
Abstract
There is intense interest in identifying modifiable risk factors associated with autism-spectrum disorders (ASD). Autism-related traits, which can be assessed in a continuous fashion, share risk factors with ASD, and thus can serve as informative phenotypes in population-based cohort studies. Based on the growing body of research linking gestational vitamin D deficiency with altered brain development, this common exposure is a candidate modifiable risk factor for ASD and autism-related traits. The association between gestational vitamin D deficiency and a continuous measure of autism-related traits at ~6 years (Social Responsiveness Scale; SRS) was determined in a large population-based cohort of mothers and their children (n=4229). 25-hydroxyvitamin D (25OHD) was assessed from maternal mid-gestation sera and from neonatal sera (collected from cord blood). Vitamin D deficiency was defined as 25OHD concentrations less than 25 nmol l−1. Compared with the 25OHD sufficient group (25OHD>50 nmol l−1), those who were 25OHD deficient had significantly higher (more abnormal) SRS scores (mid-gestation n=2866, β=0.06, P<0.001; cord blood n=1712, β=0.03, P=0.01). The findings persisted (a) when we restricted the models to offspring with European ancestry, (b) when we adjusted for sample structure using genetic data, (c) when 25OHD was entered as a continuous measure in the models and (d) when we corrected for the effect of season of blood sampling. Gestational vitamin D deficiency was associated with autism-related traits in a large population-based sample. Because gestational vitamin D deficiency is readily preventable with safe, cheap and accessible supplements, this candidate risk factor warrants closer scrutiny.
Similar content being viewed by others

Introduction
Autism-spectrum disorder (ASD) is a neurodevelopmental disorder characterised by repetitive or stereotyped behaviours, and deficits in social relationships.1 Although ASD is a highly heritable disorder, several candidate environmental risk factors have been identified such as prenatal and early life exposures related to infection,2 obstetric complications3, 4 and toxin-related exposures.5 Another potential environmental risk factor for ASD is gestational vitamin D deficiency.6, 7 The vitamin D system is best known for its impact on bone mineral density,8 however optimal concentrations of vitamin D are also required for brain function, via its role in calcium signalling, neurotrophic and neuroprotective actions, as well as its role in neuronal differentiation, maturation and growth.9
There is a growing body of evidence linking gestational vitamin D deficiency with neurodevelopmental disorders such as schizophrenia and ASD.6, 7, 10, 11, 12, 13, 14 Birth cohort studies have provided evidence that gestational vitamin D deficiency (based on prenatal maternal sera) is associated with impairment on a range of cognitive outcomes related to language, motor development and general intelligence.15, 16, 17, 18, 19 With respect to autism-related traits, an Australian birth cohort study (n=406) reported an association between lower mid-gestation 25-hydroxyvitamin D (25OHD) concentrations and higher scores on the Attention Switching subscale of the Autism-Spectrum Quotient.20 Although several studies have assessed vitamin D status in children with ASD,21 and one study has compared neonatal vitamin D status in those with ASD versus their unaffected sibling,22 to the best of our knowledge, no studies have examined the association between gestational vitamin D deficiency and autism or autism-related traits in general population samples.
ASD can be conceptualised as a pronounced and disabling mix of autism-related traits that also exist in a continuum (from mild to severe) in the general population.23, 24 As healthy individuals vary substantially in their capacities for social-emotional interactions and communications, these autism-related traits are thought to follow a normal distribution within the general population. Family studies have shown an increase in autism-related traits in relatives of individuals diagnosed with ASD, suggesting that the same genetic factors affect both ASD and autism-related behaviours.25 Epidemiological studies have suggested a shared aetiology for autism-related traits in the general populations and at the quantitative extremes.26, 27 Recently, Robinson et al.28 have shown that genetic influences on ASD risk also influence typical variation in the population in autism-related traits such as social-emotional interaction and communication ability, suggesting that ASD-related phenotypes can be studied in a quantitative manner.
To this end, we have explored the association between gestational 25OHD concentrations and a widely used parent-report continuous measure of autism-related traits—the Social Responsive Scale (SRS).29 We had the opportunity to do so in a large multi-ethnic population cohort30 where vitamin D concentrations were available at two time points: at mid-gestation (~21 weeks) taken from maternal serum and at birth (from cord blood). In addition, we were able to take into account individual level genome-wide genotype information of the children, in order to reduce the influence of population structure and familial relatedness. We predicted that, compared with those with sufficient concentrations of 25OHD, those who were 25OHD deficient (defined as <25 nmol l−1) at either time point would demonstrate more autism-related traits as indicated by higher SRS scores.
Materials and methods
The cohort
This study was embedded in the Generation R Study, a population-based prospective cohort from fetal life onward, based in Rotterdam, The Netherlands. The design and cohort of Generation R is extensively described elsewhere.31, 32 In brief, the study was designed to identify environmental and genetic correlates of normal and abnormal health-related outcomes in mothers and their children.
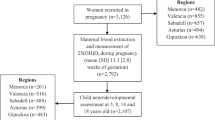
A total of 9778 mothers were enrolled in the study, of these mothers, 8878 (91%) enrolled during pregnancy. Delivery date of the pregnant women was between April 2002 and January 2006. Cohort retention until the age of 6 years, the age of SRS measurement, exceeded 80%. Generation R is a multi-ethnic cohort with the Dutch comprising roughly half of the sample. The ethnic background of the children was defined by the parents’ country of birth, and further classified using definitions from Statistics Netherland.33 If both parents were born abroad, the country of birth of the mother was used to define the child’s ethnicity. The main non-Dutch ethnic groups were Surinamese, Turkish, Moroccan and Cape Verdian, which together accounted for almost 30% of the cohort. Written informed consent was obtained from the mothers, and the study was approved by the institutional review board of the Erasmus Medical Centre.
Vitamin D status
Vitamin D status was assessed by measuring the storage form 25OHD.34 Samples were quantified using isotope dilution liquid chromatography-tandem mass spectrometry. The analytical system consisted of a Shimadzu Nexera UPLC coupled to an AbSciex 5500 QTRAP equipped with an APCI source. Assay accuracy was assessed using certified reference materials purchased from the National Institute of Standards and Technology (NIST SRM 972a Levels 1–4). Further details of the assay methodology can be found in the Supplementary Material (Supplementary Methods 2).
The prevalence and socio-demographic correlates of 25OHD concentrations in the Generation R cohort have been described extensively elsewhere.30 25OHD concentration was defined as the sum of 25-hydroxyvitamin D2 (25OHD2) and 25-hydroxyvitamin D3 (25OHD3) species measured in serum.35 25OHD was measured from prenatal and cord serum in a total of 7935 expecting mothers and their children. The first sample was taken at mid-gestation: “mean (s.d.) gestational age 20.6 (1.2) weeks, range 18.1–24.9 weeks)”. The second sample was collected at birth, from neonatal cord blood: “mean (s.d.) gestational age 40 (1.5) weeks, range 28.4–43.6 weeks)”.
The relationships between 25OHD concentrations and various health-related outcomes can be non-linear.34 Although there is some debate about the definition of deficiency and insufficiency with respect to different health outcomes,36 there is widespread agreement that concentrations lower than 25 nmol l−1 can be defined as deficient (and associated with increased risk of adverse health outcomes).8 In keeping with recommendations for thresholds as defined by the Institute of Medicine,34 we examined three stratified levels of 25OHD concentrations: deficient (<25.0 nmol l−1), insufficient (25–49.9 nmol l−1) and sufficient (50 nmol l−1 or more). We also examined the association between 25OHD concentrations when assessed as a continuous variable. Because the fetus is entirely dependent on the maternal supply of vitamin D, and because of the relatively long half-life of 25OHD (approximately 2 weeks), cord blood assays serve as a proxy measure of late gestational vitamin D status (with deficient cord levels suggesting a vitamin D-deficient environment during late gestation).37, 38 25OHD concentrations in maternal serum collected at delivery and neonatal cord blood are highly correlated (r~0.7).39, 40, 41
Social Responsiveness Scale
The SRS is a rating scale that measures the severity of autism-related traits in the general population.29 For this study, parents of the children filled out an 18-item abridged version of the questionnaire when the children were ~6 years of age (mean age (s.d.)=6.17 (0.48) years; range: 4.89–8.90 years). Parents are asked to rate probes on a 4 point Likert scale; 0 (not true); 1 (sometimes true); 2 (often true); and 3 (almost always true). Prior to analyses, scores of the 18-item SRS were gender-weighted, such that the recommended cutoffs for screening in population-based settings were consistent with weighted scores of 1.078 for boys and 1.000 for girls. The cutoff for the 18-items SRS is based on the cutoff that is suggested by the authors for the full 65 items SRS (that is, weighted by the number of items.)29 The abridged version of the SRS focuses on behavioural features related to social cognition, social communication and autistic mannerisms. Social cognition reflects a child’s ability to interpret social cues (example item ‘Is able to understand the meaning of other people’s tone of voice and facial expressions’). Social communication reflects expressive social communication (example SRS item: ‘Has trouble keeping up with the flow of a normal interaction with other children’; ‘Talks to people with an unusual tone of voice (for example, talks like a robot or like he/she is giving a lecture’). Autistic mannerisms include stereotypical behaviour or highly restricted interests characteristics of autism (example SRS items: ‘Has repetitive odd behaviours such as hand flapping or rocking’; ‘Has more difficulty than other children with changes in his/her routine’). The complete 18-items SRS is provided in the Supplementary Material. Statistical properties of the full SRS have been investigated in a UK population sample of 500 children, aged 5–8 years.42 Construct validity was found to be good when compared with the Repetitive Behaviours Questionnaire 2, and the Strength and Difficulties Questionnaire subscales. Internal consistency was estimated for males and females separately (Cronbach’s α males and females: 0.92). Correlations between the total scores from the full SRS and the abridged version as used in the current study range from 0.93 to 0.99.43, 44 The SRS allows the exploration of autism-related traits as a continuous measure with higher scores indicating greater impairment in the domains of interest.
Ancestry and relatedness derived from observed common genetic variants
Classifications related to ethnicity are often imprecise and contestable.45 Within the Generation R sample there is substantial ‘sample structure’ resulting from both geographic population stratification (that is, inclusion of individuals from different populations) as well as from known and hidden family-relatedness (for example, siblings, cousins and so on). We have previously shown that (a) ethnicity is strongly associated with vitamin D status,30 and (b) ethnicity is strongly (but imperfectly) associated with principal components derived from common single-nucleotide polymorphisms.46 Principal components are often included as covariates in statistical models in order to adjust for ethnic differences; however these do not capture all features of the underlying sample structure. Inadequate adjustment for sample structure may lead to inflation of test statistics and possibly spurious associations between the variables of interest. Recent developments in statistical genetics have utilised genome-wide genotype data to better model the effects of sample structure on a phenotype.47 Within the Generation R Cohort, genome-wide genotype data are available for the children, thus utilising these data allows us to reduce the imprecision of the important confounding ethnicity variable. DNA was extracted from blood collected from the umbilical cord, or if this was not available, from a blood sample that was obtained by venepuncture during the child’s visit to the research centre at a mean age of 6 years. A detailed description of the genotyping of the Generation R cohort is described elsewhere.46, 48 and details about genotyping and Quality Control that are relevant to this study are provided in the Supplementary Material. Analyses involving genome-wide genotype data in the current study were based on 3234 individuals on 518 245 single-nucleotide polymorphisms.
Statistical analyses
The sample sizes for different analyses vary between analyses related to the availability of mid-gestational and cord 25OHD concentrations, SRS at age 6 years, offspring genotype information and ethnicity. Note that twin pregnancies and mothers with no follow-up after birth were removed prior to analyses (see Supplementary Material Figure).
In order to optimise the sample size, we imputed a range of parental and offspring variables that were included as covariates in the models.49 Imputation was performed using the ‘Mix’ imputation package in R.50 ‘Mix’ uses an iterative multiple regression algorithm, which is Expectation–Maximisation based and imputes mixed continuous and categorical data under the general location model. Imputation expectancies were based on covariates only and were independent of predictor variables (25OHD concentrations) and outcome variable (SRS). Four out of eight variables had missing data with missing proportions ranging from 3% (‘Educational level of the mother’) to 10% (‘Mother smoking during pregnancy’).
Main analyses
Within a linear model framework, we first compared SRS scores between those with (a) deficient versus sufficient and (b) insufficient versus sufficient concentrations of vitamin D, for both mid-gestation and cord blood. Parental and offspring variables were included as covariates in the model. Second, we compared SRS scores between those who were deficient at two time points (mid-gestation and cord blood) and those that were not deficient at either time point and we compared SRS scores between those that were deficient at one time point (mid-gestation or cord blood) and those that were not deficient at either time point. Third, we tested the association between continuous measures of vitamin D and SRS. In addition, we tested whether vitamin D deficiency was predictive of SRS when SRS was treated as a dichotomous outcome. In this analysis, the outcome variable was high-SRS for those children with SRS scores above the suggested gender-weighted cutoff and low-SRS for those with scores below the cutoff.
Sensitivity and responder analyses
In addition to the main analyses, we undertook three planned sensitivity analyses. First, we analysed only offspring with European ethnic background. Second, we replaced the ethnicity variable with a genetic component that captures both population stratification and family-relatedness and allows a test for association that is free from confounding owing to sample structure. In this setting, we do not want to adjust the analyses based on any particular single-nucleotide polymorphism, but for an overall, genome-wide degree of relatedness. Third, we adjusted the models for season of blood sampling to (a) correct for within-year fluctuations in 25OHD concentrations and (b) to reduce the influence of other (unobserved) seasonally fluctuating exposures. A detailed description of the models is provided in the Supplementary Material, including both a simplified ‘worked example’ and a detailed technical description of the Genetic Relationship Matrix approach for dealing with sample structure. In our prospective population cohort we have missingness on socio-demographic variables, blood samples and SRS. We compared SRS responders versus non-responders in order to explore the impact of attrition/missingness on key socio-demographic variables.
Results
Supplementary Figure 1 depicts a flow chart of the inclusion of participants in this study. In total, 4229 children and their mothers were available with measures of vitamin D concentrations drawn from maternal blood at mid-gestation and/or drawn from cord blood at time of birth as well as data on the SRS, 2489 children and their mothers were available with measures of vitamin D concentrations at both time points. Of the 4229 children in our sample, 3169 of the children had individual level genotype data available. Table 1 provides an overview of the distributions of parental and offspring demographic variables in the study sample. Supplementary Table 1 provides details of the distributions of the demographic variables before and after imputation.
Table 2 summarises the prevalence of 25OHD deficiency in mid-gestation and cord blood for those samples for which SRS scores were available. The proportion of the sample with deficiency was substantial: 16% for maternal serum at mid-gestation and 36% for cord blood. On average, 25OHD concentrations from cord blood were lower compared with concentrations at mid-gestation (mean 25OHD concentration in maternal serum at mid-gestation: 58.9 nmol l−1; mean 25OHD concentration in cord blood: 35.9 nmol l−1; t=35.8, P<001).
Vitamin D and SRS scores
Scores on the SRS were available for 4229 children. The data were right skewed and in order to improve the distribution of the outcome variable, values for the SRS were ‘winsorized’ (that is, extreme outlier scores were recoded to improve distribution). Scores higher than 1.5 (corresponding with ~5 s.d.s above the mean, n=21 children) were set to equal 1.5. Supplementary Figure 2 depicts the distributions of the raw SRS scores and the gender-weighted and winsorized SRS scores. Mean gender-weighted scores (s.d., range) of the SRS was 0.23 units (0.23, 0–1.5) and median (interquartile range) of 0.17 (0.06, 0.29). Mean SRS (s.d.) for individuals vitamin D deficient, insufficient and sufficient at mid-gestation was: 0.32 (0.28), 0.24 (0.24) and 0.20 (0.20), respectively. Mean SRS (s.d.) for individuals vitamin D deficient, insufficient and sufficient based on cord blood was: 0.27 (0.25), 0.21 (0.22) and 0.19 (0.20), respectively. Supplementary Table 3 also provides an overview of the SRS scores for different vitamin D deficiency categories.
Table 3 shows the results of the main analyses for the SRS (including ethnicity as a covariate). In all analyses, 25OHD deficiency or lower 25OHD concentrations were associated with higher (more impaired) SRS scores. Compared with those who were sufficient, those who were deficient at mid-gestation or deficient at time of birth were significantly more likely to have higher SRS scores (mid-gestation: β=0.06, s.e.=0.01, P<0.001; cord: β=0.03, s.e.=0.01, P=0.01). Moreover, compared with those who were sufficient at mid-gestation, those who were insufficient were also significantly more likely to have higher SRS scores (β=0.02, s.e.=0.01, P=0.007) (see Table 3A). These results imply that, after correcting for confounding variables (see notes under Table 3), those who were deficient at time of birth had on average 0.06 point higher gender-weighted SRS score, which corresponds to an increase of approximately one fourth of the s.d. (s.d. of the SRS in the total sample=0.23). When treating SRS as a dichotomous outcome, that is, comparing children with SRS scores above the suggested cutoff with children below the suggested cutoff, those who were vitamin D deficient at mid-gestation were 3.8 times more likely to be screened positive than those who were vitamin D sufficient at mid-gestation (see also Supplementary Table 4).
The comparison of SRS scores of those that were deficient at two time points (mid-gestation and cord blood) versus those that were not deficient at either time point showed that being 25OHD deficient at both time points was predictive of higher SRS scores. Having 25OHD deficiency at only one time point (mid-gestation or cord blood) did not predict SRS scores (Table 3B). When we treated 25OHD concentrations as continuous variables we observed a significant increase in SRS scores with decreasing concentrations of 25OHD for both mid-gestation and cord samples, that is, a similar pattern as observed in the association between vitamin D deficiency categories and SRS (Table 3C).
Sensitivity and responder analyses
In the analyses restricted to offspring with European ethnicity, we found that the pattern of findings persisted with significant increase in SRS scores for those deficient versus sufficient (both Midgestion and Cord) and for those insufficient vs sufficient (mid-gestation) (Supplementary Table 5). Similarly, when we replaced ethnicity with the genetic component that captures both population stratification and family-relatedness, the pattern of findings identified in the main analyses persisted, suggesting that the observed association was free from confounding with ethnicity (Supplementary Table 6). The results persisted after adjusting the models for season of blood sampling (that is, season at mid-gestation or at time of birth for respective analyses). Results shown in Supplementary Table 7. Those who dropped out, or had missing data for the predictor and/or outcome variable, were more likely to have the follow characteristics; (a) non-European, (b) less well educated, (c) smoked during the pregnancy, (c) younger parental age and (d) shorter gestational age. There was no significant difference in the gender of the child (Supplementary Table 8).
Discussion
In our population-based cohort study sample of 4229 children, we show that gestational vitamin D deficiency was associated with higher scores on the SRS. We report for we believe the first time an association between mid-gestational 25OHD deficiency and variation in a widely used, continuous measure of autism-related traits in the general population. The pattern of findings persisted when we restricted the analyses to the offspring of European ethnicity and when we accounted for sample structure using individual level genetic data of the offspring. These analyses strongly reduce the chance that our main analyses were confounded by ethnic diversity within the sample.
When we examined the two time-point measures of vitamin D deficiency we found only mother–infant pairs with deficiency at both time points had higher scores on the SRS. This finding suggests that infants exposed to persistent low vitamin D from mid-gestation until birth may be at risk for autism-related traits, whereas this was not identified in those with deficiency at only one time point. In light of the (a) significant relationship between 25OHD when assessed as a continuous variable versus SRS, and (b) the significant relationship between both mid-gestation deficient and insufficient 25OHD concentration versus SRS, we speculate that the exposure may operate as a continuous graded risk factor, without a critical threshold. Our study, based on a large, population-based, multi-ethnic cohort, was well suited to test our hypotheses. The prevalence of vitamin D deficiency was high (16% of the mothers had mid-gestational 25OHD concentrations <25 nmol l−1; based on cord blood, the prevalence of vitamin D deficiency was 36%).
Vitamin D is a fat-soluble vitamin that, in humans, is obtained from exposure to sunlight and, to a lesser extent, from diet.8 The active form of vitamin D (1,25 dihydroxyvitamin D) binds to the vitamin D receptor, which is a member of a phylogenetically conserved superfamily of nuclear receptors. Several other ligands operating via nuclear receptors are known to be important in brain development (for example, retinoic acid, glucocorticoids, thyroid hormone, sex hormones). Both the vitamin D receptor and the rate-limiting enzyme required for the production of 1,25 dihydroxyvitamin D, are expressed in neurons and glial cells in the brain.51 The findings from the current study lends weight to the growing body of research linking gestational vitamin D deficiency and altered brain development. Rodent models based on transient prenatal exposure to vitamin D deficiency have found a range of persistent molecular (gene and protein expression), neurochemical and behavioural changes of interest to neuropsychiatry.52 Neonatal vitamin D deficiency has been previously associated with an increased risk of schizophrenia,53 and ASD and schizophrenia are known to share genetic risk variants.54 Our findings provide additional evidence of the shared risk architecture between these two neurodevelopmental disorders. These convergent clues may provide insights into the etiopathogenesis of neurodevelopmental disorders. For example, the active form of vitamin D (1,25 dihydoxyvitamin D) is known to impact on the function of voltage-gated calcium channels.55, 56 Variants in genes coding for subunits of these same calcium channels (for example, CACNA1C) have been linked to risk of both schizophrenia and ASD.57, 58 In addition, vitamin D has been linked to other neurobiological features associated with autism.14, 59 For example, 1,25 dihydoxyvitamin D has been shown to influence the expression of tryptophan hydroxylase 2 (a key enzyme in the production of serotonin).60 Mice exposed to adult vitamin D-deficient diets had altered behaviour (that is, hyperlocomotion in a novel open field) and a significant reduction in the key enzyme involved in the key synthesising enzymes for GABA, glutamic acid decarboxylase type 65 and 67 (GAD65, GAD67).61 Reductions in the expression of GAD65/67 has been previously reported in post-mortem studies of ASD.62, 63
With respect to study limitations, although we had measures of 25OHD concentrations at two developmental time points, we lacked information at other stages of gestation and early life. Defining the precise critical window during which developmental vitamin D deficiency adversely impacts on brain development would be premature. Differential attrition is known to impact on the representativeness of modern birth cohorts. Several of the variables associated with non-responder status in our study are associated with either low vitamin D (for example, non-European ethnicity, smoking),30 and/or risk of autism-related outcomes (for example, lower gestational age).64 In the presence of a true association between gestational vitamin D deficiency and higher SRS scores, this differential pattern of nonresponse would bias the sample toward the null hypothesis (it is therefore unlikely that the observed responder bias could account for our significant findings). It should also be noted that we do not believe that low gestational 25OHD concentration is solely linked to higher scores on the SRS (that is, specificity between the exposure and the outcome). There is evidence linking low prenatal vitamin D status with increased risk of other neurodevelopmental disorders such as schizophrenia13 and attention deficit and hyperactivity disorder.65 Although the SRS is well suited to assess autism-related traits, poor communication can also be associated with a range of other childhood disorders.66, 67 Findings based on observational epidemiology are susceptible to residual confounding and it is feasible that vitamin D status could serve as a proxy marker for other (unobserved) risk-modifying factors linked to SRS scores. Randomised controlled trials of vitamin D supplementation during pregnancy will be needed in order to confidently link vitamin D and an increased risk of autism-related conditions. In light of the evidence linking prenatal vitamin D with general growth and bone health68, 69, 70 such trials should be designed with several primary outcomes. In our data, we observe a more pronounced association for those who were deficient at two time points (that is, mid-gestation and at time of birth) compared with deficiency at only one time point. We also detected an association between the continuous measure of vitamin D concentrations and autism-related traits, letting us hypothesise that vitamin D is operating as a continuous grade risk factor without a critical threshold. Randomised controlled trials will be required to test this hypothesis.
Future research should focus on specificity of the effect of early life vitamin D deficiency in relation to neurodevelopmental disorders. Alongside animal studies that aim to elucidate the biological mechanisms linking vitamin D deficiency and brain development, human studies could focus on endophenotypes to better understand the pathway from vitamin D deficiency to various neurodevelopmental disorders (for example, structural and functional magnetic resonance imaging44, 71).
This study has several important strengths. Our sample was based on a large representative multi-ethnic cohort. We used a gold standard assessment of 25OHD concentrations, and a widely used measure of autism-related traits. We had access to infant genotypes and were able to explore innovative models that can more precisely adjust for ancestral differences and family-relatedness in the cohort.
Our findings require replication in independent samples. We are aware of several case–control studies currently underway that will examine the association between neonatal 25OHD and ASD. Ideally, future studies should examine additional time points during gestation, as well as cord/neonatal samples, as it remains to be determined whether gestational and early life vitamin D status has a ‘critical window’ when the brain is differentially sensitive to this exposure.
Conclusions
25OHD deficiency assessed either at mid-gestation or at birth was associated with an increase in autism-related traits in 6-year-old children. The association between developmental vitamin D deficiency and autism-related traits may have important implications from a public health perspective. It is feasible that a safe, cheap and publicly accessible vitamin D supplement in at-risk groups may reduce the prevalence of this risk factor. Just as prenatal folate supplementation has reduced the incidence of spina bifida, we speculate that prenatal vitamin D supplementation may reduce the incidence of ASD.
References
APA APA . Diagnostic and statistical manual of mental disorders: DSM-5 5th edn, American Psychiatric Association: Washington, DC, USA, 2013.
Patterson PH . Immune involvement in schizophrenia and autism: etiology, pathology and animal models. Behav Brain Res 2009; 204: 313–321.
Glasson EJ, Bower C, Petterson B, de Klerk N, Chaney G, Hallmayer JF . Perinatal factors and the development of autism: a population study. Arch Gen Psychiatry 2004; 61: 618–627.
Kolevzon A, Gross R, Reichenberg A . Prenatal and perinatal risk factors for autism: a review and integration of findings. Arch Pediatr Adolesc Med 2007; 161: 326–333.
Lyall K, Schmidt RJ, Hertz-Picciotto I . Maternal lifestyle and environmental risk factors for autism spectrum disorders. Int J Epidemiol 2014; 43: 443–464.
Mazahery H, Camargo CA, Conlon C, Beck KL, Kruger MC, von Hurst PR . Vitamin D and autism spectrum disorder: a literature review. Nutrients 2016; 8: 236.
Cannell JJ . Autism and vitamin D. Med Hypotheses 2008; 70: 750–759.
Holick MF . Vitamin D deficiency. N Engl J Med 2007; 357: 266–281.
Groves NJ, McGrath JJ, Burne THJ . Vitamin D as a neurosteroid affecting the developing and adult brain. Annu Rev Nutr 2014; 34: 117–141.
McGrath JJ, Burne TH, Féron F, Mackay-Sim A, Eyles DW . Developmental vitamin D deficiency and risk of schizophrenia: a 10-year update. Schizophr Bull 2010; 36: 1073–1078.
Deluca GC, Kimball SM, Kolasinski J, Ramagopalan SV, Ebers GC . The role of vitamin D in nervous system health and disease. Neuropathol Appl Neurobiol 2013; 39: 458–484.
Kocovska E, Fernell E, Billstedt E, Minnis H, Gillberg C . Vitamin D and autism: clinical review. Res Dev Disabil 2012; 33: 1541–1550.
McGrath JJ, Burne TH, Feron F, Mackay-Sim A, Eyles DW . Developmental vitamin D deficiency and risk of schizophrenia: a 10-year update. Schizophr Bull 2010; 36: 1073–1078.
Patrick RP, Ames BN . Vitamin D hormone regulates serotonin synthesis. Part 1: relevance for autism. FASEB J 2014; 28: 2398–2413.
Whitehouse AJ, Holt BJ, Serralha M, Holt PG, Kusel MM, Hart PH . Maternal serum vitamin D levels during pregnancy and offspring neurocognitive development. Pediatrics 2012; 129: 485–493.
Morales E, Guxens M, Llop S, Rodriguez-Bernal CL, Tardon A, Riano I et al. Circulating 25-hydroxyvitamin D3 in pregnancy and infant neuropsychological development. Pediatrics 2012; 130: e913–e920.
Hanieh S, Ha TT, Simpson JA, Thuy TT, Khuong NC, Thoang DD et al. Maternal vitamin D status and infant outcomes in rural Vietnam: a prospective cohort study. PLoS One 2014; 9: e99005.
Keim SA, Bodnar LM, Klebanoff MA . Maternal and cord blood 25(OH)-vitamin D concentrations in relation to child development and behaviour. Paediatr Perinat Epidemiol 2014; 28: 434–444.
Tylavsky FA, Kocak M, Murphy LE, Graff JC, Palmer FB, Volgyi E et al. Gestational vitamin 25(OH)D status as a risk factor for receptive language development: a 24-month, longitudinal, observational study. Nutrients 2015; 7: 9918–9930.
Whitehouse AJ, Holt BJ, Serralha M, Holt PG, Hart PH, Kusel MM . Maternal vitamin D levels and the autism phenotype among offspring. J Autism Dev Disord 2013; 43: 1495–1504.
Wang T, Shan L, Du L, Feng J, Xu Z, Staal WG et al. Serum concentration of 25-hydroxyvitamin D in autism spectrum disorder: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry 2016; 25: 341–350.
Fernell E, Bejerot S, Westerlund J, Miniscalco C, Simila H, Eyles D et al. Autism spectrum disorder and low vitamin D at birth: a sibling control study. Mol Autism 2015; 6: 3.
Wing L. The continuum of autistic characteristics. Diagnosis and assessment in autism. Springer US, New York, USA, 1988, pp 91–110.
Baron-Cohen S, Wheelwright S, Skinner R, Martin J, Clubley E . The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord 2001; 31: 5–17.
Constantino JN, Zhang Y, Frazier T, Abbacchi AM, Law P . Sibling recurrence and the genetic epidemiology of autism. Am J Psychiatry 2010; 167: 1349–1356.
Robinson EB, Koenen KC, McCormick MC, Munir K, Hallett V, Happe F et al. Evidence that autistic traits show the same etiology in the general population and at the quantitative extremes (5%, 2.5%, and 1%). Arch Gen Psychiatry 2011; 68: 1113–1121.
Ronald A, Hoekstra RA . Autism spectrum disorders and autistic traits: a decade of new twin studies. Am J Med Genet B Neuropsychiatr Genet 2011; 156B: 255–274.
Robinson EB St, Pourcain B, Anttila V, Kosmicki JA, Bulik-Sullivan B, Grove J et al. Genetic risk for autism spectrum disorders and neuropsychiatric variation in the general population. Nat Genet 2016; 48: 552–555.
Constantino JN, Davis SA, Todd RD, Schindler MK, Gross MM, Brophy SL et al. Validation of a brief quantitative measure of autistic traits: comparison of the social responsiveness scale with the autism diagnostic interview-revised. J Autism Dev Disord 2003; 33: 427–433.
Vinkhuyzen AA, Eyles DW, Burne TH, Blanken LM, Kruithof CJ, Verhulst F et al. Prevalence and predictors of vitamin D deficiency based on maternal mid-gestation and neonatal cord bloods: The Generation R Study. J Steroid Biochem Mol Biol 2015; 164: 161–167.
Jaddoe VW, van Duijn CM, Franco OH, van der Heijden AJ, van Iizendoorn MH, de Jongste JC et al. The Generation R Study: design and cohort update 2012. Eur J Epidemiol 2012 27: 739–756.
Kruithof CJ, Kooijman MN, van Duijn CM, Franco OH, de Jongste JC, Klaver CC et al. The Generation R Study: biobank update 2015. Eur J Epidemiol 2014; 29: 911–927.
Statistiek CBvd Immigrants in the Netherlands 2004. Voorburg: The Netherlands, 2004.
Institute of Medicine (US) Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In: A Catharine Ross, Christine LT, Ann LY, Heather B Del Valle (eds). Dietary Reference Intakes for Calcium and Vitamin D. National Academies Press: Washington DC, USA, 2010.
Eyles D, Anderson C, Ko P, Jones A, Thomas A, Burne T et al. A sensitive LC/MS/MS assay of 250H vitamin D-3 and 250H vitamin D-2 in dried blood spots. Clin Chim Acta 2009; 403: 145–151.
Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011; 96: 1911–1930.
Hillman LS, Haddad JG . Human perinatal vitamin D metabolism. I. 25-Hydroxyvitamin D in maternal and cord blood. J Pediatr 1974; 84: 742–749.
Salle BL, Delvin EE, Lapillonne A, Bishop NJ, Glorieux FH . Perinatal metabolism of vitamin D. Am J Clin Nutr 2000; 71: 1317S–1324S.
Jacquemyn Y, Ajaji M, Karepouan N . Vitamin D levels in maternal serum and umbilical cord blood in a multi-ethnic population in Antwerp, Belgium. Facts Views Vis Obgyn 2013; 5: 3–5.
Vieth Streym S, Kristine Moller U, Rejnmark L, Heickendorff L, Mosekilde L, Vestergaard P . Maternal and infant vitamin D status during the first 9 months of infant life-a cohort study. Eur J Clin Nutr 2013; 67: 1022–1028.
Karras SN, Shah I, Petroczi A, Goulis DG, Bili H, Papadopoulou F et al. An observational study reveals that neonatal vitamin D is primarily determined by maternal contributions: implications of a new assay on the roles of vitamin D forms. Nutr J 2013; 12: 77.
Wigham S, McConachie H, Tandos J, Le Couteur AS . Gateshead Millennium Study core team. The reliability and validity of the Social Responsiveness Scale in a UK general child population. Res Dev Disabil 2012; 33: 944–950.
Roman GC, Ghassabian A, Bongers-Schokking JJ, Jaddoe VW, Hofman A, de Rijke YB et al. Association of gestational maternal hypothyroxinemia and increased autism risk. Ann Neurol 2013; 74: 733–742.
Blanken LM, Mous SE, Ghassabian A, Muetzel RL, Schoemaker NK, El Marroun H et al. Cortical morphology in 6- to 10-year old children with autistic traits: a population-based neuroimaging study. Am J Psychiatry 2015; 172: 479–486.
Yudell M, Roberts D, DeSalle R, Tishkoff S . Taking race out of human genetics. Science 2016; 351: 564–565.
Medina-Gomez C, Felix JF, Estrada K, Peters MJ, Herrera L, Kruithof CJ et al. Challenges in conducting genome-wide association studies in highly admixed multi-ethnic populations: the Generation R Study. Eur J Epidemiol 2015; 30: 317–330.
Kang HM, Sul JH, Service SK, Zaitlen NA, Kong SY, Freimer NB et al. Variance component model to account for sample structure in genome-wide association studies. Nat Genet 2010; 42: 348–354.
Jaddoe VW, Bakker R, van Duijn CM, van der Heijden AJ, Lindemans J, Mackenbach JP et al. The Generation R Study Biobank: a resource for epidemiological studies in children and their parents. Eur J Epidemiol 2007; 22: 917–923.
Newgard CD, Lewis RJ . Accounting for missing data in clinical research—reply. JAMA 2016; 315: 518.
Schafer J. Estimation/multiple imputation for mixed categorical and continuous data. 1.0-9 edn, 2015.
Eyles DW, Smith S, Kinobe R, Hewison M, McGrath JJ . Distribution of the Vitamin D receptor and 1alpha-hydroxylase in human brain. J Chem Neuroanat 2005; 29: 21–30.
Cui X, Gooch H, Groves NJ, Sah P, Burne TH, Eyles DW et al. Vitamin D and the brain: key questions for future research. J Steroid Biochem Mol Biol 2015; 148: 305–309.
McGrath JJ, Eyles DW, Pedersen CB, Anderson C, Ko P, Burne TH et al. Neonatal vitamin D status and risk of schizophrenia: a population-based case-control study. Arch Gen Psychiatry 2010; 67: 889–894.
Lee SH, Ripke S, Neale BM, Faraone SV, Purcell SM, Perlis RH et al. Genetic relationship between five psychiatric disorders estimated from genome-wide SNPs. Nat Genet 2013; 45: 984–994.
Latimer CS, Brewer LD, Searcy JL, Chen KC, Popovic J, Kraner SD et al. Vitamin D prevents cognitive decline and enhances hippocampal synaptic function in aging rats. Proc Natl Acad Sci USA 2014; 111: E4359–E4366.
Cui X, Gooch H, Groves NJ, Sah P, Burne TH, Eyles DW et al. Vitamin D and the brain: key questions for future research. J Steroid Biochem Mol Biol 2015; 148: 305–309.
Bhat S, Dao DT, Terrillion CE, Arad M, Smith RJ, Soldatov NM et al. CACNA1C (Ca(v)1.2) in the pathophysiology of psychiatric disease. Prog Neurobiol 2012; 99: 1–14.
Casamassima F, Hay AC, Benedetti A, Lattanzi L, Cassano GB, Perlis RH . L-type calcium channels and psychiatric disorders: a brief review. Am J Med Genet B Neuropsychiatr Genet 2010; 153B: 1373–1390.
Eyles DW, Burne THJ, McGrath JJ . Vitamin D, effects on brain development, adult brain function and the links between low levels of vitamin D and neuropsychiatric disease. Front Neuroendocrinol 2013; 34: 47–64.
Kaneko I, Sabir MS, Dussik CM, Whitfield GK, Karrys A, Hsieh JC et al. 1,25-Dihydroxyvitamin D regulates expression of the tryptophan hydroxylase 2 and leptin genes: implication for behavioral influences of vitamin D. FASEB J 2015; 29: 4023–4035.
Groves NJ, Kesby JP, Eyles DW, McGrath JJ, Mackay-Sim A, Burne TH . Adult vitamin D deficiency leads to behavioural and brain neurochemical alterations in C57BL/6J and BALB/c mice. Behav Brain Res 2012; 241C: 120–131.
Fatemi SH, Halt AR, Stary JM, Kanodia R, Schulz SC, Realmuto GR . Glutamic acid decarboxylase 65 and 67 kDa proteins are reduced in autistic parietal and cerebellar cortices. Biol Psychiatry 2002; 52: 805–810.
Blatt GJ, Fatemi SH . Alterations in GABAergic biomarkers in the autism brain: research findings and clinical implications. Anat Rec (Hoboken) 2011; 294: 1646–1652.
Atladottir HO, Schendel DE, Henriksen TB, Hjort L, Parner ET . Gestational age and autism spectrum disorder: trends in risk over time. Autism Res 2016; 9: 224–231.
Morales E, Julvez J, Torrent M, Ballester F, Rodriguez-Bernal CL, Andiarena A et al. Vitamin D in pregnancy and attention deficit hyperactivity disorder-like symptoms in childhood. Epidemiology 2015; 26: 458–465.
Hus V, Bishop S, Gotham K, Huerta M, Lord C . Factors influencing scores on the social responsiveness scale. J Child Psychol Psychiatry 2013; 54: 216–224.
Hanratty J, Livingstone N, Robalino S, Terwee CB, Glod M, Oono IP et al. Systematic review of the measurement properties of tools used to measure behaviour problems in young children with autism. PLoS One 2015; 10: e0144649.
Sunyecz JA . The use of calcium and vitamin D in the management of osteoporosis. Ther Clin Risk Manag 2008; 4: 827–836.
Hansen KE, Johnson RE, Chambers KR, Johnson MG, Lemon CC, Vo TN et al. Treatment of vitamin D insufficiency in postmenopausal women: a randomized clinical tTrial. JAMA Intern Med 2015; 175: 1612–1621.
Di Daniele N, Carbonelli MG, Candeloro N, Iacopino L, De Lorenzo A, Andreoli A . Effect of supplementation of calcium and vitamin D on bone mineral density and bone mineral content in peri- and post-menopause women; a double-blind, randomized, controlled trial. Pharmacol Res 2004; 50: 637–641.
van Erp TG, Hibar DP, Rasmussen JM, Glahn DC, Pearlson GD, Andreassen OA et al. Subcortical brain volume abnormalities in 2028 individuals with schizophrenia and 2540 healthy controls via the ENIGMA consortium. Mol Psychiatry 2016; 21: 585.
Acknowledgements
The Generation R Study is made possible by financial support from the Erasmus Medical Centre, Rotterdam, the Erasmus University Rotterdam and the Netherlands Organization for Health Research and Development. Dr Vincent Jaddoe received an additional grant from the Netherlands Organization for Health Research and Development (ZonMw-VIDI 016.136.361) and a Consolidator Grant from the European Research Council (ERC-2014-CoG-648916). The vitamin D assay was supported by the National Health and Medical Research Council (NHMRC APP1062846). Shipping of the samples was supported by FP7 Nutrimenthe (grant agreement 212652). John McGrath received a NHMRC John Cade Fellowship (APP1056929). We thank the participants and staff of the Generation R study. We thank the members of the Centre for Neurogenetics and Statistical Genomics at the Queensland Brain Institute for their support (a list of members of this centre can be found http://cnsgenomics.com/index.html)
Author contributions
Dr Tiemeier has full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analyses. Study concept and design: McGrath, Jaddoe, Tiemeier, Verhulst, Eyles. Acquisition of data: Jaddoe, Tiemeier, Kruithof, Eyles. Analysis and interpretation: Vinkhuyzen, McGrath, Tiemeier, Blanken, Jaddoe. Drafting of the manuscript: McGrath, Vinkhuyzen, Tiemeier, Blanken. Critical review of the manuscript for important intellectual content: McGrath, Vinkhuyzen, Tiemeier, Blanken, Jaddoe, Kruithof, Verhulst, Eyles, Burne. Statistical analyses: Vinkhuyzen, McGrath. Obtained funding: Jaddoe, Tiemeier, McGrath, Burne, Eyles. Administrative, technical, or material support: Kruithof, Blanken. Study supervision: McGrath, Tiemeier.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Molecular Psychiatry website
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Vinkhuyzen, A., Eyles, D., Burne, T. et al. Gestational vitamin D deficiency and autism-related traits: the Generation R Study. Mol Psychiatry 23, 240–246 (2018). https://doi.org/10.1038/mp.2016.213
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/mp.2016.213
This article is cited by
-
Sex differences in placenta-derived markers and later autistic traits in children
Translational Psychiatry (2023)
-
Developmental vitamin D-deficiency produces autism-relevant behaviours and gut-health associated alterations in a rat model
Translational Psychiatry (2023)
-
Genetic correlates of vitamin D-binding protein and 25-hydroxyvitamin D in neonatal dried blood spots
Nature Communications (2023)
-
Evidence based recommendations for an optimal prenatal supplement for women in the US: vitamins and related nutrients
Maternal Health, Neonatology and Perinatology (2022)
-
Maternal vitamin D during pregnancy and offspring autism and autism-associated traits: a prospective cohort study
Molecular Autism (2022)

{kind=link}
{kind=link}