
Abstract
Arising from L. M. Mangravite et al. Nature 502, 377–380 (2013); doi:10.1038/nature12508
Mangravite et al.1 identified six expression quantitative loci (eQTLs) that interacted with simvastatin exposure by using 480 lymphoblastoid cell lines exposed to β-hydroxy simvastatin acid in vitro. One of these SNPs (rs9806699) within the glycine amidinotransferase (GATM) gene was shown to have an association with statin-induced myopathy in two independent cohorts (n = 172 myopathy cases), conferring a protective effect (odds ratio = 0.61, 95% confidence interval = 0.39–0.95, P = 0.03). Our genotyping results from statin myopathy patients do not appear to replicate this finding. There is a Reply to this Brief Communication Arising by Mangravite, L. M. et al. Nature 513, http://dx.doi.org/10.1038/nature13630 (2014).
Similar content being viewed by others


Main
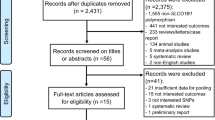
Using primarily the UK Clinical Practice Research Datalink, an electronic healthcare record database, we recruited 145 cases with statin-induced myopathy and 537 statin-exposed control patients2. In addition, five patients meeting our case inclusion criteria were identified prospectively through a tertiary adult muscle clinic. Our myopathy phenotype was defined as serum creatine kinase levels of greater than 4 × upper limit of normal (ULN) or clinical record of rhabdomyolysis concurrent with statin prescription. In a proof-of-concept study, using a subset of patients (78 cases, 372 controls)3 we were able to show an association between the SLCO1B1*5 allele (rs4149056) and both statin-induced myopathy (odds ratio = 2.1, 95% confidence interval = 1.3–3.1) and severe myopathy (n = 23, odds ratio = 4.1, 95% confidence interval = 2.1–8.2), consistent with the genome-wide association study (GWAS) findings from the SEARCH collaborative4.
We have undertaken genotyping for the rs9806699 GATM single-nucleotide polymorphism (SNP) in our cases and drug-exposed control patients (n = 150 and 587, respectively, after quality control) in order to attempt replication of the association shown by Mangravite et al.1. However, we were unable to show a significant difference in the minor allele frequency of rs9806699 between myopathy cases (MAF = 0.28) and controls (MAF = 0.30) (odds ratio = 0.94, P = 0.68). The MAF in our cases was similar to that identified in controls in the paper by Mangravite et al.1. By limiting cases to just those with ‘severe’ myopathy (creatine kinase > 10 × ULN or rhabdomyolysis) (n = 37), we again failed to show a significant difference in MAF between cases and controls (odds ratio = 0.94, P = 0.83). Further analysis restricted to patients only receiving simvastatin (99 cases, 344 controls) also did not demonstrate an association between rs9806699 and risk of either myopathy (odds ratio = 1.12, P = 0.49) or severe myopathy (n = 26, odds ratio = 1.42, P = 0.24). Analysis restricted to the 120 cases that were not on drugs known to interact with statins also did not change the result. We have also undertaken genome wide analysis of 128 myopathy cases (Illumina Human OmniExpress Exome 8v1), and comparison with the WTCCC2 (Wellcome Trust Case Control Consortium 2) genotype data also did not show any association between statin myopathy (generalized or severe) and any of 90 typed or imputed SNPs within the GATM gene locus.
In conclusion, we have not been able to replicate the association between the rs9806699 GATM SNP and statin myopathy reported by Mangravite et al.1 in an independent sample set despite the fact that all patients were of European ancestry and had similar statin-myopathy phenotypes. This association will need to be assessed in more patients, and through an individual patient-data meta-analysis to determine, first, whether the SNP is relevant to a sub-phenotype of statin myopathy, and second, its clinical and mechanistic relevance.
References
Mangravite, L. M. et al. A statin-dependent QTL for GATM expression is associated with statin-induced myopathy. Nature 502, 377–380 (2013)
O’Meara, H. et al. Electronic health records for biological sample collection: feasibility study of statin-induced myopathy using the clinical practice research datalink. Br. J. Clin. Pharmacol. 77, 831–838 (2014)
Carr, D. F. et al. SLCO1B1 genetic variant associated with statin-induced myopathy: a proof-of-concept study using the clinical practice research datalink. Clin. Pharmacol. Ther. 94, 695–701 (2013)
The SEARCH Collaborative Group SLCO1B1 variants and statin-induced myopathy—a genomewide study. N. Engl. J. Med. 359, 789–799 (2008)
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Carr, D., Alfirevic, A., Johnson, R. et al. GATM gene variants and statin myopathy risk. Nature 513, E1 (2014). https://doi.org/10.1038/nature13628
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nature13628
This article is cited by
-
Correlation between single-nucleotide polymorphisms and statin-induced myopathy: a mixed-effects model meta-analysis
European Journal of Clinical Pharmacology (2021)
-
The association of GATM polymorphism with statin-induced myopathy: a systematic review and meta-analysis
European Journal of Clinical Pharmacology (2021)
-
Muscle phenotype of AGAT- and GAMT-deficient mice after simvastatin exposure
Amino Acids (2020)
-
GATM locus does not replicate in rhabdomyolysis study
Nature (2014)
-
Mangravite et al. reply
Nature (2014)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
