
Abstract
Idiopathic achalasia is characterized by a failure of the lower esophageal sphincter to relax due to a loss of neurons in the myenteric plexus1,2. This ultimately leads to massive dilatation and an irreversibly impaired megaesophagus. We performed a genetic association study in 1,068 achalasia cases and 4,242 controls and fine-mapped a strong MHC association signal by imputing classical HLA haplotypes and amino acid polymorphisms. An eight-residue insertion at position 227–234 in the cytoplasmic tail of HLA-DQβ1 (encoded by HLA-DQB1*05:03 and HLA-DQB1*06:01) confers the strongest risk for achalasia (P = 1.73 × 10−19). In addition, two amino acid substitutions in the extracellular domain of HLA-DQα1 at position 41 (lysine encoded by HLA-DQA1*01:03; P = 5.60 × 10−10) and of HLA-DQβ1 at position 45 (glutamic acid encoded by HLA-DQB1*03:01 and HLA-DQB1*03:04; P = 1.20 × 10−9) independently confer achalasia risk. Our study implies that immune-mediated processes are involved in the pathophysiology of achalasia.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others
References
Gockel, H.R. et al. Achalasia: will genetic studies provide insights? Hum. Genet. 128, 353–364 (2010).
Park, W. & Vaezi, M.F. Etiology and pathogenesis of achalasia: the current understanding. Am. J. Gastroenterol. 100, 1404–1414 (2005).
de Bakker, P.I. et al. A high-resolution HLA and SNP haplotype map for disease association studies in the extended human MHC. Nat. Genet. 38, 1166–1172 (2006).
Jia, X. et al. Imputing amino acid polymorphisms in human leukocyte antigens. PLoS ONE 8, e64683 (2013).
Senju, S. et al. Allele-specific expression of the cytoplasmic exon of HLA-DQB1 gene. Immunogenetics 36, 319–325 (1992).
Raychaudhuri, S. et al. Five amino acids in three HLA proteins explain most of the association between MHC and seropositive rheumatoid arthritis. Nat. Genet. 44, 291–296 (2012).
Pos, W. et al. Crystal structure of the HLA-DM–HLA-DR1 complex defines mechanisms for rapid peptide selection. Cell 151, 1557–1568 (2012).
Khalil, H. et al. The MHC class II β chain cytoplasmic tail overcomes the invariant chain p35-encoded endoplasmic reticulum retention signal. Int. Immunol. 15, 1249–1263 (2003).
Parkes, M., Cortes, A., van Heel, D.A. & Brown, M.A. Genetic insights into common pathways and complex relationships among immune-mediated diseases. Nat. Rev. Genet. 14, 661–673 (2013).
Tollefsen, S. et al. Structural and functional studies of trans-encoded HLA-DQ2.3 (DQA1*03:01/DQB1*02:01) protein molecule. J. Biol. Chem. 287, 13611–13619 (2012).
Robinson, J. et al. The IMGT/HLA database. Nucleic Acids Res. 39, D1171–D1176 (2011).
Schmermund, A. et al. Assessment of clinically silent atherosclerotic disease and established and novel risk factors for predicting myocardial infarction and cardiac death in healthy middle-aged subjects: rationale and design of the Heinz Nixdorf RECALL Study. Risk Factors, Evaluation of Coronary Calcium and Lifestyle. Am. Heart J. 144, 212–218 (2002).
Trynka, G. et al. Dense genotyping identifies and localizes multiple common and rare variant association signals in celiac disease. Nat. Genet. 43, 1193–1201 (2011).
Manichaikul, A. et al. Robust relationship inference in genome-wide association studies. Bioinformatics 26, 2867–2873 (2010).
Browning, B.L. & Browning, S.R. A unified approach to genotype imputation and haplotype-phase inference for large data sets of trios and unrelated individuals. Am. J. Hum. Genet. 84, 210–223 (2009).
Purcell, S. et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 81, 559–575 (2007).
SAS Institute, Inc. SAS/STAT 9.2 User's Guide (SAS Institute, Inc., Cary, NC, 2008).
Acknowledgements
We thank all subjects for participating to this study. We acknowledge our collaborating clinical partners, all colleagues who contributed to patient recruitment, and our laboratory technicians and colleagues responsible for database management (for a complete list of all individuals, see the Supplementary Note). I.G., M.K. and J.S. received support for this work from the Deutsche Forschungsgemeinschaft (DFG), individual grants GO 1795/1-1, KN 378/2-1 and SCHU 1596/5-1. M.M.N. received support for this work from the Alfried Krupp von Bohlen und Halbach-Stiftung. M.M.N. is a member of the DFG-funded Excellence Cluster ImmunoSensation. The Heinz Nixdorf Recall cohort was established with the generous support of the Heinz Nixdorf Foundation, Germany. We thank B. Pötzsch (University of Bonn) for help with collecting DNA samples from anonymous blood donors. In addition, we thank the Type I Diabetes Genetics Consortium (T1DGC) for data access and J. Sauter (German Bone Marrow Donor Center (DKMS), Tübingen) for help differentiating HLA-DQA1 alleles. P.I.W.d.B. is the recipient of a Vernieuwingsimpuls VIDI Award from the Netherlands Organization for Scientific Research (NWO project 016.126.354). M.M.W. is supported by a postdoctoral fellowship of the Fund for Scientific Research (FWO) Flanders, Belgium. G.E.B. is supported by a grant from the Research Foundation–Flanders (FWO) (Odysseus program). K.-P.H. is supported by DFG SFB 684 and the Center for Integrated Protein Sciences Munich.
Author information
Authors and Affiliations
Contributions
H.L., I.G., J.B., J.S., M.M.N. and M.T.H. initiated the study. J.B., J.S., K.-P.H., M.K. and P.I.W.d.B. analyzed and interpreted the data. D.R., J.B., J.T., J.Z., M.M.W. and T.H. prepared the DNA and performed the molecular genetic experiments. A.G.V., A.J.E., A.L., A.R.d.L., B.H.A.v.R., D.D., E.M., E.U., G.E.B., G.S., H.-D.A., H.R.G., H.G.S., I.G., J.P.d.l.S., J.U.M., L.L., M. Müller, P.R.G., R.C., R.K., S. Heilmann, S.N., U.F., V.A. and W.K. clinically characterized the achalasia cases and/or collected blood samples from cases and/or controls. C.W., G.T., H.-J.W., L.F. and V.K. provided genotype data from the Dutch, Italian and Spanish controls. M. Mattheisen, P.H. and S. Herms provided database management. I.G., J.B., J.S., M.K. and M.M.N. prepared the manuscript, with feedback from the other authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Integrated supplementary information
Supplementary Figure 1 Association results within the MHC region.
(a) The strongest genetic determinant of achalasia risk represents an 8-residue insertion at position 227–234 in HLA-DQβ1. (b) Subsequent conditional analysis controlling for this insertion as well as for amino acid changes at position 41/130 in HLA-DQα1 and position 45 in HLA-DQβ1 revealed no further independent association within the MHC region (P > 1 × 10−6).
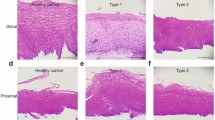
Supplementary Figure 2 Comparison of disease risk predicted by two different models.
This figure shows the comparison of the disease risk predicted by a full logistic regression model in which each HLA-DQ allele confers its own unique risk (y axis) with the disease risk predicted by a simpler logistic regression model in which risk is defined by HLA-DQβ1 positions 227–234 and 45 as well as HLA-DQα1 position 41/130 (x axis). Patients are represented in red, and controls are represented in blue.
Supplementary Figure 3 Multidimensional scaling (MDS) analysis.
Representation of our study sample and HapMap individuals for the first two dimensions obtained by multidimensional scaling analysis of a matrix of pairwise IBS (identical-by-state) distance values between samples.
Supplementary information
Supplementary Text and Figures
Supplementary Figures 1–3, Supplementary Tables 1–9 and Supplementary Note. (PDF 1032 kb)
Supplementary Table 10
Imputation of classical HLA haplotypes. (XLSX 44 kb)
Rights and permissions
About this article

Cite this article
Gockel, I., Becker, J., Wouters, M. et al. Common variants in the HLA-DQ region confer susceptibility to idiopathic achalasia. Nat Genet 46, 901–904 (2014). https://doi.org/10.1038/ng.3029
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ng.3029
This article is cited by
-
Ethnic Differences in Clinical Presentations and Esophageal High-Resolution Manometry Findings in Patients with Achalasia
Dysphagia (2023)
-
Update on the Diagnosis and Treatment of Achalasia
Dysphagia (2023)
-
Disorders of the enteric nervous system — a holistic view
Nature Reviews Gastroenterology & Hepatology (2021)
-
Elevated risk of invasive group A streptococcal disease and host genetic variation in the human leucocyte antigen locus
Genes & Immunity (2020)
-
Motilitätsstörungen des Ösophagus
Gastro-News (2020)
