth hormone or growth hormone-releasing hormone does not affect human sleep (Kern et al, 1993), which renders such a connection improbable. Nocturnal insulin secretion is entrained to NonREM sleep phases (Kern et al, 1996), and peripheral and intracerebroventricular administration of insulin to healthy and diabetic rats increases the time spent in NonREM sleep (Danguir and Nicolaidis, 1984; Sangiah et al, 1982). Although relative time spent in different sleep stages was not affected by intranasal insulin in the present study, our finding of an insulin-induced increase in delta band power during the second 90 min of NonREM sleep in the men indicates that insulin intensifies NonREM sleep also in humans. Specifically, the occurrence of this increase in the second 90 min of NonREM sleep may be the result of central nervous insulin interfering with the homeostatic reduction of sleep pressure that normally manifests in waning delta band activity during the night (Borbely and Achermann, 1999). The absence of a respective effect in women may be related to estrogen that is known to alter sleep architecture and homeostatic regulation in rats (Deurveilher et al, 2011). Insulin has been found to be expressed in GABAergic neurogliaform cells in rodent cerebral cortex (Molnar et al, 2014) and can lead to rapid insertion of post-synaptic GABAA receptors (Wan et al, 1997). Tonic GABAA-receptor activation strongly increases the amount of NonREM sleep and delta power (Lancel, 1999). Assuming that insulin enhanced delta activity via respective mechanisms in the present study, the absence of a directly measurable effect on memory consolidation would be in line with our previous observation that inhibiting GABA re-uptake promotes slow wave activity without benefiting memory consolidation (Feld et al, 2013b).
Our finding that intranasal insulin administration before sleep compromises the learning of interfering memory contents in the subsequent evening most likely was not due to a direct effect of exogenous insulin at the retrieval session because the peptide can be assumed to have cleared the system during the preceding 20-h delay (Born et al, 2002). It might be argued that the impairment in new learning was a consequence of improved overnight consolidation interfering with encoding capacity. However, retrieval of the originally encoded word-pairs was comparable between conditions. Moreover, insulin-associated differences in the overnight retention of word-pairs were positively rather than negatively associated with respective differences in the performance on the interfering words. The enhanced brain insulin signal might rather have interacted with a supposed neurophysiological key feature of sleep, ie, its beneficial effect on subsequent new learning (Feld and Diekelmann, 2015), which is thought to be achieved by the renormalization of synaptic weights during NonREM’s slow wave sleep (Tononi and Cirelli, 2014) and REM sleep theta activity (Born and Feld, 2012). According to this theory, the encoding of new information during wakefulness is mainly achieved by widespread potentiation, which must be subsequently compensated to sustain the brain’s ability to incorporate new information. The concept that sleep, and in particular NonREM sleep, fosters the ability to learn new information has received ample empirical support (eg, Antonenko et al, 2013; Yoo et al, 2007). Moreover, REM sleep has been shown to renormalize firing rates in the hippocampus (Grosmark et al, 2012). However, in the present experiments, delta activity was increased and REM sleep theta power remained unchanged after insulin administration. Therefore, it seems more plausible that the plasticity-mediating effects of central nervous insulin outlined above exert a direct detrimental effect on the capacity to learn new contents (eg, by inducing unselective potentiation in hippocampal synapses) even when subjective tiredness is relatively reduced, as observed in the insulin condition of our study. It is well conceivable that insulin disturbs the machinery of an active decay (eg, PKMζ) that is constantly erasing irrelevant memories (Hardt et al, 2013), although clearly more work is necessary to delineate insulin’s specific effects on (sleep-related) changes in synaptic plasticity.
In sum, our study indicates that in healthy humans intranasal insulin enhances the sleep-associated rise in growth hormone concentrations but that insulin’s beneficial effect on memory function is not primarily due to acute improvements in sleep-dependent memory consolidation. This finding highlights that plastic processes during sleep can differ from the wake state, as it contrasts the acutely improving effect of intranasal insulin on memory encoding (Benedict et al, 2008; Krug et al, 2010). Still, central nervous insulin appears to act on sleep-associated mechanisms that diminish the subsequent encoding of interfering information, suggesting an involvement of changes in meta-plastic or homeostatic processes. Thus, insulin might be assumed to benefit memory formation by reducing the interfering influence of new information, eg, by perturbing processes of active forgetting during sleep. These results shed new light on the potential of intranasal insulin as a memory-aiding drug, which is the subject of an increasing number of research efforts (Spetter and Hallschmid, 2015).
Funding and disclosure
This research was supported by grants from the Deutsche Forschungsgemeinschaft (DFG; SFB 654 ‘Plasticity and Sleep’), from the German Federal Ministry of Education and Research (BMBF) to the German Center for Diabetes Research (DZD e.V.; 01GI0925), and the Helmholtz Alliance ICEMED—Imaging and Curing Environmental Metabolic Diseases (ICEMED), through the Initiative and Networking Fund of the Helmholtz Association. The funding sources had no input in the design and conduct of this study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the article. The authors declare no conflict of interest.
References
Abel T, Havekes R, Saletin JM, Walker MP (2013). Sleep, plasticity and memory from molecules to whole-brain networks. Curr Biol 23: R774–R788.
Adzovic L, Domenici L (2014). Insulin induces phosphorylation of the AMPA receptor subunit GluR1, reversed by ZIP, and over-expression of Protein Kinase M zeta, reversed by amyloid beta. J Neurochem 131: 582–587.
Antonenko D, Diekelmann S, Olsen C, Born J, Molle M (2013). Napping to renew learning capacity: enhanced encoding after stimulation of sleep slow oscillations. Eur J Neurosci 37: 1142–1152.
Baudry M, Bi X, Aguirre C (2012). Progesterone-estrogen interactions in synaptic plasticity and neuroprotection. Neuroscience 239: 280–294.
Benedict C, Brede S, Schioth HB, Lehnert H, Schultes B, Born J et al (2011). Intranasal insulin enhances postprandial thermogenesis and lowers postprandial serum insulin levels in healthy men. Diabetes 60: 114–118.
Benedict C, Hallschmid M, Hatke A, Schultes B, Fehm HL, Born J et al (2004). Intranasal insulin improves memory in humans. Psychoneuroendocrinology 29: 1326–1334.
Benedict C, Hallschmid M, Schmitz K, Schultes B, Ratter F, Fehm HL et al (2007). Intranasal insulin improves memory in humans: superiority of insulin aspart. Neuropsychopharmacology 32: 239–243.
Benedict C, Kern W, Schultes B, Born J, Hallschmid M (2008). Differential sensitivity of men and women to anorexigenic and memory-improving effects of intranasal insulin. J Clin Endocrinol Metab 93: 1339–1344.
Bohringer A, Schwabe L, Richter S, Schachinger H (2008). Intranasal insulin attenuates the hypothalamic-pituitary-adrenal axis response to psychosocial stress. Psychoneuroendocrinology 33: 1394–1400.
Borbely AA, Achermann P (1999). Sleep homeostasis and models of sleep regulation. J Biol Rhythms 14: 557–568.
Born J, Feld GB (2012). Sleep to upscale, sleep to downscale: balancing homeostasis and plasticity. Neuron 75: 933–935.
Born J, Lange T, Kern W, McGregor GP, Bickel U, Fehm HL (2002). Sniffing neuropeptides: a transnasal approach to the human brain. Nat Neurosci 5: 514–516.
Bruning JC, Gautam D, Burks DJ, Gillette J, Schubert M, Orban PC et al (2000). Role of brain insulin receptor in control of body weight and reproduction. Science 289: 2122–2125.
Brunner YF, Kofoet A, Benedict C, Freiherr J (2015). Central insulin administration improves odor-cued reactivation of spatial memory in young men. J Clin Endocrinol Metab 100: 212–219.
Chiu SL, Cline HT (2010). Insulin receptor signaling in the development of neuronal structure and function. Neural Dev 5: 7.
Christie JM, Wenthold RJ, Monaghan DT (1999). Insulin causes a transient tyrosine phosphorylation of NR2A and NR2B NMDA receptor subunits in rat hippocampus. J Neurochem 72: 1523–1528.
Craft S, Baker LD, Montine TJ, Minoshima S, Watson GS, Claxton A et al (2012). Intranasal insulin therapy for Alzheimer disease and amnestic mild cognitive impairment: a pilot clinical trial. Arch Neurol 69: 29–38.
Cryer PE (1997). Hierarchy of physiological responses to hypoglycemia: relevance to clinical hypoglycemia in type I (insulin dependent) diabetes mellitus. Horm Metab Res 29: 92–96.
Danguir J, Nicolaidis S (1984). Chronic intracerebroventricular infusion of insulin causes selective increase of slow wave sleep in rats. Brain Res 306: 97–103.
De Felice FG (2013). Alzheimer's disease and insulin resistance: translating basic science into clinical applications. J Clin Invest 123: 531–539.
Devaskar SU, Giddings SJ, Rajakumar PA, Carnaghi LR, Menon RK, Zahm DS (1994). Insulin gene expression and insulin synthesis in mammalian neuronal cells. J Biol Chem 269: 8445–8454.
Deurveilher S, Rusak B, Semba K (2011). Female reproductive hormones alter sleep architecture in ovariectomized rats. Sleep 34: 519–530.
Diekelmann S, Born J (2010). The memory function of sleep. Nat Rev Neurosci 11: 114–126.
Dhuria SV, Hanson LR, Frey WH 2nd (2010). Intranasal delivery to the central nervous system: mechanisms and experimental considerations. J Pharm Sci 99: 1654–1673.
Doyle P, Cusin I, Rohner-Jeanrenaud F, Jeanrenaud B (1995). Four-day hyperinsulinemia in euglycemic conditions alters local cerebral glucose utilization in specific brain nuclei of freely moving rats. Brain Res 684: 47–55.
Feld GB, Diekelmann S (2015). Sleep smart-optimizing sleep for declarative learning and memory. Front Psychol 6: 622.
Feld GB, Lange T, Gais S, Born J (2013a). Sleep-dependent declarative memory consolidation—unaffected after blocking NMDA or AMPA receptors but enhanced by NMDA coagonist D-cycloserine. Neuropsychopharmacology 38: 2688–2697.
Feld GB, Wilhelm I, Ma Y, Groch S, Binkofski F, Molle M et al (2013b). Slow wave sleep induced by GABA agonist tiagabine fails to benefit memory consolidation. Sleep 36: 1317–1326.
Gahete MD, Cordoba-Chacon J, Lin Q, Bruning JC, Kahn CR, Castano JP et al (2013). Insulin and IGF-I inhibit GH synthesis and release in vitro and in vivo by separate mechanisms. Endocrinology 154: 2410–2420.
Gais S, Born J (2004). Low acetylcholine during slow-wave sleep is critical for declarative memory consolidation. Proc Natl Acad Sci USA 101: 2140–2144.
Gais S, Hullemann P, Hallschmid M, Born J (2006). Sleep-dependent surges in growth hormone do not contribute to sleep-dependent memory consolidation. Psychoneuroendocrinology 31: 786–791.
Gais S, Rasch B, Wagner U, Born J (2008). Visual-procedural memory consolidation during sleep blocked by glutamatergic receptor antagonists. J Neurosci 28: 5513–5518.
Genzel L, Kiefer T, Renner L, Wehrle R, Kluge M, Grozinger M et al (2012). Sex and modulatory menstrual cycle effects on sleep related memory consolidation. Psychoneuroendocrinology 37: 987–998.
Goh JJ, Manahan-Vaughan D (2015). Role of inhibitory autophosphorylation of calcium/calmodulin-dependent kinase II (alphaCAMKII) in persistent (>24h) hippocampal LTP and in LTD facilitated by novel object-place learning and recognition in mice. Behav Brain Res 285: 79–88.
Gray SM, Meijer RI, Barrett EJ (2014). Insulin regulates brain function, but how does it get there? Diabetes 63: 3992–3997.
Grillo CA, Piroli GG, Lawrence RC, Wrighten SA, Green AJ, Wilson SP et al (2015). Hippocampal insulin resistance impairs spatial learning and synaptic plasticity. Diabetes (e-pub ahead of print 27 July 2015).
Groch S, Wilhelm I, Diekelmann S, Sayk F, Gais S, Born J (2011). Contribution of norepinephrine to emotional memory consolidation during sleep. Psychoneuroendocrinology 36: 1342–1350.
Grosmark AD, Mizuseki K, Pastalkova E, Diba K, Buzsaki G (2012). REM sleep reorganizes hippocampal excitability. Neuron 75: 1001–1007.
Hallschmid M, Benedict C, Schultes B, Fehm HL, Born J, Kern W (2004). Intranasal insulin reduces body fat in men but not in women. Diabetes 53: 3024–3029.
Hallschmid M, Wilhelm I, Michel C, Perras B, Born J (2011). A role for central nervous growth hormone-releasing hormone signaling in the consolidation of declarative memories. PLoS One 6: e23435.
Hardt O, Nader K, Nadel L (2013). Decay happens: the role of active forgetting in memory. Trends Cogn Sci 17: 111–120.
Hulme SR, Jones OD, Abraham WC (2013). Emerging roles of metaplasticity in behaviour and disease. Trends Neurosci 36: 353–362.
Ji D, Wilson MA (2007). Coordinated memory replay in the visual cortex and hippocampus during sleep. Nat Neurosci 10: 100–107.
Kern W, Halder R, al-Reda S, Spath-Schwalbe E, Fehm HL, Born J (1993). Systemic growth hormone does not affect human sleep. J Clin Endocrinol Metab 76: 1428–1432.
Kern W, Offenheuser S, Born J, Fehm HL (1996). Entrainment of ultradian oscillations in the secretion of insulin and glucagon to the nonrapid eye movement/rapid eye movement sleep rhythm in humans. J Clin Endocrinol Metab 81: 1541–1547.
Krug R, Benedict C, Born J, Hallschmid M (2010). Comparable sensitivity of postmenopausal and young women to the effects of intranasal insulin on food intake and working memory. J Clin Endocrinol Metab 95: E468–E472.
Lancel M (1999). Role of GABAA receptors in the regulation of sleep: initial sleep responses to peripherally administered modulators and agonists. Sleep 22: 33–42.
Liu L, Brown JC 3rd, Webster WW, Morrisett RA, Monaghan DT (1995). Insulin potentiates N-methyl-D-aspartate receptor activity in Xenopus oocytes and rat hippocampus. Neurosci Lett 192: 5–8.
Man HY, Lin JW, Ju WH, Ahmadian G, Liu L, Becker LE et al (2000). Regulation of AMPA receptor-mediated synaptic transmission by clathrin-dependent receptor internalization. Neuron 25: 649–662.
Molnar G, Farago N, Kocsis AK, Rozsa M, Lovas S, Boldog E et al (2014). GABAergic neurogliaform cells represent local sources of insulin in the cerebral cortex. J Neurosci 34: 1133–1137.
Moult PR, Harvey J (2008). Hormonal regulation of hippocampal dendritic morphology and synaptic plasticity. Cell Adh Migr 2: 269–275.
Osborne DM, Pearson-Leary J, McNay EC (2015). The neuroenergetics of stress hormones in the hippocampus and implications for memory. Front Neurosci 9: 164.
Oudiette D, Paller KA (2013). Upgrading the sleeping brain with targeted memory reactivation. Trends Cogn Sci 17: 142–149.
Plihal W, Born J (1999). Memory consolidation in human sleep depends on inhibition of glucocorticoid release. Neuroreport 10: 2741–2747.
Rasch B, Pommer J, Diekelmann S, Born J (2009). Pharmacological REM sleep suppression paradoxically improves rather than impairs skill memory. Nat Neurosci 12: 396–397.
Rechtschaffen A, Kales A (1968) A manual of standardized terminology, technique and scoring system for sleep stages of human sleep. Public Health Service, US Government Printing Office: Washington, DC.
Reger MA, Watson GS, Green PS, Baker LD, Cholerton B, Fishel MA et al (2008a). Intranasal insulin administration dose-dependently modulates verbal memory and plasma amyloid-beta in memory-impaired older adults. J Alzheimers Dis 13: 323–331.
Reger MA, Watson GS, Green PS, Wilkinson CW, Baker LD, Cholerton B et al (2008b). Intranasal insulin improves cognition and modulates beta-amyloid in early AD. Neurology 70: 440–448.
Sangiah S, Caldwell DF, Villeneuve MJ, Clancy JJ (1982). Sleep: sequential reduction of paradoxical (REM) and elevation of slow-wave (NREM) sleep by a non-convulsive dose of insulin in rats. Life Sci 31: 763–769.
Skeberdis VA, Lan J, Zheng X, Zukin RS, Bennett MV (2001). Insulin promotes rapid delivery of N-methyl-D- aspartate receptors to the cell surface by exocytosis. Proc Natl Acad Sci USA 98: 3561–3566.
Spetter MS, Hallschmid M (2015). Intranasal neuropeptide administration to target the human brain in health and disease. Mol Pharm 12: 2767–2780.
Tononi G, Cirelli C (2014). Sleep and the price of plasticity: from synaptic and cellular homeostasis to memory consolidation and integration. Neuron 81: 12–34.
Unger JW, Livingston JN, Moss AM (1991). Insulin receptors in the central nervous system: localization, signalling mechanisms and functional aspects. Prog Neurobiol 36: 343–362.
Van Cauter E, Plat L, Copinschi G (1998). Interrelations between sleep and the somatotropic axis. Sleep 21: 553–566.
Vitiello MV, Moe KE, Merriam GR, Mazzoni G, Buchner DH, Schwartz RS (2006). Growth hormone releasing hormone improves the cognition of healthy older adults. Neurobiol Aging 27: 318–323.
Wan Q, Xiong ZG, Man YH, Ackerley CA, Braunton J, Lu WY et al (1997). Recruitment of functional GABA(A) receptors to postsynaptic domains by insulin. Nature 388: 686–690.
Wilson MA, McNaughton BL (1994). Reactivation of hippocampal ensemble memories during sleep. Science 265: 676–679.
Yoo SS, Hu PT, Gujar N, Jolesz FA, Walker MP (2007). A deficit in the ability to form new human memories without sleep. Nat Neurosci 10: 385–392.
Acknowledgements
We thank Kirstin Nordhausen (Internal Medicine I, University of Lübeck, Lübeck, Germany) for her expert technical assistance and Martina Grohs (Department of Neuroendocrinology, University of Lübeck) for her invaluable laboratory work. Aero Pump, Hochheim, Germany, generously provided us with precision nasal air pumps.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supplementary Information accompanies the paper on the Neuropsychopharmacology website
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Feld, G., Wilhem, I., Benedict, C. et al. Central Nervous Insulin Signaling in Sleep-Associated Memory Formation and Neuroendocrine Regulation. Neuropsychopharmacol 41, 1540–1550 (2016). https://doi.org/10.1038/npp.2015.312
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2015.312
This article is cited by
-
Sleep-associated insulin resistance promotes neurodegeneration
Molecular Biology Reports (2023)
-
Protective effect of intranasal insulin on postoperative cognitive dysfunction in elderly patients with metabolic syndrome undergoing noncardiac surgery: a randomized clinical trial
Aging Clinical and Experimental Research (2023)
-
Intranasal administration of 40 and 80 units of insulin does not cause hypoglycemia during cardiac surgery: a randomized controlled trial
Canadian Journal of Anesthesia/Journal canadien d'anesthésie (2021)
-
Intranasal Insulin for Alzheimer’s Disease
CNS Drugs (2021)

{kind=link}
{kind=link}
{kind=link}