
Abstract
Serotonin reuptake inhibitors and cognitive-behavior therapy (CBT) are considered first-line treatments for obsessive-compulsive disorder (OCD). However, little is known about their modulatory effects on regional brain morphology in OCD patients. We sought to document structural brain abnormalities in treatment-naive OCD patients and to determine the effects of pharmacological and cognitive-behavioral treatments on regional brain volumes. Treatment-naive patients with OCD (n=38) underwent structural magnetic resonance imaging scan before and after a 12-week randomized clinical trial with either fluoxetine or group CBT. Matched-healthy controls (n=36) were also scanned at baseline. Voxel-based morphometry was used to compare regional gray matter (GM) volumes of regions of interest (ROIs) placed in the orbitofrontal, anterior cingulate and temporolimbic cortices, striatum, and thalamus. Treatment-naive OCD patients presented smaller GM volume in the left putamen, bilateral medial orbitofrontal, and left anterior cingulate cortices than did controls (p<0.05, corrected for multiple comparisons). After treatment with either fluoxetine or CBT (n=26), GM volume abnormalities in the left putamen were no longer detectable relative to controls. ROI-based within-group comparisons revealed that GM volume in the left putamen significantly increased (p<0.012) in fluoxetine-treated patients (n=13), whereas no significant GM volume changes were observed in CBT-treated patients (n=13). This study supports the involvement of orbitofronto/cingulo-striatal loops in the pathophysiology of OCD and suggests that fluoxetine and CBT may have distinct neurobiological mechanisms of action.
Similar content being viewed by others


INTRODUCTION
Obsessive-compulsive disorder (OCD) is a chronic disorder associated with clinically significant functional impairment (Vikas et al, 2009). Available treatments with serotonin reuptake inhibitors (SRIs) and cognitive-behavior therapy (CBT) are effective for most patients, but impairing residual symptoms and treatment non-response are common among this population (Eddy et al, 2004). Therefore, understanding brain-modulatory effects of these treatments is essential for further improvement of therapeutic alternatives.
Numerous magnetic resonance imaging (MRI) studies of OCD have demonstrated the presence of brain abnormalities involving cortico-subcortical circuits that interconnect the orbitofrontal cortex (OFC), anterior cingulate cortex (ACC), striatum, and thalamus, as well as temporolimbic regions (Atmaca et al, 2008; Busatto et al, 2000; Chamberlain et al, 2008; Harrison et al, 2009; Lacerda et al, 2003; Pujol et al, 2004; Radua and Mataix-Cols, 2009; Rauch et al, 1994; Saxena and Rauch, 2000; Szeszko et al, 1999; Valente et al, 2005; van den Heuvel et al, 2009). However, it is unknown whether such abnormalities may be reversed by specific treatments.
There are indications that SRIs modulate serotonin neurotransmission earlier in certain subcortical regions and later in the cerebral cortex (Blier and Bouchard, 1994; el Mansari et al, 1995). In the case of CBT, there is increasing evidence implicating the medial prefrontal cortex (medial OFC and rostral/subgenual subregions of the ACC) in the mediation of its therapeutic action (Sotres-Bayon et al, 2006; Milad et al, 2005). The medial prefrontal cortex is a key regulatory region in the maintenance inhibition of conditioned fear responses believed to underlie obsessive-compulsive symptoms and in the mediation of the extinction process of such fear responses (Milad et al, 2005, 2007; Phelps et al, 2004; Sotres-Bayon et al, 2006). Thus, although successful pharmacological interventions for OCD seem to exert a preferential subcortical-cortical ‘bottom-up’ regulation in the brain, CBT seems to elicit cortical-subcortical ‘top-down’ effects (Derryberry and Tucker, 1992; Goldapple et al, 2004; Tucker et al, 1995).
Although there are a growing number of short-term longitudinal functional neuroimaging studies documenting regional brain activity changes in OCD patients after SRI treatment or CBT (Baxter et al, 1992; Benkelfat et al, 1990; Perani et al, 1995; Saxena et al, 2002, 2009; Schwartz et al, 1996; Swedo et al, 1992), longitudinal MRI studies investigating treatment-related brain morphological changes are still scarce. The few available longitudinal MRI studies in this regard have been limited to the investigation of small groups of children with short illness duration, treated in an open, uncontrolled manner (Benazon et al, 2003; Gilbert et al, 2000; Lazaro et al, 2009; Rosenberg et al, 2000; Szeszko et al, 2004). Anecdotally, it has been suggested that SRIs are more likely than CBT to modulate brain volumes in OCD patients (Rosenberg et al, 2000). However, firmer conclusions are limited because of the lack of longitudinal MRI studies conducted in association with controlled, randomized clinical trials investigating the brain structural effects of these two modalities of intervention.
We attempted to address the above limitations by conducting a longitudinal voxel-based morphometry (VBM) study in treatment-naive adult OCD patients randomized to participate in either a clinical trial with fluoxetine or group CBT. Our aims were threefold: first, to document the profile of brain structural abnormalities associated with OCD without the confounding factor of previous treatment, we compared brain morphometric patterns between treatment-naive OCD patients and healthy controls; second, OCD patients were compared with controls again after treatment (either with fluoxetine or CBT) to examine whether brain volumes would change over the course of treatment; and third, we performed within-group comparisons (separately for fluoxetine- and CBT-treated subgroups) to disentangle possible independent effects of pharmacological and cognitive-behavioral treatment on regional brain morphology.
We focused our investigation within the principal brain regions previously implicated in imaging studies of OCD (OFC, ACC, striatum, thalamus, and temporolimbic structures) (Saxena and Rauch, 2000). A priori, we hypothesized that: (1) OCD patients would show significant gray matter (GM) volumetric abnormalities in those brain regions relative to controls; (2) after successful treatment, brain volume abnormalities would be attenuated, resulting in fewer significant differences relative to controls; (3) specifically, given the supposed effect of SRI treatment in modulating the activity of frontal-subcortical and limbic circuits (Bloom and Kupfer, 1995), patients in the fluoxetine group would exhibit more widespread brain effects after treatment; and (4) patients undergoing CBT would present GM volume changes mainly in regions of the medial prefrontal cortex (medial OFC and rostral/subgenual ACC), reflecting the primacy of cortico-subcortical top-down effects associated with extinction processes (Milad et al, 2005, 2007; Phelps et al, 2004).
MATERIALS AND METHODS
Subjects
This investigation is an arm of a research protocol that involved administering several neurobiological measures to treatment-naive OCD patients who participated in a larger clinical trial intended to investigate the effectiveness of fluoxetine and group CBT in a setting more similar to clinical practice (clinical registration information: http://clinicaltrials.gov—NCT00680602) (Belotto-Silva et al, 2011). This project was conducted in our outpatient OCD clinics at the University of São Paulo Medical School, Brazil (protocol, training, and reliability of instruments can be found elsewhere) (Hoexter et al, 2009; Miguel et al, 2008).
In brief, patients were referred from primary psychiatric services or were recruited through the local media (radio/television/newspapers/internet). Screening procedures included a telephone assessment, conducted by a trained psychologist. Once the subject met the initial requirements, a medical appointment was scheduled in which clinical and psychiatric assessments, structured clinical diagnostic interviews (SCID-I) (First et al, 1997), routine blood tests, and an electrocardiogram were obtained. Inclusion criteria comprised: (1) age between 18 and 65 years; (2) primary DSM-IV diagnosis of OCD; and (3) Yale–Brown Obsessive-Compulsive Scale (Y-BOCS) score ⩾16 or at least 10 if only obsessions or compulsions were present (only one patient had total Y-BOCS score <16, scoring 2 for obsessions and 13 for compulsions). Patients were excluded if they had: (1) previous exposure to any sort of psychotropic medication (benzodiazepines, antipsychotics, antidepressants, stimulants, mood stabilizers); (2) previous exposure to at least 12 sessions of CBT (only 2 patients had been exposed to CBT before); (3) history of head injury with loss of consciousness; (4) past/current substance abuse or dependence; (5) lifetime history of psychosis; (6) suicide risk; (7) any organic disorders that could affect the central nervous system; (8) contraindications for MRI scanning; and (9) being pregnant.
Controls were selected among college students and hospital and university staff, or were recruited through word of mouth. They were selected according to the same criteria described above (except for the presence of OCD) and had no current history of neurological or psychiatric disorders on the basis of SCID interviews. All participants provided written informed consent, which had been approved by the local Institutional Review Board.
From 623 patients referred to our OCD clinic from 2006 to 2008 (Hoexter et al, 2009), 254 were excluded in the telephone screening and 328 were excluded in the psychiatric medical assessment mainly for not being treatment naive (Supplementary Figure S1). In all, 41 OCD patients participated. Similarly, 54 potential healthy controls were screened, from which 38 who fulfilled all the criteria for study entry were selected. It is noteworthy that three patients and two controls were excluded (Figure 1). Therefore, 38 treatment-naive OCD patients and 36 controls who matched for age, gender, socioeconomic status, level of education, and handedness were studied (Table 1).

Study flowchart showing the numbers of participants through each stage of the study.
Clinical Assessments
The Y-BOCS (Goodman et al, 1989), Dimensional Yale–Brown Obsessive-Compulsive Scale (DY-BOCS) (Rosario-Campos et al, 2006), Beck Depression Inventory (BDI) (Beck et al, 1961), Beck Anxiety Inventory (BAI) (Beck et al, 1988), and Clinical Global Impression scale (CGI) (Guy, 1976) were administered before and after 12 weeks of treatment (Hoexter et al, 2009) by interviewers who were blind to the type of treatment.
On the basis of the SCID, 13 OCD patients met DSM-IV criteria for current major depression and 10 additional patients had a history of major depression and/or dysthymia. Other SCID-I DSM-IV lifetime diagnoses included agoraphobia (n=2), panic disorder with agoraphobia (n=1), panic disorder without agoraphobia (n=3), specific phobia (n=13), social phobia (n=21), post-traumatic stress disorder (n=8), generalized anxiety disorder (n=17), bipolar I (n=1), bipolar II disorder (n=2), somatization (n=2), hypochondriasis (n=1), body dysmorphic disorder (n=5), anorexia nervosa (n=3), bulimia nervosa (n=2), binge-eating disorder (n=2), skin picking (n=8), trichotillomania (n=2), intermittent explosive disorder (n=7), attention-deficit/hyperactivity disorder (n=3), chronic tics (n=4), and Tourette's syndrome (n=2).
Allocation
A specific mode of randomization was used in this study (Fossaluza et al, 2009). In brief, a computer program was developed to sequentially allocate patients to each treatment group, in which prognostic factors such as gender, age, and initial Y-BOCS score were inserted in the model. The aim of this method was to minimize differences between groups by balancing possible confounders. Consequently, patients allocated to either group (fluoxetine=19 and CBT=19) were less likely to differ significantly in terms of major clinical and demographical characteristics (Supplementary Table S1).
Fluoxetine Treatment
Patients received fluoxetine (up to 80 mg/day) for 12 weeks, starting at 20 mg/day in the first week, with weekly increases of 20 mg/day (Diniz et al, 2010). Medical appointments were scheduled every 4 weeks to monitor side effects and treatment compliance. Of the 14 patients who completed the treatment (74% of the initial sample), all reached the maximal dose of 80 mg/day without reporting major side effects, except for one subject who could not tolerate doses higher than 20 mg/day because of gastrointestinal effects and tremor. In all, 13 post-fluoxetine MRI scans were analyzed. Reasons for not analyzing a second MRI scan and reasons for dropouts are presented in Figure 1. Non-completers were not statistically different from completers in terms of age, age at onset of symptoms, illness duration, Y-BOCS, DY-BOCS, BDI, and BAI scores.
Group CBT Treatment
Patients were divided into subgroups of 6–8 people each and attended a weekly 2-h standardized CBT session for 12 weeks. The groups were coordinated by a psychologist with several years of experience in behavior therapy, who was trained by the author of the group CBT protocol (Cordioli et al, 2002; Volpato Cordioli et al, 2003). Patients who missed more than two consecutive sessions were considered dropouts. The protocol consisted of (Volpato Cordioli et al, 2003): session 1—psychoeducational information; session 2—development of symptoms hierarchies; session 3—introduction to exposure with response prevention—E/RP; sessions 4–7—E/RP exercises and cognitive techniques; session 8—family session, and sessions 9–12—review of E/RP and cognitive techniques. In all, 15 patients (79% of the initial sample) completed the group CBT treatment, and 13 post-CBT MRI scans were analyzed. Reasons for not analyzing a second MRI scan and reasons for dropouts are presented in Figure 1. The non-completers were not statistically different from completers in terms of age, age at onset of symptoms, illness duration, Y-BOCS, DY-BOCS, BDI, and BAI scores.
Image Acquisition and Processing
Patients were scanned at baseline and after 12 weeks of treatment. Healthy controls were scanned just once at baseline, given that there is evidence that such a small period of time does not significantly affect GM measures in healthy subjects as assessed with VBM (Hölzel et al, 2011; Lyoo et al, 2010; Lazaro et al, 2009). Images were acquired using a 1.5-T GE Signa scanner (General Electric, Milwaukee, WI, USA). Contiguous 1.6-mm axial images across the entire brain were obtained (T1-3D SPGR sequence, TE=4.20 ms, TR=10.5 ms, flip angle=15, acquisition matrix=256 × 192) and interpolated using ZIP2 to a final voxel size of 0.94 × 0.94 × 0.80 mm3 (248 slices). VBM processing was executed using the Statistical Parametric Mapping (SPM5) package (Wellcome Department of Imaging Neuroscience, London, UK), performed in Matlab (Mathworks, Sherborn, MA), using the default parameters implemented in the VBM5 Toolbox (http://dbm.neuro.uni-jena.de/vbm/). This protocol uses the unified segmentation approach (Ashburner and Friston, 2005), which integrates the processes of tissue classification, MRI inhomogeneity bias correction, and spatial normalization to the standard SPM T1-MRI template, based on 152 healthy subjects from the Montreal Neurological Institute (MNI) (Mazziotta et al, 1995), using linear (12-parameter affine) and non-linear transformations. The extension of Hidden Markov Random Field approach available in the VBM5 tool box was used, aimed at increasing the quality of image segmentation (Cuadra et al, 2005). Subsequently, the final tissue maps of GM, white matter, and brain-spinal fluid were modulated by the Jacobian determinants derived from spatial normalization to the MNI standard space. This enabled brain structures that had their volumes reduced after spatial normalization to have their total counts restored by an amount proportional to the degree of volume shrinkage and thus allowed testing for regional differences in the absolute volume amount of GM (Good et al, 2001). Voxel sizes of segmented and spatially normalized images equaled 1 × 1 × 1 mm3. Finally, images from OCD patients and controls were smoothed using a 12-mm Gaussian kernel.
Statistical Analysis
Comparisons of GM volume were performed between and within groups with VBM using the general linear model (Friston et al, 1994). Only voxels with values above an absolute threshold of p=0.05 for differentiating GM from other tissues entered the analyses. A measure of the total amount of GM was entered as confound in an analysis of covariance. In each comparison, two t-statistic maps, corresponding to opposite contrasts (volume decrease and increase), were generated and displayed into standard space at a threshold of p<0.001, uncorrected. Each statistical map was then inspected for the presence of clusters of significant differences in regions where volumetric abnormalities had been predicted a priori (orbitofrontal, anterior cingulate and temporolimbic cortices, thalamus, and caudate–putamen) using the small volume correction (SVC) method included in SPM toolbox, with the purpose of constraining the total number of voxels included in the analyses. Each region was circumscribed by merging the spatially normalized region-of-interest (ROI) masks that are available within the Anatomical Automatic Labeling SPM toolbox. Anatomical masks were used separately in each hemisphere (left and right, respectively), resulting in search volumes of 7704 and 7976 voxels for the superior lateral OFC; 7104 and 8120 voxels for the middle lateral OFC; 13 520 and 13 631 voxels for the inferior lateral OFC; 5752 and 6848 voxels for the medial OFC; 7696 and 7952 voxels for the caudate nucleus; 8039 and 8438 voxels for the putamen; 8435 and 8174 voxels for the thalamus; 11 200 and 10 504 voxels for the anterior cingulate gyrus; 1760 and 1984 voxels for the amygdala; 7456 and 7568 voxels for the hippocampus; and 7824 and 9056 voxels for the parahippocampal gyrus. Findings of these hypothesis-driven, SVC-based analyses were reported as significant if surviving family-wise error (FWE) correction for multiple comparisons (p<0.05) over the respective ROI, with voxel clusters comprising at least 20 voxels. For unpredicted findings in other GM regions, we used the FWE-corrected p<0.05 level over the whole brain. In all analyses, we converted MNI coordinates of voxels of maximal statistical significance to the Talairach and Tournoux (1988) system (Brett et al, 2002).
RESULTS
Treatment Outcome
After treatment, OCD patients as a whole exhibited a significant decrease in the severity of obsessive-compulsive symptoms (mean±SD pre- vs post-treatment Y-BOCS: 24.9±5.2 vs 16.3±8.1; decrements of 34.5%; p=0.001) and depressive symptoms (pre- vs post-treatment BDI: 14.9±8.0 vs 9.8±7.6; decrements of 34.2%; p=0.007). Within-group comparisons (fluoxetine-treated=13 and CBT-treated=13) revealed significant OCD severity reductions for both treatments subgroups (pre- vs post-treatment Y-BOCS: 23.4±5.0 vs 14.8±6.3; decrements of 36.7%; p=0.005 for fluoxetine and 26.5±5.1 vs 17.7±9.6; decrements of 33%; p=0.003 for CBT), with no statistical difference between treatments. In all, 5 out of 13 fluoxetine-treated patients (38.4%) and 6 out of 13 CBT-treated patients (46.1%) were considered full responders (defined as a minimum reduction of 35% on the Y-BOCS and a ‘much-improved’ or ‘very-much-improved’ CGI-improvement scores for OCD).
Subjects also experienced a decrease in depressive symptoms in both treatment subgroups, but this difference was only statistically significant for CBT (pre- vs post-treatment BDI: 14.7±9.2 vs 9.1±9.0; decrements of 38.1%; p=0.018 for CBT and 15.0±7.1 vs 10.5±6.4; decrements of 30%; p=0.1 for fluoxetine).
MRI Comparisons: Treatment-Naive OCD Patients at Baseline vs Controls
The total GM volume measured in milliliters in the segmented images was 915.12±61.34 in the OCD group and 932.51±39.26 in healthy control subjects (t=−1.443, df=72, p=0.153).
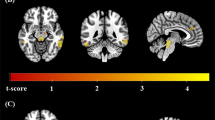
VBM analyses indicated that there was a significantly smaller GM volume in the left putamen (dorsal rostral portions) in OCD patients than in controls (Table 2 and Figure 2a). A similar pattern of between-group differences involving the putamen was seen after exclusion of patients who met criteria for current major depression (n=13) (Table 2). In addition, this subgroup of non-depressed OCD patients also presented clusters of significant smaller GM volume in the left (Table 2, Figure 2b) and right medial OFC (Table 2, Figure 2c) and right ACC (Table 2, Figure 2c).

Brain regions where there were foci of significantly gray matter volume differences in obsessive-compulsive disorder (OCD) patients relative to healthy control subjects. (a) Lesser regional gray matter volume in OCD patients (n=38) vs healthy controls (n=36) in the left putamen. (b) Lesser regional gray matter volume in OCD patients without major depression (n=25) vs healthy controls (n=36) in the left medial orbitofrontal cortex. (c) Lesser regional gray matter volume in OCD patients without major depression (n=25) vs healthy controls (n=36) encompassing the right anterior cingulate and medial orbitofrontal cortices.
No clusters of significant greater GM volumes were found within the principal brain areas predicted a priori in the OCD sample. There were also no clusters of regional changes of greater or smaller GM volumes in other unpredicted brain regions considering a p-value <0.05, corrected for multiple comparisons over the whole brain. For exploratory purposes, given that other regions appear to be involved in OCD, such as the dorsolateral prefrontal, posterior cingulate, and parietal cortices (Menzies et al, 2008; Busatto et al, 2000), data of unpredicted GM volumes using a less stringent threshold of p<0.001 for the whole brain (uncorrected for multiple comparisons) are listed in Supplementary Table S2.
In the OCD group, there were no significant linear correlations between GM volumes involving the regions shown to be altered in the between-group comparisons and either of the variables: age at onset of symptoms, illness duration, Y-BOCS, DY-BOCS, BDI, and BAI scores. The threshold for considering a correlation as statistically significant was set at a p-value <0.001, uncorrected for multiple comparisons over the entire brain, after covarying out the effect of the total amount of GM.
We also performed an analysis comparing pre-treatment GM volumes specifically in the OCD subgroup who subsequently completed either the fluoxetine or CBT treatment protocols (n=26) against the control group (n=36). This analysis confirmed the findings of significant smaller GM volume in the left putamen in OCD patients relative to controls (219 voxels; peak coordinates=−27, 13, 2; Z=3.59; peak voxel p-FWE=0.016) (1350 voxels; peak coordinates=−27, 13, 2; Z=3.77; peak voxel p-FWE=0.009). No GM alterations involving regions within the medial orbitofrontal and anterior cingulate cortices were observed.
MRI Comparisons: Treated OCD Patients vs Controls
The analyses comparing post-treatment GM volumes in OCD patients who completed the treatment protocols (n=26) against the control group indicated that there were no longer significant findings of smaller GM volume in the left putamen in OCD subjects relative to controls, as it had been found in the pre-treatment comparisons between OCD patients and controls. There were no other clusters of significant GM volume differences between treated OCD patients and controls, either in the other areas where volume abnormalities had been hypothesized a priori or in unpredicted brain regions.
Pre- vs Post-Treatment MRI Comparisons within the OCD Group
To test our hypothesis that fluoxetine and CBT exert different modulations over the volume of brain regions relevant to the pathophysiology of OCD, we conducted voxelwise within-group analysis comparing GM volumes pre vs post treatment in the two OCD subgroups (pre vs post fluoxetine=13, pre vs post CBT=13). None of these analyses revealed significant changes in GM volumes after treatment, either with a threshold of p<0.001 or a less stringent threshold of p<0.01, uncorrected for multiple comparisons, nor in other, unpredicted brain regions. Finally, for exploratory purposes, we extracted mean GM volume values from the spatially normalized images of each patient before and after treatment, using bilateral ROI masks placed on the putamen, medial OFC, and ACC. These within-group ROI comparisons showed, in fluoxetine-treated OCD patients (n=13), a significant increase in GM volume in the left putamen (p=0.012) after treatment. Conversely, there were no statistically significant GM volume changes after treatment in any of the ROIs in OCD patients who underwent the CBT program (n=13) (Table 3). It is noteworthy that these results were not influenced by differences in the percentage of changes in comorbid depressive symptoms.
DISCUSSION
This study investigated post-treatment morphometric brain alterations in adult treatment-naive OCD patients participating in a randomized clinical trial comparing pharmacotherapy and psychotherapy. A methodological advantage of enrolling treatment-naive patients in such a study design is the exclusion of potentially confounding effects of previous treatments on GM brain volumes. The VBM analysis revealed, in treatment-naive OCD patients, decreased GM volume in the left putamen compared with controls. In a subgroup of OCD patients without comorbid depression, reduced GM volumes in the bilateral medial orbitofrontal and left anterior cingulate cortices were also observed, reinforcing the involvement of these structures in the pathophysiology of OCD. After successful treatment with either SRIs or CBT, GM volume abnormalities in the left putamen presented in the whole sample of OCD patients were no longer detectable relative to controls. ROI-based within-group comparisons revealed that GM volume in the left putamen significantly increased in fluoxetine-treated patients, whereas no significant GM volume changes were observed in CBT-treated patients.
Fluoxetine and Group CBT Treatment Outcomes
Weekly group CBT has been shown to be as effective as fluoxetine treatment in reducing obsessive-compulsive symptoms. This study adds to evidence from earlier papers that weekly group CBT is as effective as selective SRIs in treating OCD (Sousa et al, 2006). It is important to highlight that the group approach lowers costs considerably, hence making CBT accessible to a larger numbers of patients.
Baseline Brain Volume Abnormalities in Treatment-Naive OCD Patients vs Controls
Neuroimaging studies have implicated a dysfunction of frontostriatal regions in the pathophysiology of OCD (Insel, 1992; Rauch, 2000; Saxena et al, 2000). Although the direction of regional GM volumetric abnormalities reported in the literature has not always been consistent across morphometric MRI studies, our results converge with the findings from two recent VBM meta-analysis that demonstrated GM alterations in OCD patients encompassing territories within the striatum, orbitofrontal, and anterior cingulate cortices (Radua et al, 2009; Rotge et al, 2010). It is noteworthy that although our results showed putaminal decrements in OCD, Radua and Mataix-Cols (2009) and Rotge et al (2010) demonstrated increased GM within this region. Another recent VBM meta-analysis demonstrated that OCD was associated with greater putaminal volume, whereas the opposite was observed in other anxiety disorders (such as posttraumatic stress disorder and panic disorder) (Radua et al, 2010). Inconsistencies in the direction of these abnormalities may be partially interpreted as a consequence of methodological differences across separate MRI studies, such as small and heterogeneous samples of OCD participants, matching criteria, voxelwise statistical testing, and image processing details (Ferreira and Busatto, 2010; Menzies et al, 2008). In this study, aiming to investigate a real-world OCD population, we did not exclude many comorbidities including several anxiety disorders, which may have added variability to our findings. Moreover, an alternative explanation for such a disparity is the fact that we investigated treatment-naive adult OCD patients. This may be an important difference, given that the majority of studies included in these meta-analyses investigated OCD patients who were currently taking or had already taken medication. The few studies that investigated treatment-naive patients were performed in children with a short illness duration. Therefore, our results may suggest that previous exposure to medication, regardless of whether OCD patients were medicated or non-medicated at the time of MRI scanning, may also have an important role in the variability of results. It is equally important to highlight, given that OCD and major depressive disorder are mediated by distinct but partially overlapping neural systems (Cardoner et al, 2007; Saxena et al, 2001), that our baseline findings of altered GM volumes were present in the OCD sample independently of the presence of current major depression.
In particular, the dorsal subregion of the rostral putamen implicated in this study receives projections from the dorsolateral prefrontal cortex (critical to higher cognitive processes), as well as premotor and motor areas (involved in motor planning and execution) (Haber, 2003). Thus, alterations in this striatal subregion could be related to cognitive and motor impairments that are highly frequently reported in OCD patients (Chamberlain et al, 2005; Menzies et al, 2008), such as mental inflexibility and impaired motor inhibition.
Our finding of smaller GM volume in the medial OFC and ACC is consistent with previous results reported in imaging studies of OCD (Pujol et al, 2004; Rauch et al, 1994; Valente et al, 2005, Radua et al, 2009; Rotge et al, 2010). Given their connections with the ventral striatum, amygdala and insula, the medial OFC, and ACC are important regulatory nodes monitoring motivation and emotional responses (Cardinal et al, 2002; Phillips et al, 2003). Recently, functional imaging studies have provided evidence that cortical connectivity of different subregions within the striatum, involving both cognitive and emotional processing, is disrupted in OCD (Harrison et al, 2009). Therefore, our findings of GM abnormalities in specific subregions of the striatum (putamen), OFC, and ACC provide structural substrate for functional connectivity alterations observed in OCD. The exact neurobiological mechanisms underlying how morphometric changes of specific brain regions may influence actual physiological activity of the putative cortico-striatal loops are not fully understood. It may be speculated that alterations in GM volumes could be due to changes in the number of neurons, glial cells, or synaptic arborization that could ultimately inhibit or facilitate cortico-striatal communication. It is remarkable that surgical treatments for treatment-refractory OCD, such as stereotactic ablation and deep brain stimulation that intent to modulate specific cortico-striatal circuits (Greenberg et al, 2010), target regions closely located to our putaminal finding.
MRI Findings in OCD Patients after Treatment with Fluoxetine or CBT
The results of our post-treatment comparison between OCD patients and healthy controls suggest that GM volume abnormalities in the left putamen were attenuated after treatment. These findings may indicate that OCD treatment, regardless of the modality used modulates GM volumes in OCD patients. If it is the case, this interpretation is consistent with several functional imaging studies that have reported metabolic normalization after either pharmacotherapy or behavior therapy for OCD (Baxter et al, 1992; Perani et al, 1995; Saxena et al, 2002; Swedo et al, 1992).
However, the above interpretation has to be made cautiously, as there are other plausible explanations for these results. Loss of significant GM differences between post-treated patients and controls does not necessarily prove major changes in regional GM volume in OCD subjects, but may reflect minor effects or even increased experimental noise at follow-up.
One second alternative interpretation is that modulation of brain volume abnormalities would be the result of only one of the two specific treatments, either SRI or CBT, rather than reflecting overall effects of clinical improvement per se. Indeed, although the voxelwise within-group comparisons of pre- vs post-treatment MRI data did not show significant volumetric brain changes after treatment in OCD patients, our exploratory ROI analysis demonstrated a significant left putaminal volume increase after fluoxetine treatment, whereas no volume changes after CBT were observed in any of the brain regions investigated. Interestingly, a longitudinal VBM study reported volume increments in the striatum of OCD children after exposure to selective SRIs (Lazaro et al, 2009). It is noteworthy that this finding was obtained only when a less stringent threshold was used. It is possible that GM modifications after treatment were not detectable by VBM because of a limitation of this approach in investigating subtle changes spread throughout large portions of specific GM nuclei (Szeszko et al, 2008). In this sense, ROI approaches may be more suitable for detecting subtle GM changes that take place over an entire anatomical brain structure, in contrast to VBM, which requires a more robust GM volume change localized in particular discrete areas. It has been suggested in previous longitudinal morphometric neuroimaging investigations that neurobiological changes after treatment may be specific to SRIs rather than to CBT (Benazon et al, 2003; Gilbert et al, 2000; Lazaro et al, 2009; Rosenberg et al, 2000; Szeszko et al, 2004). In this regard, given that the majority of longitudinal volumetric studies were performed in children with short illness duration, our findings complement previous data by demonstrating similar results in chronic adult patients. We speculate that different neural pathways and neurotransmitters are associated with each type of intervention. It has been demonstrated that modulations in serotonergic neurotransmission by SRIs mediate neuroplasticity (neurogenesis and gliogenesis) in various cortical and subcortical structures involved in OCD (Czeh et al, 2007; Kodama et al, 2004; Soumier et al, 2009). On the other hand, given the role of the medial prefrontal cortex in the modulation of extinction memory of conditioned fear response (Milad et al, 2005, 2007; Phelps et al, 2004), it is postulated that the brain sites of action of CBT primarily encompass regions within the medial OFC and rostral/subgenual ACC. In recent years, there has been increasing interest in the glutamatergic system in OCD (MacMaster et al, 2008) and its role in extinction learning (Davis and Myers, 2002). Previous studies have shown that glutamatergic manipulation within the medial prefrontal cortex enhances synaptic plasticity and facilitates consolidation of extinction (Burgos-Robles et al, 2007).
Finally, although we did document medial OFC and ACC volume abnormalities in OCD patients, there were no GM volume changes after treatment in any regions of the frontal cortex in either the fluoxetine or CBT OCD subgroups. Speculatively, given that SRIs are considered to modulate serotonin transmission earlier in subcortical regions and later in cortical ones (Blier and Bouchard, 1994; el Mansari et al, 1995) and that treatment effects with SRIs and CBT can be delayed beyond 12 weeks (Greist et al, 1995), volumetric changes in frontal cortical territories may require longer periods to take place. Moreover, given the impossibility of patients to choose the type of treatment, the lack of a within-group CBT effect on MRI volumes could have been due to variability in the engagement to perform that intervention.
Methodological Considerations and Conclusions
The results reported herein must be interpreted with caution because of several limitations. First, the small sample size, mainly in the follow-up arm of the study, may have limited our power to detect differences in other brain regions. Second, the CBT approach was applied in a group setting, which may be different than providing one-to-one treatment. Third, given that we adopted broad inclusion criteria to build a setting closer to clinical practice, our OCD patients presented many comorbidities which may have added variability to our findings. Fourth, our randomized clinical trial did not include a placebo-treated group. Fifth, we did not perform a second MRI scan in controls. Sixth, GM volume within-group differences were only observed in the ROI analyses, whereas no within-group differences were detected in the VBM approach. This limits the robustness of the post hoc tests. Therefore, our findings that fluoxetine and CBT may have different treatment effects on the brain should be interpreted as exploratory and deserve replication before generalization.
In conclusion, our results of smaller GM volume in the putamen, medial OFC, and ACC of treatment-naive OCD patients highlight the involvement of orbitofrontal/cingulo-striatal loops in the pathophysiology of OCD. ROI exploratory analyses suggest that fluoxetine and CBT may have distinct neurobiological mechanisms of action. Further MRI studies are warranted using placebo-controlled designs in larger samples of OCD patients, with longer follow-up periods to allow investigation as to whether GM changes reported herein may be replicated and extended to other brain regions after different treatment interventions.
References
Ashburner J, Friston KJ (2005). Unified segmentation. Neuroimage 26: 839–851.
Atmaca M, Yildirim H, Ozdemir H, Ozler S, Kara B, Ozler Z et al (2008). Hippocampus and amygdalar volumes in patients with refractory obsessive-compulsive disorder. Prog Neuropsychopharmacol Biol Psychiatry 32: 1283–1286.
Baxter Jr LR, Schwartz JM, Bergman KS, Szuba MP, Guze BH, Mazziotta JC et al (1992). Caudate glucose metabolic rate changes with both drug and behavior therapy for obsessive-compulsive disorder. Arch Gen Psychiatry 49: 681–689.
Beck AT, Epstein N, Brown G, Steer RA (1988). An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 56: 893–897.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961). An inventory for measuring depression. Arch Gen Psychiatry 4: 561–571.
Belotto-Silva C, Diniz JB, Malavazzia DM, Valério C, Fossaluza V, Sonia Borcato S et al (2011). Group cognitive-behavioral therapy versus selective serotonin reuptake inhibitors for obsessive-compulsive disorder: a practical clinical trial. J Anxiety Disord (in press).
Benazon NR, Moore GJ, Rosenberg DR (2003). Neurochemical analyses in pediatric obsessive-compulsive disorder in patients treated with cognitive-behavioral therapy. J Am Acad Child Adolesc Psychiatry 42: 1279–1285.
Benkelfat C, Nordahl TE, Semple WE, King AC, Murphy DL, Cohen RM (1990). Local cerebral glucose metabolic rates in obsessive-compulsive disorder. Patients treated with clomipramine. Arch Gen Psychiatry 47: 840–848.
Blier P, Bouchard C (1994). Modulation of 5-HT release in the guinea-pig brain following long-term administration of antidepressant drugs. Br J Pharmacol 113: 485–495.
Bloom FE, Kupfer DJ (1995). Psychopharmacology: The Fourth Generation of Progress. Raven Press: New York. 2002p.pp.
Brett M, Johnsrude IS, Owen AM (2002). The problem of functional localization in the human brain. Nat Rev Neurosci 3: 243–249.
Burgos-Robles A, Vidal-Gonzalez I, Santini E, Quirk GJ (2007). Consolidation of fear extinction requires NMDA receptor-dependent bursting in the ventromedial prefrontal cortex. Neuron 53: 871–880.
Busatto GF, Zamignani DR, Buchpiguel CA, Garrido GE, Glabus MF, Rocha ET et al (2000). A voxel-based investigation of regional cerebral blood flow abnormalities in obsessive-compulsive disorder using single photon emission computed tomography (SPECT). Psychiatry Res 99: 15–27.
Cardinal RN, Parkinson JA, Hall J, Everitt BJ (2002). Emotion and motivation: the role of the amygdala, ventral striatum, and prefrontal cortex. Neurosci Biobehav Rev 26: 321–352.
Cardoner N, Soriano-Mas C, Pujol J, Alonso P, Harrison BJ, Deus J et al (2007). Brain structural correlates of depressive comorbidity in obsessive-compulsive disorder. Neuroimage 38: 413–421.
Chamberlain SR, Blackwell AD, Fineberg NA, Robbins TW, Sahakian BJ (2005). The neuropsychology of obsessive compulsive disorder: the importance of failures in cognitive and behavioural inhibition as candidate endophenotypic markers. Neurosci Biobehav Rev 29: 399–419.
Chamberlain SR, Menzies L, Hampshire A, Suckling J, Fineberg NA, del Campo N et al (2008). Orbitofrontal dysfunction in patients with obsessive-compulsive disorder and their unaffected relatives. Science 321: 421–422.
Cordioli A, Heldt E, Bochi D, Margis M, de Sousa M, Tonello J et al (2002). Cognitive-behavioral group therapy in the treatment of obsessive-compulsive disorder: an open clinical trial. Revista Brasileira de Psiquiatria 24: 113–120.
Cuadra MB, Cammoun L, Butz T, Cuisenaire O, Thiran JP (2005). Comparison and validation of tissue modelization and statistical classification methods in T1-weighted MR brain images. IEEE Trans Med Imaging 24: 1548–1565.
Czeh B, Muller-Keuker JI, Rygula R, Abumaria N, Hiemke C, Domenici E et al (2007). Chronic social stress inhibits cell proliferation in the adult medial prefrontal cortex: hemispheric asymmetry and reversal by fluoxetine treatment. Neuropsychopharmacology 32: 1490–1503.
Davis M, Myers KM (2002). The role of glutamate and gamma-aminobutyric acid in fear extinction: clinical implications for exposure therapy. Biol Psychiatry 52: 998–1007.
Derryberry D, Tucker DM (1992). Neural mechanisms of emotion. J Consult Clin Psychol 60: 329–338.
Diniz JB, Shavitt RG, Pereira CA, Hounie AG, Pimentel I, Koran LM et al (2010). Quetiapine versus clomipramine in the augmentation of selective serotonin reuptake inhibitors for the treatment of obsessive-compulsive disorder: a randomized, open-label trial. J Psychopharmacol 24: 297–307.
Eddy KT, Dutra L, Bradley R, Westen D (2004). A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder. Clin Psychol Rev 24: 1011–1030.
el Mansari M, Bouchard C, Blier P (1995). Alteration of serotonin release in the guinea pig orbito-frontal cortex by selective serotonin reuptake inhibitors. Relevance to treatment of obsessive-compulsive disorder. Neuropsychopharmacology 13: 117–127.
Ferreira LK, Busatto GF (2010). Heterogeneity of coordinate-based meta-analyses of neuroimaging data: an example from studies in OCD. Br J Psychiatry 197: 76–77; author reply 77.
Fossaluza V, Diniz JB, Pereira Bde B, Miguel EC, Pereira CA (2009). Sequential allocation to balance prognostic factors in a psychiatric clinical trial. Clinics (Sao Paulo) 64: 511–518.
Friston K, Holmes A, Worsley K, Poline J, Frith C, Frackowiak R (1994). Statistic parametric maps in functional imaging: a general linear approach. Hum Brain Mapp 2: 189–210.
Gilbert AR, Moore GJ, Keshavan MS, Paulson LA, Narula V, Mac Master FP et al (2000). Decrease in thalamic volumes of pediatric patients with obsessive-compulsive disorder who are taking paroxetine. Arch Gen Psychiatry 57: 449–456.
Goldapple K, Segal Z, Garson C, Lau M, Bieling P, Kennedy S et al (2004). Modulation of cortical-limbic pathways in major depression: treatment-specific effects of cognitive behavior therapy. Arch Gen Psychiatry 61: 34–41.
Good CD, Johnsrude IS, Ashburner J, Henson RN, Friston KJ, Frackowiak RS (2001). A voxel-based morphometric study of ageing in 465 normal adult human brains. Neuroimage 14 (1 Pt 1): 21–36.
Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL et al (1989). The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch Gen Psychiatry 46: 1006–1011.
Greenberg BD, Rauch SL, Haber SN (2010). Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for OCD. Neuropsychopharmacology 35: 317–336.
Greist JH, Jefferson JW, Kobak KA, Katzelnick DJ, Serlin RC (1995). Efficacy and tolerability of serotonin transport inhibitors in obsessive-compulsive disorder. A meta-analysis. Arch Gen Psychiatry 52: 53–60.
Guy W (1976). Clinical Global Impression (CGI). In: ECDEU Assessment Manual for Psychopharmacology, Revised edn. US Department of Health, Education, and Welfare: Rockville, MD, USA [S.l].
Haber SN (2003). The primate basal ganglia: parallel and integrative networks. J Chem Neuroanat 26: 317–330.
Harrison BJ, Soriano-Mas C, Pujol J, Ortiz H, Lopez-Sola M, Hernandez-Ribas R et al (2009). Altered corticostriatal functional connectivity in obsessive-compulsive disorder. Arch Gen Psychiatry 66: 1189–1200.
Hoexter MQ, Shavitt RG, D’Alcante CC, Cecconi JP, Diniz JB, Belotto-Silva C et al (2009). The drug-naive OCD patients imaging genetics, cognitive and treatment response study: methods and sample description. Rev Bras Psiquiatr 31: 349–353.
Hölzel BK, Carmody J, Vangel M, Congleton C, Yerramsetti SM, Gard T et al (2011). Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Res 191: 36–43.
Insel TR (1992). Toward a neuroanatomy of obsessive-compulsive disorder. Arch Gen Psychiatry 49: 739–744.
Kodama M, Fujioka T, Duman RS (2004). Chronic olanzapine or fluoxetine administration increases cell proliferation in hippocampus and prefrontal cortex of adult rat. Biol Psychiatry 56: 570–580.
Lacerda AL, Dalgalarrondo P, Caetano D, Camargo EE, Etchebehere EC, Soares JC (2003). Elevated thalamic and prefrontal regional cerebral blood flow in obsessive-compulsive disorder: a SPECT study. Psychiatry Res 123: 125–134.
Lazaro L, Bargallo N, Castro-Fornieles J, Falcon C, Andres S, Calvo R et al (2009). Brain changes in children and adolescents with obsessive-compulsive disorder before and after treatment: a voxel-based morphometric MRI study. Psychiatry Res 172: 140–146.
Lyoo IK, Dager SR, Kim JE, Yoon SJ, Friedman SD, Dunner DL et al (2010). Lithium-induced gray matter volume increase as a neural correlate of treatment response in bipolar disorder: a longitudinal brain imaging study. Neuropsychopharmacology 35: 1743–1750.
MacMaster FP, O’Neill J, Rosenberg DR (2008). Brain imaging in pediatric obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry 47: 1262–1272.
Mazziotta JC, Toga AW, Evans A, Fox P, Lancaster J (1995). A probabilistic atlas of the human brain: theory and rationale for its development. The International Consortium for Brain Mapping (ICBM). Neuroimage 2: 89–101.
First MB, Spitzer RL, Gibbon M, Williams JB (1997). Structured Clinical Interview for DSM-IV Axis I Disorders: Clinical Version (SCID CV). American Psychiatric Press: Washington, DC.
Menzies L, Chamberlain SR, Laird AR, Thelen SM, Sahakian BJ, Bullmore ET (2008). Integrating evidence from neuroimaging and neuropsychological studies of obsessive-compulsive disorder: the orbitofronto-striatal model revisited. Neurosci Biobehav Rev 32: 525–549.
Miguel EC, Ferrao YA, Rosario MC, Mathis MA, Torres AR, Fontenelle LF et al (2008). The Brazilian research consortium on obsessive-compulsive spectrum disorders: recruitment, assessment instruments, methods for the development of multicenter collaborative studies and preliminary results. Rev Bras Psiquiatr 30: 185–196.
Milad MR, Quinn BT, Pitman RK, Orr SP, Fischl B, Rauch SL (2005). Thickness of ventromedial prefrontal cortex in humans is correlated with extinction memory. Proc Natl Acad Sci USA 102: 10706–10711.
Milad MR, Wright CI, Orr SP, Pitman RK, Quirk GJ, Rauch SL (2007). Recall of fear extinction in humans activates the ventromedial prefrontal cortex and hippocampus in concert. Biol Psychiatry 62: 446–454.
Perani D, Colombo C, Bressi S, Bonfanti A, Grassi F, Scarone S et al (1995). [18F]FDG PET study in obsessive-compulsive disorder. A clinical/metabolic correlation study after treatment. Br J Psychiatry 166: 244–250.
Phelps EA, Delgado MR, Nearing KI, LeDoux JE (2004). Extinction learning in humans: role of the amygdala and vmPFC. Neuron 43: 897–905.
Phillips ML, Drevets WC, Rauch SL, Lane R (2003). Neurobiology of emotion perception I: the neural basis of normal emotion perception. Biol Psychiatry 54: 504–514.
Pujol J, Soriano-Mas C, Alonso P, Cardoner N, Menchon JM, Deus J et al (2004). Mapping structural brain alterations in obsessive-compulsive disorder. Arch Gen Psychiatry 61: 720–730.
Radua J, Mataix-Cols D (2009). Voxel-wise meta-analysis of grey matter changes in obsessive-compulsive disorder. Br J Psychiatry 195: 393–402.
Radua J, van den Heuvel OA, Surguladze S, Mataix-Cols D (2010). Meta-analytical comparison of voxel-based morphometry studies in obsessive-compulsive disorder vs other anxiety disorders. Arch Gen Psychiatry 67: 701–711.
Rauch SL (2000). Neuroimaging research and the neurobiology of obsessive-compulsive disorder: where do we go from here? Biol Psychiatry 47: 168–170.
Rauch SL, Jenike MA, Alpert NM, Baer L, Breiter HC, Savage CR et al (1994). Regional cerebral blood flow measured during symptom provocation in obsessive-compulsive disorder using oxygen 15-labeled carbon dioxide and positron emission tomography. Arch Gen Psychiatry 51: 62–70.
Rosario-Campos MC, Miguel EC, Quatrano S, Chacon P, Ferrao Y, Findley D et al (2006). The Dimensional Yale-Brown Obsessive-Compulsive Scale (DY-BOCS): an instrument for assessing obsessive-compulsive symptom dimensions. Mol Psychiatry 11: 495–504.
Rosenberg DR, Benazon NR, Gilbert A, Sullivan A, Moore GJ (2000). Thalamic volume in pediatric obsessive-compulsive disorder patients before and after cognitive behavioral therapy. Biol Psychiatry 48: 294–300.
Rotge JY, Langbour N, Guehl D, Bioulac B, Jaafari N, Allard M et al (2010). Gray matter alterations in obsessive-compulsive disorder: an anatomic likelihood estimation meta-analysis. Neuropsychopharmacology 35: 686–691.
Saxena S, Brody AL, Ho ML, Alborzian S, Ho MK, Maidment KM et al (2001). Cerebral metabolism in major depression and obsessive-compulsive disorder occurring separately and concurrently. Biol Psychiatry 50: 159–170.
Saxena S, Brody AL, Ho ML, Alborzian S, Maidment KM, Zohrabi N et al (2002). Differential cerebral metabolic changes with paroxetine treatment of obsessive-compulsive disorder vs major depression. Arch Gen Psychiatry 59: 250–261.
Saxena S, Gorbis E, O’Neill J, Baker SK, Mandelkern MA, Maidment KM et al (2009). Rapid effects of brief intensive cognitive-behavioral therapy on brain glucose metabolism in obsessive-compulsive disorder. Mol Psychiatry 14: 197–205.
Saxena S, Rauch SL (2000). Functional neuroimaging and the neuroanatomy of obsessive-compulsive disorder. Psychiatr Clin North Am 23: 563–586.
Schwartz JM, Stoessel PW, Baxter Jr LR, Martin KM, Phelps ME (1996). Systematic changes in cerebral glucose metabolic rate after successful behavior modification treatment of obsessive-compulsive disorder. Arch Gen Psychiatry 53: 109–113.
Sotres-Bayon F, Cain CK, LeDoux JE (2006). Brain mechanisms of fear extinction: historical perspectives on the contribution of prefrontal cortex. Biol Psychiatry 60: 329–336.
Soumier A, Banasr M, Goff LK, Daszuta A (2009). Region- and phase-dependent effects of 5-HT(1A) and 5-HT(2C) receptor activation on adult neurogenesis. Eur Neuropsychopharmacol 20: 336–345.
Sousa MB, Isolan LR, Oliveira RR, Manfro GG, Cordioli AV (2006). A randomized clinical trial of cognitive-behavioral group therapy and sertraline in the treatment of obsessive-compulsive disorder. J Clin Psychiatry 67: 1133–1139.
Swedo SE, Pietrini P, Leonard HL, Schapiro MB, Rettew DC, Goldberger EL et al (1992). Cerebral glucose metabolism in childhood-onset obsessive-compulsive disorder. Revisualization during pharmacotherapy. Arch Gen Psychiatry 49: 690–694.
Szeszko PR, Christian C, Macmaster F, Lencz T, Mirza Y, Taormina SP et al (2008). Gray matter structural alterations in psychotropic drug-naive pediatric obsessive-compulsive disorder: an optimized voxel-based morphometry study. Am J Psychiatry 165: 1299–1307.
Szeszko PR, MacMillan S, McMeniman M, Lorch E, Madden R, Ivey J et al (2004). Amygdala volume reductions in pediatric patients with obsessive-compulsive disorder treated with paroxetine: preliminary findings. Neuropsychopharmacology 29: 826–832.
Szeszko PR, Robinson D, Alvir JM, Bilder RM, Lencz T, Ashtari M et al (1999). Orbital frontal and amygdala volume reductions in obsessive-compulsive disorder. Arch Gen Psychiatry 56: 913–919.
Talairach J, Tornoux P (1988). Co-planar Stereotaxic Atlas of the Human Brain. New York: Thieme Medical Publishers.
Tucker DM, Luu P, Pribram KH (1995). Social and emotional self-regulation. Ann NY Acad Sci 769: 213–239.
Valente Jr AA, Miguel EC, Castro CC, Amaro Jr E, Duran FL, Buchpiguel CA et al (2005). Regional gray matter abnormalities in obsessive-compulsive disorder: a voxel-based morphometry study. Biol Psychiatry 58: 479–487.
van den Heuvel OA, Remijnse PL, Mataix-Cols D, Vrenken H, Groenewegen HJ, Uylings HB et al (2009). The major symptom dimensions of obsessive-compulsive disorder are mediated by partially distinct neural systems. Brain 132 (Pt 4): 853–868.
Vikas A, Avasthi A, Sharan P (2009). Psychological impact of obsessive compulsive disorder on patients and their caregivers: a comparative study with depressive disorder. Int J Soc Psychiatry 57: 45–56.
Volpato Cordioli A, Heldt E, Braga Bochi D, Margis R, Basso de Sousa M, Fonseca Tonello J et al (2003). Cognitive-behavioral group therapy in obsessive-compulsive disorder: a randomized clinical trial. Psychother Psychosom 72: 211–216.
Acknowledgements
We thank Dr Cristina Belotto-Silva, Ms Sonia Borcatto, Dr Ana Gabriela Hounie, Ms Marines Alves Joaquim, Ms Ana Carolina Ferreira Rosa, and Ms Luciana Cristina Santos whose help was critical to the conduction of this project. We also thank Ms Dianne M Hezel for helpful comments on the manuscript. This study received financial support in the form of grants provided by the Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP, Foundation for the Support of Research in the State of São Paulo) to Dr Miguel (2005/55628-8) and from FAPESP scholarships to Dr Shavitt (06/61459-7), to Dr Diniz (06/50273-0), to Dr Lopes (2008/10257-0), and to Ms D’Alcante (06/58286-3). Dr Hoexter is supported by a PhD scholarship from FAPESP (2005/04206-6) and by a doctorate ‘sandwich’ scholarship from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Agency for Support and Evaluation of Graduate Education) (4375/08-4). This work was presented in part at the 48th Annual Meeting of the American College of Neuropsychopharmacology, 6–10 December 2009, Hollywood, Florida, USA.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Dr Hoexter, Dr Duran, Ms D’Alcante, Dr Shavitt, Dr Lopes, Dr Diniz, Mr Batistuzzo, and Dr Busatto have declared no conflict of interest. Dr Dougherty has acted as a consultant for Medtronic, Eli Lilly, Brand Ideas, McNeil, and Reed Elsevier, and has received research funding from Medtronic, Eli Lilly, McNeil, and Cyberonics. Dr Deckersbach's research has been funded by NIMH, NARSAD, TSA, OCF, and Tufts University. He has received honoraria, consultation fees, and/or royalties from the MGH Psychiatry Academy, BrainCells, Systems Research and Applications Corporation, Boston University, the Catalan Agency for Health Technology Assessment and Research, the National Association of Social Workers Massachusetts, the Massachusetts Medical Society, Tufts University, NIDA, German Research Foundation/Federal Ministry for Education and Research, and Oxford University Press. He has also participated in research funded by NIH, NIA, AHRQ, Janssen Pharmaceuticals, The Forest Research Institute, Shire Development, Medtronic, Cyberonics, and Northstar. Dr Bressan has received honoraria and/or consultations fees from Novartis, Eli Lilly, Janssen, and AstraZeneca. Dr Miguel has received lecture fees from Lundbeck and Solvay.
Additional information
Supplementary Information accompanies the paper on the Neuropsychopharmacology website
PowerPoint slides
Rights and permissions
About this article
Cite this article
Hoexter, M., de Souza Duran, F., D'Alcante, C. et al. Gray Matter Volumes in Obsessive-Compulsive Disorder Before and After Fluoxetine or Cognitive-Behavior Therapy: A Randomized Clinical Trial. Neuropsychopharmacol 37, 734–745 (2012). https://doi.org/10.1038/npp.2011.250
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/npp.2011.250
Keywords
This article is cited by
-
Volumetric MRI Findings in Mild Traumatic Brain Injury (mTBI) and Neuropsychological Outcome
Neuropsychology Review (2023)
-
Brief internet-delivered cognitive-behavioural intervention for children and adolescents with symptoms of anxiety and depression during the COVID-19 pandemic: a randomised controlled trial protocol
Trials (2022)
-
Structural neuroimaging biomarkers for obsessive-compulsive disorder in the ENIGMA-OCD consortium: medication matters
Translational Psychiatry (2020)
-
Layer-specific reduced neuronal density in the orbitofrontal cortex of older adults with obsessive–compulsive disorder
Brain Structure and Function (2019)
-
Cortical Thickness and Subcortical Gray Matter Volume in Pediatric Anxiety Disorders
Neuropsychopharmacology (2017)
