
Abstract
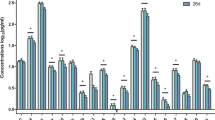
Patients with major depressive disorder (MDD) have clinically relevant, significant decreases in bone mineral density (BMD). We sought to determine if predictive markers of bone inflammation—the osteoprotegerin (OPG)-RANK-RANKL system or osteopontin (OPN)—play a role in the bone abnormalities associated with MDD and, if so, whether ketamine treatment corrected the abnormalities. The OPG-RANK-RANKL system plays the principal role in determining the balance between bone resorption and bone formation. RANKL is the osteoclast differentiating factor and diminishes BMD. OPG is a decoy receptor for RANKL, thereby increasing BMD. OPN is the bone glue that acts as a scaffold between bone tissues matrix composition to bind them together and is an important component of bone strength and fracture resistance. Twenty-eight medication-free inpatients with treatment-resistant MDD and 16 healthy controls (HCs) participated in the study. Peripheral bone marker levels and their responses to IV ketamine infusion in MDD patients and HCs were measured at four time points: at baseline, and post-infusion at 230 min, Day 1, and Day 3. Patients with MDD had significant decreases in baseline OPG/RANKL ratio and in plasma OPN levels. Ketamine significantly increased both the OPG/RANKL ratio and plasma OPN levels, and significantly decreased RANKL levels. Bone marker levels in HCs remained unaltered. We conclude that the OPG-RANK-RANKL system and the OPN system play important roles in the serious bone abnormalities associated with MDD. These data suggest that, in addition to its antidepressant effects, ketamine also has a salutary effect on a major medical complication of depressive illness.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others
References
Michelson D, Stratakis C, Hill L, Reynolds J, Galliven E, Chrousos G et al. Bone mineral density in women with depression. N Engl J Med 1996; 335: 1176–1181.
Altindag O, Altindag A, Asoglu M, Gunes M, Soran N, Deveci Z. Relation of cortisol levels and bone mineral density among premenopausal women with major depression. Int J Clin Pract 2007; 61: 416–420.
Cizza G, Mistry S, Nguyen VT, Eskandari F, Martinez P, Torvik S et al. Do premenopausal women with major depression have low bone mineral density? A 36-month prospective study. PLoS One 2012; 7: e40894.
Cizza G, Ronsaville DS, Kleitz H, Eskandari F, Mistry S, Torvik S et al. Clinical subtypes of depression are associated with specific metabolic parameters and circadian endocrine profiles in women: the power study. PLoS One 2012; 7: e28912.
Coelho R, Silva C, Maia A, Prata J, Barros H. Bone mineral density and depression: a community study in women. J Psychosom Res 1999; 46: 29–35.
Diem SJ, Harrison SL, Haney E, Cauley JA, Stone KL, Orwoll E et al. Depressive symptoms and rates of bone loss at the hip in older men. Osteoporos Int 2013; 24: 111–119.
Eskandari F, Martinez PE, Torvik S, Phillips TM, Sternberg EM, Mistry S et al. Low bone mass in premenopausal women with depression. Arch Intern Med 2007; 167: 2329–2336.
Furlan PM, Ten Have T, Cary M, Zemel B, Wehrli F, Katz IR et al. The role of stress-induced cortisol in the relationship between depression and decreased bone mineral density. Biol Psychiatry 2005; 57: 911–917.
Hsiao MC, Liu CY, Wang CJ. Factors associated with low bone density among women with major depressive disorder. Int J Psychiatry Med 2012; 44: 77–90.
Jacka FN, Pasco JA, Henry MJ, Kotowicz MA, Dodd S, Nicholson GC et al. Depression and bone mineral density in a community sample of perimenopausal women: Geelong Osteoporosis Study. Menopause 2005; 12: 88–91.
Kurmanji JM, Sulaiman SA, Kah LK, Chandrasekaran PK. Depression and low bone mineral density: The correlation among Chinese. Asian J Psychiatr 2010; 3: 134–137.
Laudisio A, Marzetti E, Cocchi A, Bernabei R, Zuccala G. Association of depressive symptoms with bone mineral density in older men: a population-based study. Int J Geriatr Psychiatry 2008; 23: 1119–1126.
Mussolino ME, Jonas BS, Looker AC. Depression and bone mineral density in young adults: results from NHANES III. Psychosom Med 2004; 66: 533–537.
Oh SM, Kim HC, Ahn SV, Rhee Y, Suh I. Association between depression and bone mineral density in community-dwelling older men and women in Korea. Maturitas 2012; 71: 142–146.
Petronijevic M, Petronijevic N, Ivkovic M, Stefanovic D, Radonjic N, Glisic B et al. Low bone mineral density and high bone metabolism turnover in premenopausal women with unipolar depression. Bone 2008; 42: 582–590.
Robbins J, Hirsch C, Whitmer R, Cauley J, Harris T. The association of bone mineral density and depression in an older population. J Am Geriatr Soc 2001; 49: 732–736.
Schweiger U, Deuschle M, Korner A, Lammers CH, Schmider J, Gotthardt U et al. Low lumbar bone mineral density in patients with major depression. Am J Psychiatry 1994; 151: 1691–1693.
Schweiger U, Weber B, Deuschle M, Heuser I. Lumbar bone mineral density in patients with major depression: evidence of increased bone loss at follow-up. Am J Psychiatry 2000; 157: 118–120.
Spangler L, Scholes D, Brunner RL, Robbins J, Reed SD, Newton KM et al. Depressive symptoms, bone loss, and fractures in postmenopausal women. J Gen Intern Med 2008; 23: 567–574.
Whooley MA, Kip KE, Cauley JA, Ensrud KE, Nevitt MC, Browner WS. Depression, falls, and risk of fracture in older women. Study of Osteoporotic Fractures Research Group. Arch Intern Med 1999; 159: 484–490.
Williams LJ, Bjerkeset O, Langhammer A, Berk M, Pasco JA, Henry MJ et al. The association between depressive and anxiety symptoms and bone mineral density in the general population: the HUNT Study. J Affect Disord 2011; 131: 164–171.
Wong SY, Lau EM, Lynn H, Leung PC, Woo J, Cummings SR et al. Depression and bone mineral density: is there a relationship in elderly Asian men? Results from Mr. Os (Hong Kong). Osteoporos Int 2005; 16: 610–615.
Yazici KM, Akinci A, Sutcu A, Ozcakar L. Bone mineral density in premenopausal women with major depressive disorder. Psychiatry Res 2003; 117: 271–275.
Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry 2009; 65: 732–741.
Seibel MJ. Biochemical markers of bone turnover:part I: biochemistry and variability. Clin Biochem Rev 2005; 26: 97–122.
Seibel MJ. Biochemical markers of bone turnover part II: clinical applications in the management of osteoporosis. Clin Biochem Rev 2006; 27: 123–138.
Raisz LG. Physiology and pathophysiology of bone remodeling. Clin Chem 1999; 45: 1353–1358.
Boyce BF, Xing L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res Ther 2007; 9: S1.
Boyce BF, Xing L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch Biochem Biophys 2008; 473: 139–146.
Giuliani N, Colla S, Morandi F, Rizzoli V. The RANK/RANK ligand system is involved in interleukin-6 and interleukin-11 up-regulation by human myeloma cells in the bone marrow microenvironment. Haematologica 2004; 89: 1118–1123.
Bucay N, Sarosi I, Dunstan CR, Morony S, Tarpley J, Capparelli C et al. osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Dev 1998; 12: 1260–1268.
Tyrovola JB. The 'mechanostat' principle and the osteoprotegerin -OPG/RANKL/RANK system PART II. the role of the hypothalamic - pituitary axis. J Cell Biochem 2016; 118: 962–966.
Lacey DL, Boyle WJ, Simonet WS, Kostenuik PJ, Dougall WC, Sullivan JK et al. Bench to bedside: elucidation of the OPG-RANK-RANKL pathway and the development of denosumab. Nat Rev Drug Discov 2012; 11: 401–419.
Liu JZ, Ji ZL, Chen SM. The OPG/RANKL/RANK system and bone resorptive disease. Sheng Wu Gong Cheng Xue Bao 2003; 19: 655–660.
Tyrovola JB. The "mechanostat theory" of frost and the OPG/RANKL/RANK System. J Cell Biochem 2015; 116: 2724–2729.
Butler WT. The nature and significance of osteopontin. Connect Tissue Res 1989; 23: 123–136.
McKee MD, Nanci A. Osteopontin deposition in remodeling bone: an osteoblast mediated event. J Bone Miner Res 1996; 11: 873–875.
Pagel CN, Wasgewatte Wijesinghe DK, Taghavi Esfandouni N, Mackie EJ. Osteopontin, inflammation and myogenesis: influencing regeneration, fibrosis and size of skeletal muscle. J Cell Commun Signal 2014; 8: 95–103.
Thurner PJ, Chen CG, Ionova-Martin S, Sun L, Harman A, Porter A et al. Osteopontin deficiency increases bone fragility but preserves bone mass. Bone 2010; 46: 1564–1573.
Sodek J, Ganss B, McKee MD. Osteopontin. Crit Rev Oral Biol Med 2000; 11: 279–303.
Hoang QQ, Sicheri F, Howard AJ, Yang DS. Bone recognition mechanism of porcine osteocalcin from crystal structure. Nature 2003; 425: 977–980.
Grassi-Oliveira R, Brieztke E, Teixeira A, Pezzi JC, Zanini M, Lopes RP et al. Peripheral chemokine levels in women with recurrent major depression with suicidal ideation. Rev Bras Psiquiatr 2012; 34: 71–75.
Wesseling-Perry K. FGF-23 in bone biology. Pediatr Nephrol 2010; 25: 603–608.
DiazGranados N, Ibrahim LA, Brutsche NE, Ameli R, Henter ID, Luckenbaugh DA et al. Rapid resolution of suicidal ideation after a single infusion of an N-methyl-D-aspartate antagonist in patients with treatment-resistant major depressive disorder. J Clin Psychiatry 2010; 71: 1605–1611.
Zarate CA Jr., Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry 2006; 63: 856–864.
Sackeim HA. The definition and meaning of treatment-resistant depression. J Clin Psychiatry 2001; 62: 10–17.
First MB, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSM-IV TR Axis I Disorders, Research Version, Patient Edition. New York State Psychiatric Institute, Biometrics Research: New York, NY, USA, 2001.
Machado-Vieira R, Yuan P, Brutsche N, DiazGranados N, Luckenbaugh D, Manji HK et al. Brain-derived neurotrophic factor and initial antidepressant response to an N-methyl-D-aspartate antagonist. J Clin Psychiatry 2009; 70: 1662–1666.
Yoshimura R, Hori H, Ikenouchi-Sugita A, Umene-Nakano W, Ueda N, Nakamura J. Higher plasma interleukin-6 (IL-6) level is associated with SSRI- or SNRI-refractory depression. Prog Neuropsychopharmacol Biol Psychiatry 2009; 33: 722–726.
Lotrich FE. Inflammatory cytokine-associated depression. Brain Res 2015; 1617: 113–125.
Hughes AE, Ralston SH, Marken J, Bell C, MacPherson H, Wallace RG et al. Mutations in TNFRSF11A, affecting the signal peptide of RANK, cause familial expansile osteolysis. Nat Genet 2000; 24: 45–48.
Axmann R, Bohm C, Kronke G, Zwerina J, Smolen J, Schett G. Inhibition of interleukin-6 receptor directly blocks osteoclast formation in vitro and in vivo. Arthritis Rheum 2009; 60: 2747–2756.
Weitzmann MN. The role of inflammatory cytokines, the RANKL/OPG axis, and the immunoskeletal interface in physiological bone turnover and osteoporosis. Scientifica 2013; 2013: 125705.
Kwan Tat S, Padrines M, Theoleyre S, Heymann D, IL-6 FortunY, RANKL. TNF-alpha/IL-1: interrelations in bone resorption pathophysiology. Cytokine Growth Factor Rev 2004; 15: 49–60.
Stein B, Yang MX. Repression of the interleukin-6 promoter by estrogen receptor is mediated by NF-kappa B and C/EBP beta. Mol Cell Biol 1995; 15: 4971–4979.
Alesci S, Martinez PE, Kelkar S, Ilias I, Ronsaville DS, Listwak SJ et al. Major depression is associated with significant diurnal elevations in plasma interleukin-6 levels, a shift of its circadian rhythm, and loss of physiological complexity in its secretion: clinical implications. J Clin Endocrinol Metab 2005; 90: 2522–2530.
van'tHof RJ, Ralston SH. Nitric oxide and bone. Immunology 2001; 103: 255–261.
Li CY, Chou TC, Wong CS, Ho ST, Wu CC, Yen MH et al. Ketamine inhibits nitric oxide synthase in lipopolysaccharide-treated rat alveolar macrophages. Can J Anaesth 1997; 44: 989–995.
Lin SZ, Chiou AL, Wang Y. Ketamine antagonizes nitric oxide release from cerebral cortex after middle cerebral artery ligation in rats. Stroke 1996; 27: 747–752.
Rahnert J, Fan X, Case N, Murphy TC, Grassi F, Sen B et al. The role of nitric oxide in the mechanical repression of RANKL in bone stromal cells. Bone 2008; 43: 48–54.
Calarge CA, Burns TL, Schlechte JA, Zemel BS. Longitudinal examination of the skeletal effects of selective serotonin reuptake inhibitors and risperidone in boys. J Clin Psychiatry 2015; 76: 607–613.
Diem SJ, Blackwell TL, Stone KL, Yaffe K, Haney EM, Bliziotes MM et al. Use of antidepressants and rates of hip bone loss in older women: the study of osteoporotic fractures. Arch Intern Med 2007; 167: 1240–1245.
Ortuno MJ, Robinson ST, Subramanyam P, Paone R, Huang YY, Guo XE et al. Serotonin-reuptake inhibitors act centrally to cause bone loss in mice by counteracting a local anti-resorptive effect. Nat Med 2016; 22: 1170–1179.
Yirmiya R, Goshen I, Bajayo A, Kreisel T, Feldman S, Tam J et al. Depression induces bone loss through stimulation of the sympathetic nervous system. Proc Natl Acad Sci USA 2006; 103: 16876–16881.
Hodge JM, Wang Y, Berk M, Collier FM, Fernandes TJ, Constable MJ et al. Selective serotonin reuptake inhibitors inhibit human osteoclast and osteoblast formation and function. Biol Psychiatry 2013; 74: 32–39.
Warden SJ, Nelson IR, Fuchs RK, Bliziotes MM, Turner CH. Serotonin (5-hydroxytryptamine) transporter inhibition causes bone loss in adult mice independently of estrogen deficiency. Menopause 2008; 15: 1176–1183.
Sansone RA, Sansone LA. SSRIs: bad to the bone? Innov Clin Neurosci 2012; 9: 42–47.
Bliziotes MM, Eshleman AJ, Zhang XW, Wiren KM. Neurotransmitter action in osteoblasts: expression of a functional system for serotonin receptor activation and reuptake. Bone 2001; 29: 477–486.
Kerbage H, Bahadori S, Leger J, Carel JC, Purper Ouakil D. Effect of SSRIs on bone metabolism. Encephale 2014; 40: 56–61.
Warden SJ, Robling AG, Sanders MS, Bliziotes MM, Turner CH. Inhibition of the serotonin (5-hydroxytryptamine) transporter reduces bone accrual during growth. Endocrinology 2005; 146: 685–693.
Mion G, Villevieille T. Ketamine pharmacology: an update (pharmacodynamics and molecular aspects, recent findings). CNS Neurosci Ther 2013; 19: 370–380.
Can A, Zanos P, Moaddel R, Kang HJ, Dossou KS, Wainer IW et al. Effects of ketamine and ketamine metabolites on evoked striatal dopamine release, dopamine receptors, and monoamine transporters. J Pharmacol Exp Ther 2016; 359: 159–170.
Tanaka R, Kumagai Y. Pharmacokinetics of anti-RANKL antibody drugs: Denosumab. Clin Calcium 2016; 26: 1597–1603.
Varenna M, Gatti D. The role of rank-ligand inhibition in the treatment of postmenopausal osteoporosis. Reumatismo 2010; 62: 163–171.
Cummings SR, San Martin J, McClung MR, Siris ES, Eastell R, Reid IR et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 2009; 361: 756–765.
Simon JA, Recknor C, Moffett AH Jr., Adachi JD, Franek E, Lewiecki EM et al. Impact of denosumab on the peripheral skeleton of postmenopausal women with osteoporosis: bone density, mass, and strength of the radius, and wrist fracture. Menopause 2013; 20: 130–137.
Torring O. Denosumab efficient against osteoporosis. a biological drug gives new possibilities to treat a public disease. Lakartidningen 2010; 107: 574–575.
Boonen S, Adachi JD, Man Z, Cummings SR, Lippuner K, Torring O et al. Treatment with denosumab reduces the incidence of new vertebral and hip fractures in postmenopausal women at high risk. J Clin Endocrinol Metab 2011; 96: 1727–1736.
Dempster DW, Lambing CL, Kostenuik PJ, Grauer A. Role of RANK ligand and denosumab, a targeted RANK ligand inhibitor, in bone health and osteoporosis: a review of preclinical and clinical data. Clin Ther 2012; 34: 521–536.
Ferrari S, Adachi JD, Lippuner K, Zapalowski C, Miller PD, Reginster JY et al. Further reductions in nonvertebral fracture rate with long-term denosumab treatment in the FREEDOM open-label extension and influence of hip bone mineral density after 3 years. Osteoporos Int 2015; 26: 2763–2771.
Acknowledgments
Funding for this work was supported by the Intramural Research Program at the National Institute of Mental Health, National Institutes of Health (IRP-NIMH-NIH; ZIA MH002927), by a NARSAD Independent Investigator Award to CAZ, and by a Brain and Behavior Mood Disorders Research Award to CAZ. We thank the 7SE research unit and staff for their support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
CAZ is listed as a co-inventor on a patent for the use of ketamine in major depression and suicidal ideation (2 R,6 R)-hydroxynorketamine, (S)-dehydronorketamine, and other stereoisomeric dehydro and hydroxylated metabolites of (R,S)-ketamine metabolites in the treatment of depression and neuropathic pain. CAZ is listed as co-inventor on a patent application for the use of (2 R,6 R)-hydroxynorketamine and (2 S,6 S)-hydroxynorketamine in the treatment of depression, anxiety, anhedonia, suicidal ideation and post-traumatic stress disorders; he has assigned his patent rights to the US. government but will share a percentage of any royalties that may be received by the government. The remaining authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Kadriu, B., Gold, P.W., Luckenbaugh, D.A. et al. Acute ketamine administration corrects abnormal inflammatory bone markers in major depressive disorder. Mol Psychiatry 23, 1626–1631 (2018). https://doi.org/10.1038/mp.2017.109
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/mp.2017.109
This article is cited by
-
Sex differences in the effects of repeated ketamine infusions on bone markers in patients with unipolar and bipolar depression
Biology of Sex Differences (2024)
-
The effects of ketamine and classic hallucinogens on neurotrophic and inflammatory markers in unipolar treatment-resistant depression: a systematic review of clinical trials
European Archives of Psychiatry and Clinical Neuroscience (2023)
-
Molecular mechanisms underlying the antidepressant actions of arketamine: beyond the NMDA receptor
Molecular Psychiatry (2022)
-
Osthole enhances the bone mass of senile osteoporosis and stimulates the expression of osteoprotegerin by activating β-catenin signaling
Stem Cell Research & Therapy (2021)
-
The kynurenine pathway and bipolar disorder: intersection of the monoaminergic and glutamatergic systems and immune response
Molecular Psychiatry (2021)
