
Abstract
Replying to: M. R. Dawson et al. Nature 461, 10.1038/nature08254 (2009)
Commenting on ref. 1, Dawson et al.2 claim that metastasis formation is independent of VEGFR1 activity, contradicting work by us and many others, including the original description of flt1TK-/- (VEGFR1-TK-/-) mice in the metastatic setting3. Contrasting the findings by Dawson et al.2, here we show that VEGFR1 knockdown in myelomonocytic cells eradicates micro- and macrometastases in a non-amputation/resection tumour model.
Similar content being viewed by others


Main
Hiratsuka et al.3 originally reported that flt1TK-/- mice have impaired metastatic progression due to a significant reduction in MMP9+CD11b+ (Mac1+) cell infiltration in pre-metastatic lungs following inoculation with LLC or B16 tumour cells. Moreover, several reports demonstrate that inhibition of VEGFR1 by anti-VEGFR1 peptide blocks micro- and macrometastasis, while overexpression of placental growth factor (PlGF), which signals exclusively through VEGFR1, increases metastatic spread4,5. Thus, caution is necessary when drawing conclusions from the findings of Dawson et al.2 regarding the role of VEGFR1 in metastasis.
In deviation from metastasis models used by us and others to document the existence of the pre-metastatic niche1,3,6,7,8,9, Dawson et al.2 use a model whereby primary tumours were implanted in the hind limb and resected by amputation of the leg, thus producing a sizeable wound before examining metastatic progression in the lung. Resection of the primary tumour at this early time point eliminates several tumour-derived paracrine factors, including VEGF-A, TNF-α, TGF-β, S100A8-SAA36,7, lysyl oxidase8, IL6 and versican9, factors that have been shown to recruit myeloid cells to the pre-metastatic niche and promote metastatic progression. Thus, it is plausible that removal of the primary tumour and generation of a traumatic wound caused a significant modulation of systemic metastatic niche supportive factors, resulting in disabled recruitment and/or function of VEGFR1-expressing bone marrow-derived cells (BMDCs), at metastatic sites. Although their experimental design may provide a relevant model for the effects of primary surgical resection on metastasis, the findings by Dawson et al.2 cannot exclude VEGFR1 function in metastasis in non-tumour resection/amputation models.
The methodology used to evaluate metastasis in the lung by Dawson et al.2 was insufficient and further confounds interpretation of their findings. Metastasis was evaluated grossly by counting metastatic nodules (Fig. 1; ref. 2). More quantitative measures may yield differing results, given both the risk of underestimating tumour burden by gross examination and the role VEGFR1 may play in both micro- and macrometastatic disease.

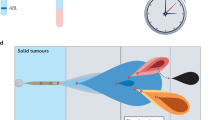
a, Schematic showing experimental design. Lineage-depleted bone marrow cells were transduced with a lentiviral vector driving ubiquitous expression of VEGFR1 shRNA. Transduced cells were used for bone marrow transplants. Six to eight weeks after transplantation, mice were given subcutaneous injections of mCherry-B16 tumour cells (day 0) and lungs were analysed at day 17 and day 30. b, Time course indicating primary tumour volume (v) throughout the experiment; v was calculated using v = (lwh)/(2π/3), where l is length, w is width and h is height; n = 7 for days 0–17; n = 4 for days 18–26. c, Quantitative PCR analysis of VEGFR1 expression in peripheral blood of VEGFR1 shRNA mice at days 17 and 30. Data are represented as percentage of mRNA expression compared to average of vector control mice (n = 4). d, Images illustrating visible metastatic foci in lungs at day 30 after B16 melanoma tumour injection. Data are mean visible metastatic foci per lung ± s.e.m. (n = 4). e, Quantitative PCR analysis of tumour-derived mCherry expression in lungs at day 30 (n = 4). f, Quantification of micrometastatic lesions (defined by >20 tumour cells) visible per lung section at day 30. Six sections per mouse (n = 4). Data are mean ± s.e.m. **P < 0.01, Student’s t-test.
Many studies have confirmed that infiltration of myeloid cells is essential for metastasis10,11. Current data suggest that many pro-angiogenic myeloid cells express VEGFR112,13. Furthermore, these studies highlight inhibition of VEGFR1 to target metastasis and PlGF-dependent tumour models in which VEGFR1 signalling is specifically targeted10,14. In these models, there is a profound defect in recruitment of pro-angiogenic and pre-metastatic VEGFR1+ myeloid cells, resulting in a reduction of metastasis.
An additional important consideration is that a complete absence of VEGFR1-mediated signalling in the flt1TK-/- mouse model used in this study has not been proven. Given the promiscuity of tyrosine kinase receptors, it is likely that the extracellular domain of the kinase retains some signalling activity through cross-talk with other activated tyrosine kinases or integrins. This residual activity is also supported by the finding that flt1TK-/- mice are viable, while mice lacking the full-length VEGFR1 die in utero15. In addition, VEGFR1 is expressed in many different cell types, including haematopoietic, endothelial and stromal cells, and non-cell-specific deletion of VEGFR1 in this model does not specifically address the role of its expression in BMDCs.
To address this question and expand on the brief functional analyses of VEGFR1 inhibition presented in ref. 1, we used lentiviral vectors to knockdown VEGFR1 activity specifically in BMDCs (Fig. 1a). Consistent with other reports1,3,7, inhibition of VEGFR1 by short hairpin (sh)RNA did not significantly alter primary B16 melanoma tumour growth (Fig. 1b, c). However, analysis of the lungs 30 days post-implantation revealed a pronounced reduction in the number of metastatic lesions and total tumour burden in mice with bone marrow transduced with VEGFR1 shRNA as compared to controls (Fig. 1d–f). This observation indicates that VEGFR1 expression by BMDCs is necessary for metastatic tumour progression. Thus, a genetic approach using a non-amputation/resection model can serve to resolve the controversy surrounding the function of VEGFR1 in mediating metastasis. We hope that the field of metastatic initiation continues to move forward, given its profound impact in the clinical setting. Moreover, anti-PlGF/VEGFR1 agents may provide novel means to block micrometastasis in an adjuvant setting and inhibit metastatic progression.
References
Kaplan, R. N. et al. VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 438, 820–827 (2005)
Dawson, M. R., Duda, D. G., Fukumura, D. & Jain, R. K. VEGFR1-activity-independent metastasis formation. Nature 461 10.1038/nature08254 (2009)
Hiratsuka, S. et al. MMP9 induction by vascular endothelial growth factor receptor-1 is involved in lung-specific metastasis. Cancer Cell 2, 289–300 (2002)
Marcellini, M. et al. Increased melanoma growth and metastasis spreading in mice overexpressing placenta growth factor. Am. J. Pathol. 169, 643–654 (2006)
Taylor, A. P. & Goldenberg, D. M. Role of placenta growth factor in malignancy and evidence that an antagonistic PlGF/Flt-1 peptide inhibits the growth and metastasis of human breast cancer xenografts. Mol. Cancer Ther. 6, 524–531 (2007)
Hiratsuka, S. et al. The S100A8-serum amyloid A3-TLR4 paracrine cascade establishes a premetastatic phase. Nature Cell Biol. 10, 1349–1355 (2008)
Hiratsuka, S., Watanabe, A., Aburatani, H. & Maru, Y. Tumour-mediated upregulation of chemoattractants and recruitment of myeloid cells predetermines lung metastasis. Nature Cell Biol. 8, 1369–1375 (2006)
Erler, J. T. et al. Hypoxia-induced lysyl oxidase is a critical mediator of bone marrow cell recruitment to form the premetastatic niche. Cancer Cell 15, 35–44 (2009)
Kim, S. et al. Carcinoma-produced factors activate myeloid cells through TLR2 to stimulate metastasis. Nature 457, 102–106 (2009)
Fischer, C. et al. Anti-PlGF inhibits growth of VEGF(R)-inhibitor-resistant tumors without affecting healthy vessels. Cell 131, 463–475 (2007)
Shojaei, F. et al. Bv8 regulates myeloid-cell-dependent tumour angiogenesis. Nature 450, 825–831 (2007)
Du, R. et al. HIF1alpha induces the recruitment of bone marrow-derived vascular modulatory cells to regulate tumor angiogenesis and invasion. Cancer Cell 13, 206–220 (2008)
Lin, E. Y. et al. VEGF restores delayed tumor progression in tumors depleted of macrophages. Mol. Oncol. 1, 288–302 (2007)
Luttun, A. et al. Revascularization of ischemic tissues by PlGF treatment, and inhibition of tumor angiogenesis, arthritis and atherosclerosis by anti-Flt1. Nature Med. 8, 831–840 (2002)
Hiratsuka, S., Minowa, O., Kuno, J., Noda, T. & Shibuya, M. Flt-1 lacking the tyrosine kinase domain is sufficient for normal development and angiogenesis in mice. Proc. Natl Acad. Sci. USA 95, 9349–9354 (1998)
Author information
Authors and Affiliations
PowerPoint slides
Rights and permissions
About this article
Cite this article
Kaplan, R., Riba, R., Zacharoulis, S. et al. Kaplan et al. reply. Nature 461, E5 (2009). https://doi.org/10.1038/nature08261
Issue Date:
DOI: https://doi.org/10.1038/nature08261
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
