
Abstract
Deficits in eye contact have been a hallmark of autism1,2 since the condition’s initial description3. They are cited widely as a diagnostic feature4 and figure prominently in clinical instruments5; however, the early onset of these deficits has not been known. Here we show in a prospective longitudinal study that infants later diagnosed with autism spectrum disorders (ASDs) exhibit mean decline in eye fixation from 2 to 6 months of age, a pattern not observed in infants who do not develop ASD. These observations mark the earliest known indicators of social disability in infancy, but also falsify a prior hypothesis: in the first months of life, this basic mechanism of social adaptive action—eye looking—is not immediately diminished in infants later diagnosed with ASD; instead, eye looking appears to begin at normative levels prior to decline. The timing of decline highlights a narrow developmental window and reveals the early derailment of processes that would otherwise have a key role in canalizing typical social development. Finally, the observation of this decline in eye fixation—rather than outright absence—offers a promising opportunity for early intervention that could build on the apparent preservation of mechanisms subserving reflexive initial orientation towards the eyes.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 51 print issues and online access
$199.00 per year
only $3.90 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


References
Grice, S. J. et al. Neural correlates of eye-gaze detection in young children with autism. Cortex 41, 342–353 (2005)
Jones, W., Carr, K. & Klin, A. Absence of preferential looking to the eyes of approaching adults predicts level of social disability in 2-year-olds with autism spectrum disorder. Arch. Gen. Psychiatry 65, 946–954 (2008)
Kanner, L. Autistic disturbances of affective contact. Nerv. Child 2, 217–250 (1943)
Volkmar, F. R., Lord, C., Bailey, A., Schultz, R. T. & Klin, A. Autism and pervasive developmental disorders. J. Child Psychol. Psychiatry 45, 135–170 (2004)
Lord, C., Rutter, M., DiLavore, P. & Risi, S. Autism Diagnostic Observation Schedule 2nd edn (Western Psychological Services, 2008)
Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders — Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States, 2008. MMWR Surveillance Summaries 61, 1–19 (2012)
Constantino, J. N. et al. Autism recurrence in half siblings: strong support for genetic mechanisms of transmission in ASD. Mol. Psychiatry 18, 137–138 (2013)
State, M. W. & Sestan, N. Neuroscience: the emerging biology of autism spectrum disorders. Science 337, 1301–1303 (2012)
Oyama, S. The Ontogeny of Information: Developmental Systems and Evolution 2nd edn (Duke Univ. Press, 2000)
Jones, W. & Klin, A. Heterogeneity and homogeneity across the autism spectrum: the role of development. J. Am. Acad. Child Adolesc. Psychiatry 48, 471–473 (2009)
DeCasper, A. J. & Fifer, W. P. Of human bonding: newborns prefer their mothers' voices. Science 208, 1174–1176 (1980)
Haith, M. M., Bergman, T. & Moore, M. J. Eye contact and face scanning in early infancy. Science 198, 853–855 (1977)
Johnson, M. H. Subcortical face processing. Nature Rev. Neurosci. 6, 766–774 (2005)
Simion, F., Regolin, L. & Bulf, H. A predisposition for biological motion in the newborn baby. Proc. Natl Acad. Sci. USA 105, 809–813 (2008)
Johnson, M. H. Functional brain development in humans. Nature Rev. Neurosci. 2, 475–483 (2001)
Rosa Salva, O., Farroni, T., Regolin, L., Vallortigara, G. & Johnson, M. H. The evolution of social orienting: evidence from chicks (Gallus gallus) and human newborns. PLoS ONE 6, e18802 (2011)
Klin, A., Jones, W., Schultz, R. T. & Volkmar, F. The enactive mind — from actions to cognition: lessons from autism. Phil. Trans. R. Soc. B 358, 345–360 (2003)
Klin, A., Lin, D. J., Gorrindo, P., Ramsay, G. & Jones, W. Two-year-olds with autism fail to orient towards human biological motion but attend instead to non-social, physical contingencies. Nature 459, 257–261 (2009)
Ozonoff, S. et al. Recurrence risk for autism spectrum disorders: a Baby Siblings Research Consortium study. Pediatrics 128, e488–e495 (2011)
Chawarska, K., Klin, A., Paul, R. & Volkmar, F. R. Autism spectrum disorders in the second year: stability and change in syndrome expression. J. Child Psychol. Psychiatry 48, 128–138 (2007)
Ramsay, J. O. & Silverman, B. W. Functional Data Analysis 2nd edn (Springer-Verlag, 2006)
Yao, F., Müller, H. G. & Wang, J. L. Functional data analysis for sparse longitudinal data. J. Am. Stat. Assoc. 100, 577–590 (2005)
Singer, J. D. & Willett, J. B. Applied Longitudinal Data Analysis (Oxford Univ. Press, New York, 2003)
Mosteller, F. & Tukey, J. W. Data Analysis and Regression 37 (Addison-Wesley, 1977)
Stone, M. Cross-validatory choice and assessment of statistical predictions. J. R. Stat. Soc. B 36, 111–147 (1974)
Steer, C. D., Golding, J. & Bolton, P. F. Traits contributing to the autistic spectrum. PLoS ONE 5, e12633 (2010)
Horn, G., Nicol, A. U. & Brown, M. W. Tracking memory’s trace. Proc. Natl Acad. Sci. USA 98, 5282–5287 (2001)
Johnson, M. H. & Karmiloff-Smith, A. In Theories of Infant Development (eds Bremner, G. & Slater, A. ) 121–141 (Blackwell, 2004)
Abrahams, B. S. & Geschwind, D. H. Advances in autism genetics: on the threshold of a new neurobiology. Nature Rev. Genet. 9, 341–355 (2008)
Klin, A. et al. Social and communication abilities and disabilities in higher functioning individuals with autism spectrum disorders. J. Autism Dev. Disord. 37, 748–759 (2007)
Speer, L. L., Cook, A. E., McMahon, W. M. & Clark, E. Face processing in children with autism: effects of stimulus contents and type. Autism 11, 265–277 (2007)
Shultz, S., Klin, A. & Jones, W. Inhibition of eye blinking reveals subjective perceptions of stimulus salience. Proc. Natl Acad. Sci. USA 108, 21270–21275 (2011)
Leigh, R. J. & Zee, D. S. The Neurology of Eye Movements 3rd edn (Oxford Univ. Press, 1999)
Hall, P., Müller, H.-G. & Yao, F. Estimation of functional derivatives. Ann. Stat. 37, 3307–3329 (2009)
Liu, B. & Müller, H. G. Estimating derivatives for samples of sparsely observed functions, with application to online auction dynamics. J. Am. Stat. Assoc. 104, 704–717 (2009)
Tang, R. & Müller, H.-G. Pairwise curve synchronization for functional data. Biometrika 95, 875–889 (2008)
Burchinal, M., Nelson, L. & Poe, M. In Best Practices in Quantitative Methods for Developmentalists (eds McCartney, K., Burchinal, M. & Bub, K. ) Monogr. Soc. Res. Child Dev. 71, 65–87 (2006)
Acknowledgements
This work was supported by grants from the Simons Foundation and the National Institute of Mental Health (R01 MH083727). Additional support was provided by the Marcus Foundation, the Whitehead Foundation, and the Georgia Research Alliance. We wish to thank the families and children for their time and participation. We also wish to thank S. Habayeb, S. Glazer, M. Ly, T. Tsang, J. Jones, A. Trubanova, J. Borjon, J. Moriuchi, K. Rice, J. Northrup, L. Edwards, J. Xu, S. Shultz, A. Krasno, C. Zampella, K. Knoch, D. Lin, K. Carr and A. Blank for their assistance in data collection and processing; P. Lewis, J. Paredes, P. Gorrindo and M. Ackerman for assistance in designing and building laboratory hardware and software; G. Ramsay and C. McCracken for discussions of data analysis and statistics; I. Zilber, A. Margolis, D. Blum, M. Dye, D. Simeone, A. Smith and K. O’Loughlin for project supervision, coordination, and data collection; T. Babitz for administrative support; and K. Chawarska, C. Saulnier, K. Bearss, S. Macari, R. Paul, A. Carney, T. Goldsmith, A. Steiner, G. Gengoux, D. Goudreau, E. Loring, J. McGrath and A. Gupta for their contributions to the clinical characterization of the samples.
Author information
Authors and Affiliations
Contributions
W.J. and A.K. developed the initial idea and design of the study, interpreted data, wrote the final manuscript, had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. W.J. and A.K. performed final revision of the manuscript for content. A.K. supervised participant characterization. W.J. supervised technological developments and technical aspects of experimental procedure, data acquisition and analysis.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Extended data figures and tables
Extended Data Figure 1 In infants later diagnosed with ASD, decline in eye fixation during the first 2 years is significantly associated with outcome levels of symptom severity.
Functional principal component analysis (FPCA) was used to extract growth curve components explaining variance in trajectory shape about the population mean. a, Population mean for fixation to eyes in children with ASD (red line) plotted with lines indicating direction of individual trajectories having positive principal component one (PC1) scores (line marked by plus signs) or negative PC1 scores (line marked by minus signs). b, Outcome levels of social disability (as measured by ADOS Social Affect) as a function of decline in eye fixation (measured as eyes PC1 score). c, Outcome levels of social disability as a function of decline in eye fixation using subsets of the longitudinal data (that is, measuring decline in eye fixation using only data collected from month 2 to 6, excluding data thereafter; then from month 2 to 9, 2 to 12, 2 to 15, and 2 to 18). Decline in eye fixation predicts future outcome at trend levels by the developmental period from 2 to 9 months (P = 0.100), and is statistically significant thereafter.
Extended Data Figure 2 Developmental differences in visual fixation between 2 and 6 months of age.
a–l, Raw data for eyes fixation (a–c), mouth fixation (d–f), body fixation (g–i), and object fixation (j–l) between 2 and 6 months for typically developing infants (in blue) and infants later diagnosed with autism spectrum disorders (in red). Darkly shaded data markers indicate the interquartile range (spanning 25th to 75th percentiles). Data show significant associations with chronological age, but the slopes of the associations differ for ASD and TD outcome groups, with significant interactions of diagnosis by age for eyes, F1,787.928 = 9.27, P = 0.002; for body, F1,25.557 = 5.88, P = 0.023; and for object, F1,21.947 = 5.24, P = 0.032; but not for mouth, F1,47.298 = 0.019, P = 0.89. Analyses by HLM. Plots in c, f, i and l show mean trend lines and 95% confidence intervals.
Extended Data Figure 3 Percentage of total time spent fixating and saccading between 2 and 6 months of age.
a–f, Raw data for percentage of total time spent fixating (a–c) and time spent saccading (d–f) between 2 and 6 months for typically developing infants (in blue) and infants later diagnosed with autism spectrum disorders (in red). Darkly shaded data markers indicate the interquartile range (spanning 25th to 75th percentiles). Data show significant associations with chronological age, but the slopes of the associations do not differ for ASD and TD outcome groups, F1,20.026 = 0.88, P = 0.359 for time spent fixating; and F1,26.430 = 0.56, P = 0.460 for time spent saccading. Analyses by HLM. Plots in c and f show mean trend lines and 95% confidence intervals.
Extended Data Figure 4 Developmental change in visual fixation between 2 and 24 months of age in typically developing children.
a, c, e, g, Raw data for eyes fixation (a), mouth fixation (c), body fixation (e) and object fixation (g) between 2 and 24 months for typically developing children. Black lines indicates mean growth curves via hierarchical linear modelling (HLM). b, d, f, h, Mean fixation curves with 95% confidence intervals for eyes fixation (b), mouth fixation (d), body fixation (f) and object fixation (h) between 2 and 24 months for typically developing children. i–l Raw data for eyes fixation (i), mouth fixation (j), body fixation (k) and object fixation (l) between 2 and 6 months (top row), and 2 and 24 months (bottom row), together with individual fits, in black, for typically developing external validation sample (n = 4). Throughout all plots, darkly shaded data markers indicate the interquartile range (spanning 25th to 75th percentiles).
Extended Data Figure 5 Developmental change in visual fixation between 2 and 24 months of age in children with ASD.
a, c, e, g, Raw data for eyes fixation (a), mouth fixation (c), body fixation (e) and object fixation (g) between 2 and 24 months for children with ASD. Black lines indicates mean growth curves via hierarchical linear modelling (HLM). b, d, f, h, Mean fixation curves with 95% confidence intervals for eyes fixation (b), mouth fixation (d), body fixation (f) and object fixation (h) between 2 and 24 months for children with ASD. i–l Raw data for eyes fixation (i), mouth fixation (j), body fixation (k) and object fixation (l) between 2 and 6 months (top row), and 2 and 24 months (bottom row), together with individual fits, in black, for external validation sample of children infants later diagnosed with ASD (n = 2). Throughout all plots, darkly shaded data markers indicate the interquartile range (spanning 25th to 75th percentiles).
Extended Data Figure 6 Developmental change in visual fixation on the eyes relative to outcome levels of affectedness.
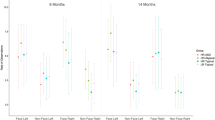
a–m, Per cent fixation on eyes for typically developing infants (a), infants at high-risk for ASD who showed no evidence of ASD at 36 months (c) (HR-ASD_No-Dx), infants at high-risk for ASD who showed some subthreshold signs of the broader autism phenotype at 36 months but did not meet clinical best estimate diagnosis of ASD (e) (HR-ASD_BAP), and infants diagnosed with ASD at 36 months (g). External validation participants not included (compare to Fig. 4). Darkly shaded data markers indicate the interquartile range (spanning 25th to 75th percentiles). Black lines indicate mean growth curves from hierarchical linear modelling (HLM). Plots in b, d, f and h show mean fixation curves with 95% confidence intervals. Plots i–l highlight the first 6 months of life in each group, and m plots the relationship across groups.
Extended Data Figure 7 Mean fixation curves by PACE and FDA with the effects of adding or subtracting principal component
functions (following the convention of Ramsay and Silverman, ref. 21). a–d, Fixation for typically developing infants (in blue) and infants with ASD (in red). a, Eye fixation. b, Mouth fixation. c, Body fixation. d, Object fixation. For each region and each group, the number of plots is dictated by number of principal component (PC) functions. The number of PC functions was determined by the Akaike Information Criterion. The fraction of variance explained (FVE) is given in parentheses in the upper left corner of each plot. The mean functions in each case match those plotted in Fig. 2. In all parts, + signs indicate the addition of PC functions; − signs indicate the subtraction of PC functions.
Extended Data Figure 8 Calibration accuracy from 2 until 24 months of life in TD children and in children diagnosed with an ASD.
a–c, In plots in a, the cross marks the location of mean calibration accuracy, and the annulus marks the 95% confidence interval (CI). In b, kernel density estimates plot the distribution of fixation locations relative to fixation targets for TD children. In c, kernel density estimates plot the distribution of fixation locations relative to fixation targets for children diagnosed with an ASD. Smoothing bandwidth for kernel density estimates was equal to 1°. Targets for testing calibration accuracy consisted of spinning and/or flashing points of light and cartoon animations, ranging in size from 1° to 1.5° of visual angle, presented on an otherwise blank screen, all with accompanying sounds.
Extended Data Figure 9 Growth charts of social visual engagement and their relationship to dimensional and categorical outcome, with data from month 2 included versus excluded.
a–d, Comparison of growth curves with month 2 data included or excluded for a, typically developing males (TD, in blue) and, b, for males with an ASD (in red). Exclusion of the month-2 data does not significantly alter the trajectories themselves, and it does not alter the between-group comparisons. c, Outcome levels of social disability (as measured by ADOS social-affect score) as a function of decline in eyes fixation (measured as eyes PC1 score, as in Extended Data Fig. 1) using subsets of the longitudinal data (that is, decline in eye fixation using only data collected from month 2 to 6 or 3 to 6, excluding data thereafter; then from months 2 to 9 or 3 to 9, and so on). In the top row, month-2 data are included; in the bottom row, month-2 data are excluded. When month-2 data are included or excluded, decline in eye fixation still significantly predicts future outcome; this relationship reaches trend level significance by the developmental period from months 3 to 9 (P = 0.097), and is statistically significant thereafter (with r = −0.714, P = 0.014 for 3 to 12 months). d, ROC curves for comparison of overlap in values between infants with confirmed ASD outcomes relative to typically developing infants. Using leave-one-out cross-validation, plots show mean and 95% confidence intervals for comparison of overlap in values based on change in eye fixation (first two plots from left), change in body fixation (middle two plots), and change in both eye and body fixation (last two plots at right) between 2 and 6 months of age. Plots show ROC for comparison of overlap in values using data from months 2 to 6 and for the comparison of month 2 to 6 relative to month 3 to 6. With month-2 data excluded, confidence intervals for the cross-validated ROC curves increase in size (as expected, in proportion to the reduction in data by excluding month 2), but the curves remain significantly different from chance, and the ROC curves with month-2 data included or excluded are not significantly different from one another.
Supplementary information
Supplementary Information
This file contains Supplementary Text and Data and Supplementary References – see contents page in document for details. (PDF 379 kb)
Rights and permissions
About this article
Cite this article
Jones, W., Klin, A. Attention to eyes is present but in decline in 2–6-month-old infants later diagnosed with autism. Nature 504, 427–431 (2013). https://doi.org/10.1038/nature12715
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nature12715
This article is cited by
-
Feasibility of a 2-minute eye-tracking protocol to support the early identification of autism
Scientific Reports (2024)
-
Joint Attention: Normativity and Sensory Modalities
Topoi (2024)
-
Correlation Between Gaze Behaviors and Social Communication Skills of Young Autistic Children: A Meta-Analysis of Eye-Tracking Studies
Journal of Autism and Developmental Disorders (2024)
-
Eye-tracking correlates of response to joint attention in preschool children with autism spectrum disorder
BMC Psychiatry (2023)
-
Endophenotype trait domains for advancing gene discovery in autism spectrum disorder
Journal of Neurodevelopmental Disorders (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
