
Abstract
It has been reported that high-risk human papillomavirus (HPV) is a causative agent of a subgroup of oropharyngeal carcinomas. In these tumors, the presence of the transcriptionally active HPV has been proved through the identification of HPV E6 or E7 messenger RNA (mRNA) transcripts. The aim of the study was to assess the HPV-active transcription in a series of sinonasal carcinomas, in correlation with the HPV DNA identification and the p16 immunohistochemistry. Seventy patients with squamous cell carcinomas of the sinonasal tract were included in the survey. The main clinicopathological characteristics were recorded. All tumors were investigated for HPV through the HPV DNA detection by PCR, using the SPF10 primers and by in situ hybridization, using the high-risk GenPoint probe (Dako, Glostrup, Denmark). HPV16 E7 mRNA transcripts detection was performed by RT-PCR in 27 cases. The immunostaining for p16 was performed in all cases. Fourteen carcinomas (20%) were positive for high-risk HPV by PCR: 13 HPV16 and one HPV35. In situ hybridization showed a dotted nuclear positivity in all these cases. HPV16 E7 mRNA was detected in seven tumors harboring HPV16; in the remaining HPV-positive cases, RNA did not reach the quality for analysis. Strong, diffuse positivity for p16 was observed only in the HPV-positive cases. The 14 HPV-positive squamous cell carcinomas were non-keratinizing or scarcely keratinizing tumors. No significant differences were found in terms of gender, age, or staging at diagnosis between HPV-positive and HPV-negative tumors. However, differences in disease-free survival and overall survival between both groups of patients were significant (P=0.004 and P=0.028, respectively). In conclusion, we have shown that HPV is the etiological agent of a subset of sinonasal carcinomas demonstrating the transcriptionally active HPV in these tumors. Immunostaining for p16 can be used as a surrogate marker to identify these tumors.
Similar content being viewed by others

Main
High-risk human papillomavirus (HPV) has been etiologically associated with a subgroup of squamous cell carcinomas of the head and neck. The prevalence of the HPV-associated squamous cell carcinomas in this area mainly depends on the anatomic location: they are unusual in the larynx and oral mucosa and are frequent in the oropharynx.1, 2, 3
Over the past few years, the clinical importance of detecting these HPV-associated squamous cell carcinomas in the head and neck region has been stressed, and the HPV assessment is already recommended in the pathological evaluation of oropharyngeal squamous cell carcinomas by the American Joint Committee on Cancer.4 The HPV-associated squamous cell carcinomas are a biologically different entity from HPV-negative squamous cell carcinomas. They usually are non-keratinizing or scarcely keratinizing and may have the morphology of a poorly differentiated or basaloid squamous cell carcinoma, with high-proliferative scores. However, in spite of these apparently poor prognostic histological characteristics, these tumors present a very good response to therapy adjuvant to surgery, such as radiotherapy and chemotherapy, even when they are diagnosed at advanced stages.5, 6, 7, 8 This fact has a great relevance for squamous cell carcinomas of the sinonasal tract, where adjuvant therapy is usually required to treat the tumors, because of the complexity of the region anatomy that makes extensive surgery difficult in a large number of cases. However, it has been shown that HPV detection in squamous cell carcinomas is clinically and prognostically relevant only in those cases in which the virus is transcriptionally active.9 HPV causes malignant transformation of keratinocytes through the expression of the oncoproteins E6 and E7. The HPV E6 protein forms a complex with an ubiquitin ligase (E6-associated protein), and ubiquinates the p53 tumor-supressor protein. The HPV E7 protein binds to the cullin 2 ubiquitin ligase complex and ubiquitinates the retinoblastoma tumor-suppressor protein (pRb). Because of the absence of pRb function, the E2F family of transcription factors is released, leading to S-phase genes transcription and cell proliferation.10 The detection of HPV E6 or E7 messenger RNA (mRNA) is considered the gold standard in identifying the transcriptionally active HPV infection.9, 11 This identification permits confirmation that the HPV is the causative agent of the neoplasm, and has been previously reported in oropharyngeal carcinomas.9, 12, 13 In the sinonasal tract, previous studies performed by us and others have identified the presence of high-risk HPV DNA in about 20% of squamous cell carcinomas, in more than 90% of cases corresponding to HPV16.7, 14, 15, 16
In this study, we correlate the results of different techniques employed to detect HPV in a series of sinonasal squamous cell carcinomas, including the HPV16 E7 mRNA transcripts detection, with the aim of confirming the HPV as a causative agent of these neoplasms. In addition, we want to establish p16 immunostaining as a surrogate marker of this infection.
Materials and methods
Patients
The study was approved by the Hospital Clinic Institution Internal Review Board. All cases diagnosed as squamous cell carcinoma of the sinonasal tract in the Hospital Clinic from 1985 to 2010 were included in the survey. Tumor site and stage were determined from the review of the operative, radiology, and pathology reports. Tumors originating in the nasal vestibule were excluded. Tumor stage was assigned by using the 2010 American Joint Committee on Cancer staging criteria.4
Tumor Specimens
All tissues had been routinely fixed in 4% buffered neutral formalin and embedded in paraffin. Review of hematoxylin and eosin (H&E)-stained slides of tumor specimens was performed, and they were classified and graded according to the 2005 World Health Organization classification for Head and Neck tumors.17 In all cases, a representative block of the invasive carcinoma was selected for immunohistochemistry, in situ hybridization, and DNA analyses. RNA analyses were performed in 27 cases corresponding to all HPV-positive tumors (14) and 13 HPV-negative tumors diagnosed the last 5 years.
Tissue Preparation
Formalin-fixed, paraffin-embedded samples were serially sectioned on a microtome. The first and last sections (4 μm thick) were stained with H&E for histological confirmation of tumor presence. In-between sections (10 μm thick) were collected in RNAase-free reaction tubes (one for DNA isolation and one for RNA isolation). Sectioning and sample preparation were carried out with the highest measures to avoid contamination and cross-contamination.
RNA Isolation
RNA was isolated by digestion of deparaffinized sections in 0.1 mg/ml proteinase K solution overnight at 52 °C, followed by RNA extraction with TRIzol reagent (Invitrogen, Carlsbad, CA, USA), according to the manufacturer’s protocol. The final RNA pellet was washed twice with 200 ml of 70% ethanol, air-dried and re-suspended in 20–50 ml of RNAse/DNase-free water. RNA yields were quantified spectrophotometrically using the Nanodrop ND-1000 (Isogen Life Science, IJsselstein, the Netherlands).
Reverse Transcriptase-PCR
Before reverse transcriptase-PCR, analysis RNA samples were RQ1-DNAse-treated according to the manufacturer’s recommendations (Promega, Leiden, the Netherlands). Subsequently, reverse transcription using AMV RT (Promega) of RNA into cDNA was performed essentially as described before.18 A reaction without RT was run in parallel for each specimen to control for DNA contamination. To assess the quality of all RNA specimens, RT-PCR for the housekeeping gene encoding the U1 small nuclear ribonucleoprotein-specific A protein (snRNP U1A, 215 bp) was performed. Primers, annealing temperature and amplicon length are listed in Table 1.
DNA Extraction
Ten-micrometer-thick sections of formalin-fixed, paraffin-embedded tissues were cut using the sandwich technique, which implies that the first and last sections are stained with H&E and used to confirm the adequacy of the sample, whereas the central sections are used for DNA extraction. The microtome blade was replaced after each case. A vacuum cleaner was used to avoid cross-contamination between paraffin blocks. The tissue sections were digested with proteinase K in a volume of 250 μl at 56 °C overnight. Proteinase K was heat inactivated at 95 °C for 10 min. A 1/10 dilution of the sample was used for PCR (10 μl).
PCR
A broad-spectrum HPV DNA amplification was performed using the short PCR fragment (SPF10) primer set (Innogenetics Diagnostica, Spain). The SPF10 primers amplify a 65-bp fragment from the L1 region of the HPV genome. For HPV amplification, a 9-min denaturation step at 94 °C was followed by 40 cycles of amplification using 1.5 IU DNA polymerase (Amplitaq Gold DNA polymerase, Applied Biosystems) with a thermocycler (GeneAmp 9700, Applied Biosystems). These cycles included denaturation at 94 °C for 30 s, primer annealing at 52 °C for 45 s, and chain elongation at 72 °C for 45 s. The final elongation step was prolonged by 7 min.
Amplification products were first tested for the presence of HPV DNA by DNA enzyme-immunoassay (DEIA), which consists of hybridization with conserved probes in a microtiter-plate assay format (Universal DNA ELISA kit, Labo Bio-medical Products, BV Rijswick, the Netherlands). SPF10 amplimers from DEIA-HPV-positive samples were subsequently analyzed by reverse hybridization in an HPV line-probe assay LiPA25 system version 1 (Labo Bio-medical Products) at high stringency, generating a type-specific hybridization pattern. In this assay, 10 μl of denatured HPV PCR product was hybridized to the genotype-specific probes immobilized as parallel lines on a nitrocellulose strip. After the washing step, the products of hybridization were detected by a color reaction with alkaline-phosphatase-streptavidin conjugate and substrate (5-bromo-4-chloro-3-indolyl phosphate and nitroblue tetrazolium), which results in a purple precipitate. The results of the hybridization were assessed visually by comparing to the standard grid. The HPV LiPA25 version 1 permits specific detection of 25 HPV types: HPV 6, 11, 16, 18, 31, 33, 34, 35, 39, 40, 42, 43, 44, 45, 51, 52, 53, 54, 56, 58, 59, 66, 68 or 73, 70, and 74. These assays were automatically performed using the AutoLipa (Innogenetics) system for 48 strips.
To confirm DNA amplification, a second PCR using primers for β-globin was conducted with primers β-globin-PCO3 and β-globin-PCO5.
In Situ Hybridization
High-risk HPV was detected using the in situ hybridization catalyzed signal amplification method for biotinylated probe that covers several high-risk HPV types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68 (GenPoint HPV Probe Cocktail, Dako). Briefly, 5 μm tissue sections were deparaffined and, after heat-induced target retrieval in citrate buffer and digestion with proteinase K (Dako), were hybridized with the biotinylated probe. Signal detection was obtained by consecutive application of streptavidin–horseradish peroxidase complex and biotinyl tyramide. Hybridization was revealed by incubation with the chromogenic substrate diaminobenzidine.
The result was considered positive was considered when punctate nuclear brown signals were seen in the neoplastic cells.
Immunohistochemistry
Immunohistochemical study for p16 was done with the automated immunohistochemical system TechMate 500® (Dako), using the EnVision system (Dako) following previously reported protocols.19 p16 was detected using a monoclonal antibody (clone JC8, Biocare Medical, Walnut Creek, CA, USA; dilution 1:100, antigen retrieval with pressure cooker and 1 mM ethylenediaminetretraacetic acid, pH 8.0, 2 min).
Positivity for p16 was considered only when strong and diffuse cytoplasmic and nuclear staining was observed in all basal and suprabasal cells in all tumor nests.
Statistical Analyses
The results of quantitative variables are given as mean values and range. Qualitative variables are given as absolute and relative frequencies (percentages). Data were analyzed with the SPSS statistical package (version 15.0; SPSS, Chicago, IL, USA). Comparison between qualitative variables was performed through Fisher’s exact test. Differences in quantitative variables were analyzed with Student’s t-test. All statistical tests were two-sided, and significance was considered with an α-risk of 0.05.
Overall survival was defined as the time from the date of registration to the date of death or to the last date of follow-up. Disease-free survival was defined as the time from registration to local recurrence or metastasis. Death without documented progression was censored at the date of death. Survival data were analyzed by the Kaplan–Meier method, and survival curves were compared by using the log-rank test.
Results
HPV Detection and Immunohistochemistry
By PCR, 14 out of 70 tumors (20%) were HPV SPF10/DEIA positive, whereas the remaining 56 tumors were negative. In 13 out of 14 positive tumors (93%), a HPV type 16 was detected. One tumor (7%) harbored a HPV type 35.
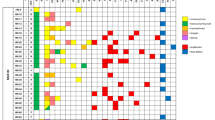
Reverse transcriptase-PCR analysis, performed in 27 cases, revealed HPV16 E7 mRNA expression in 7 HPV16-positive cases by PCR (Figure 1). Ten out of thirteen HPV-negative tumors did not expressed HPV16 E7 mRNA. In the remaining seven HPV-positive and three HPV-negative cases, U1A control was negative, therefore RNA did not reach the quality for appropriate mRNA analysis.

Agarose gel read-outs of reverse transcriptase PCRs determining mRNA expression of HPV-16 E7 and the housekeeping gene U1A, respectively, in HPV-16-positive samples. RT+ and RT− represent the results with and without reverse transcriptase added to the reverse transcriptase reaction before PCR.
By in situ hybridization, high-risk HPV DNA was detected in all 14 tumors positive by PCR. In all the cases, positivity was observed in the nuclei of the tumor cells and always showed a punctate dot pattern (Figure 2). The positive staining ranged from a single dotted signal to abundant dots into the neoplastic nuclei. All HPV-negative tumors by PCR were also negative for in situ hybridization.

(a) Histological features of a non-keratinizing squamous cell carcinoma (SCC) positive for HPV. The tumor infiltrates the stroma-forming well-circumscribed round nests. The neoplastic cells have hyperchromatic nuclei and scarce cytoplasm (HE × 100). (b) Immunohistochemical reaction for p16 protein of the same case. A strong, diffuse positivity in neoplastic nuclei and cytoplasms is shown (p16, × 100). (c) High-risk HPV DNA in situ hybridization (ISH) shows a dotted positivity in most neoplastic nuclei (ISH × 200). (d) Histological features of a poorly differentiated keratinizing SCC associated with HPV (HE, × 100). (e) Strong, diffuse positivity for p16 immunostain in the neoplastic cells (p16, × 100). (f) High-risk HPV DNA ISH shows a dotted positivity in scarce neoplastic nuclei, in this particular case (ISH, × 200).
All 14 cases positive for HPV by PCR and in situ hybridization showed strong, diffuse p16 immunostaining in the cytoplasm and nuclei of the neoplastic cells (Figure 2). In spite of some HPV-negative tumors showing a patchy or focal positivity for p16, no strong, diffuse immunostaining was seen in these cases. Thus, immunostaining for p16 had a specificity and sensitivity of 100% for the identification of HPV-positive cases.
Clinicopathological Characteristics of the Patients at Diagnosis
Fifty-one out of the seventy tumors (73%) arose in males and nineteen (27%) in females. The median age was 63.6 (range 40–93) years. The clinical and pathological characteristics of the patients with HPV-positive and -negative tumors are shown in Table 2. No significant differences were found in terms of age and gender between patients with HPV-positive or -negative tumors. At diagnosis, 37 tumors (53%) involved both the nasal and the paranasal structures. It was not possible to determine in these tumors the exact anatomical origin of the lesion. Among the remaining tumors, the HPV-positive carcinomas arose more frequently in the nasal cavity (4 out of 6), whereas HPV-negative neoplasms involved preferably the maxillary sinuses (20 out of 27), but the differences were not statistically significant (P=0.146).
Histologically, 49 tumors (70%) were conventional keratinizing squamous cell carcinomas; 14 tumors were non-keratinizing squamous cell carcinomas (20%); 5 tumors were basaloid squamous cell carcinomas (7%); and 2 tumors were papillary squamous cell carcinomas (3%). Among the 14 HPV-positive tumors, 8 were non-keratinizing squamous cell carcinomas; 2 were basaloid squamous cell carcinomas; 2 were papillary squamous cell carcinomas; and 2 were conventional keratinizing squamous cell carcinomas (both poorly differentiated and scarcely keratinizing; Figure 2). The histological differences between HPV-positive and -negative squamous cell carcinomas were statistically significant (P=0.001).
Fourteen squamous cell carcinomas developed from a sinonasal inverted papilloma. In 12 cases, areas of inverted papilloma were identified simultaneously with the squamous cell carcinoma. In two cases, the inverted papilloma had been previously excised, and no remnants of the benign lesion were identified. Only one of the carcinomas developing on sinonasal inverted papilloma was positive for HPV16.
In all, 24 carcinomas were stage IV (36%); 21 were stage III (28%); 18 were stage II (26%), and 7 were stage I (10%). No differences in tumor staging at diagnosis were identified between HPV-positive and -negative carcinomas (P=0.931).
Treatment and Survival Analyses
All patients were treated with surgical excision of the tumor and local radiotherapy as standard treatment, with the exception of seven stage I tumors that did not receive radiotherapy. Chemotherapy was added to all 24 patients with stage IV tumors and to additional 7 patients who developed metastases during the follow-up.
Mean disease-free survival in the HPV-positive group was 65.8 months (±9.8 standard error), whereas in the HPV-negative group was 30.47 months (±4.9 standard error). These results were statistically significant (P=0.004). Mean overall survival in the HPV-positive group was 156.8 months (±47.2 standard error), whereas in the HPV-negative group was 72 months (±12.3 standard error). These results were also statistically significant (P=0.028).
Discussion
In this study, we show a good correlation between the different techniques employed to detect HPV in a series of sinonasal squamous cell carcinomas. We have been able to detect HPV16 E7 mRNA transcripts expression in a subset of carcinomas, which confirms the etiological role of high-risk HPV in the development of these tumors.
By PCR, using the SPF10 probe, we have determined that 13 out of 14 positive cases (93%) harbored HPV16, as also occur in oropharyngeal HPV-positive carcinomas.2 HPV DNA detection by PCR permits the identification of the involved HPV subtype and is a highly sensitive method. However, some authors have found low specificity using this technique due to the occasional presence of transcriptionally inactive viral DNA.9, 20 In our series, in all the HPV-positive cases by PCR we have visualized the DNA HPV into the neoplastic nuclei through in situ hybridization using a high-risk HPV cocktail probe. The HPV DNA detection through in situ hybridization allows the detection and visualization of the viral DNA in the tumor nuclei. The pattern of positivity may distinguish between episomal (extrachromosomal) and integrated forms. In the former situation, there is diffuse positivity, whereas in the latter, there is punctate, dotted positivity, which we have demonstrated in all of the HPV-associated squamous cell carcinomas. This technique must be considered positive even when few nuclear signals are seen.21 In spite of being a very specific technique, no information about the active HPV transcription is given.20 The importance of detecting HPV-positive squamous cell carcinomas is due to the relevant clinical and prognostic implications associated with this infection. HPV-positive tumors are highly responsive to radiotherapy and chemotherapy, and have better prognosis compared with HPV-negative squamous cell carcinomas.5, 6, 7, 8 However, these clinical and prognostic implications are restricted to those tumors in which the HPV is transcriptionally active. In this study, we have showed significant differences in disease-free survival and overall survival between patients with HPV-positive and HPV-negative tumors (P=0.004 and P=0.028, respectively).Thus, the identification of the mRNA for the viral oncoproteins E6 and E7 has been proposed as the gold standard to detect the squamous cell carcinomas oncogenically related to HPV.18 Recently, an HPV E6/E7 mRNA in situ hybridization assay has been developed and proved useful in detecting the HPV-associated squamous cell carcinomas of the oropharynx.12, 13
Squamous cell carcinomas associated with high-risk HPV infection have a different tumor biology compared with other head and neck squamous cell carcinomas.11 The integration of high-risk HPV DNA into the host cell leads to a disruption of the viral gene E2, which results in a loss of its function. One of the functions of this gene is the regulation of the transcription of the oncoproteins E6 and E7. In consequence, there is an overexpression of E6 and E7.11, 22 These oncoproteins have a role in cell transformation and immortalization, through binding and inactivation of TP53 and Rb tumor-supressor gene products, respectively.23 Consequently, there is a deregulation of two crucial cellular mechanisms, the cell cycle and the apoptotic pathway, which is the basis of the HPV-induced carcinogenesis. The cell-cycle protein p16, encoded by the CDKN2A (INK4A, MTS1) tumor-suppressor gene, decelerates the cell cycle through the retinoblastoma pathway. In HPV-associated carcinogenesis, the inactivation of Rb by the viral gene E7 results in a marked overexpression of p16 protein. This overexpression has been extensively documented in HPV-positive carcinomas of the uterine cervix, vulva, penis, and anorrectal region,19, 24 as well as in the head and neck region.25, 26 Our study confirms that p16 immunostaining can be considered a surrogate marker of high-risk HPV infection in squamous cell carcinomas of the sinonasal region. Conversely, some studies on oropharyngeal carcinomas have observed that a small number of p16-positive cases do not harbor HPV DNA.18, 27 This finding has been attributed either to a low sensitivity of the technique used to detect HPV DNA as well as to the presence of other mechanisms resulting in p16 overexpression regardless of HPV infection. It should be stressed that only strong, diffuse nuclear, and cytoplasmic positivity involving basal and parabasal cells should be considered as positive reaction for p16. Patchy or irregular staining patterns should be considered negative for HPV identification purposes.9, 18, 20, 28
This study confirms that the sinonasal region is, after the oropharynx, the second most prevalent anatomical site of the head and neck region for HPV-positive squamous cell carcinomas, in agreement with previously published studies by our group and others.7, 14, 15, 16
In our series, most HPV-positive squamous cell carcinomas arose in the nasal cavity, whereas most HPV-negative squamous cell carcinomas arose in the maxillary sinuses. Two different hypotheses have been proposed to account for this finding. First, it is known that HPV is transmitted from one individual to another through direct contact, and nasal cavities are easily accessible. On the other hand, mucosal junctions or squamocolumnar transitions, such as the cervix and the anal canal, are prone to develop HPV-related squamous lesions and squamous cell carcinomas. These anatomical sites are usually associated with chronic inflammation and deregulated expression of soluble and cell membrane factors important for antiviral immune response.29
Interestingly, the vast majority of the HPV-positive squamous cell carcinomas in our series appeared de novo, and only one case developed from a sinonasal papilloma. Conversely, most squamous cell carcinomas arising from sinonasal inverted papilloma were HPV negative. There are some controversies in the literature about the relationship between the sinonasal papillomas and HPV, especially types 6 and 11, which are rarely detected.30
Most HPV-positive squamous cell carcinomas in our series were of the non-keratinizing type, two cases had the morphology of squamous basaloid carcinoma and two were papillary squamous cell carcinoma.17 However, two cases had the morphology of poorly differentiated conventional keratinizing squamous cell carcinoma. Similar histological characteristics have been described in oropharyngeal squamous cell carcinomas associated with HPV.31, 32 It has become essential to reclassify the head and neck squamous cell carcinomas based on their association with HPV for determining the prognosis and patient management, instead of using the purely morphological classification.33
In conclusion, we confirm in this study that high-risk HPV are etiologically involved in 20% of squamous cell carcinomas of the sinonasal tract. P16 immunostaining must be considered a surrogate marker in identifying these tumors.
We propose here a diagnostic algorithm to detect the sinonasal squamous cell carcinomas associated with high-risk HPV. Standard histology combined with p16 immunohistochemistry must be used in a first screening step. Later, specific techniques to confirm HPV, such as PCR or in situ hybridization can be performed in the p16-positive cases.
References
Gillison ML, Koch WM, Capone RB et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 2000;92:709–720.
D'Souza G, Kreimer AR, Viscidi R et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 2007;356:1944–1956.
Lewis JS Jr., Ukpo OC, Ma XJ et al. Transcriptionally-active high-risk human papillomavirus is rare in oral cavity and laryngeal/hypopharyngeal squamous cell carcinomas—a tissue microarray study utilizing E6/E7 mRNA in situ hybridization. Histopathology 2012;60:982–991.
Edge SB, Compton CC . The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010;17:1471–1474.
Lindel K, Beer KT, Laissue J et al. Human papillomavirus positive squamous cell carcinoma of the oropharynx: a radiosensitive subgroup of head and neck carcinoma. Cancer 2001;92:805–813.
Fakhry C, Gillison ML . Clinical implications of human papillomavirus in head and neck cancers. J Clin Oncol 2006;24:2606–2611.
Alos L, Moyano S, Nadal A et al. Human papillomaviruses are identified in a subgroup of sinonasal squamous cell carcinomas with favorable outcome. Cancer 2009;115:2701–2709.
Ang KK, Harris J, Wheeler R et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 2010;363:24–35.
Adelstein DJ, Ridge JA, Gillison ML et al. Head and neck squamous cell cancer and the human papillomavirus: summary of a National Cancer Institute State of the Science Meeting, November 9-10, 2008, Washington D.C. Head Neck 2009;31:1393–1422.
Laughlin-Drubin ME, Munger K . Oncogenic activities of human papillomaviruses. Virus Res 2009;143:195–208.
Chung CH, Gillison ML . Human papillomavirus in head and neck cancer: its role in pathogenesis and clinical implications. Clin Cancer Res 2009;15:6758–6762.
Ukpo OC, Flanagan JJ, Ma XJ et al. High-risk human papillomavirus E6/E7 mRNA detection by a novel in situ hybridization assay strongly correlates with p16 expression and patient outcomes in oropharyngeal squamous cell carcinoma. Am J Surg Pathol 2011;35:1343–1350.
Bishop JA, Ma XJ, Wang H et al. Detection of transcriptionally active high-risk HPV in patients with head and neck squamous cell carcinoma as visualized by a novel E6/E7 mRNA in situ hybridization method. Am J Surg Pathol 2012;36:1874–1882.
El-Mofty SK, Lu DW . Prevalence of high-risk human papillomavirus DNA in nonkeratinizing (cylindrical cell) carcinoma of the sinonasal tract: a distinct clinicopathologic and molecular disease entity. Am J Surg Pathol 2005;29:1367–1372.
Hoffmann M, Klose N, Gottschlich S et al. Detection of human papillomavirus DNA in benign and malignant sinonasal neoplasms. Cancer Lett 2006;239:64–70.
Bishop JA, Guo TW, Smith DF et al. Human papillomavirus-related carcinomas of the sinonasal tract. Am J Surg Pathol 2013;37:185–192.
Pilch BZ, Bouquot J . Thompson LDR. Squamous cell carcinoma In: Barnes EL, et al (eds). World Health Organization Classification of Tumours-Pathology and Genetics-Head and Neck Tumours. IARC Press: Lyon, France, 2005, pp 15–17.
Smeets SJ, Hesselink AT, Speel EJ et al. A novel algorithm for reliable detection of human papillomavirus in paraffin embedded head and neck cancer specimen. Int J Cancer 2007;121:2465–2472.
Santos M, Landolfi S, Olivella A et al. p16 overexpression identifies HPV-positive vulvar squamous cell carcinomas. Am J Surg Pathol 2006;30:1347–1356.
Schlecht NF, Brandwein-Gensler M, Nuovo GJ et al. A comparison of clinically utilized human papillomavirus detection methods in head and neck cancer. Mod Pathol 2011;24:1295–1305.
Huang CC, Qiu JT, Kashima ML et al. Generation of type-specific probes for the detection of single-copy human papillomavirus by a novel in situ hybridization method. Mod Pathol 1998;11:971–977.
Stelow EB, Jo VY, Stoler MH et al. Human papillomavirus-associated squamous cell carcinoma of the upper aerodigestive tract. Am J Surg Pathol 2010;34:e15–e24.
zur Hausen H . Papillomaviruses and cancer: from basic studies to clinical application. Nat Rev Cancer 2002;2:342–350.
Klaes R, Benner A, Friedrich T et al. p16INK4a immunohistochemistry improves interobserver agreement in the diagnosis of cervical intraepithelial neoplasia. Am J Surg Pathol 2002;26:1389–1399.
Klussmann JP, Gultekin E, Weissenborn SJ et al. Expression of p16 protein identifies a distinct entity of tonsillar carcinomas associated with human papillomavirus. Am J Pathol 2003;162:747–753.
Singhi AD, Westra WH . Comparison of human papillomavirus in situ hybridization and p16 immunohistochemistry in the detection of human papillomavirus-associated head and neck cancer based on a prospective clinical experience. Cancer 2010;116:2166–2173.
Lewis JS Jr., Thorstad WL, Chernock RD et al. p16 positive oropharyngeal squamous cell carcinoma:an entity with a favorable prognosis regardless of tumor HPV status. Am J Surg Pathol 2010;34:1088–1096.
Lewis JS Jr., Chernock RD, Ma XJ et al. Partial p16 staining in oropharyngeal squamous cell carcinoma: extent and pattern correlate with human papillomavirus RNA status. Mod Pathol 2012;25:1212–1220.
Herfs M, Hubert P, Moutschen M et al. Mucosal junctions: open doors to HPV and HIV infections? Trends Microbiol 2011;19:114–120.
Jenko K, Kocjan B, Zidar N et al. In inverted papillomas HPV more likely represents incidental colonization than an etiological factor. Virchows Arch 2011;459:529–538.
Begum S, Westra WH . Basaloid squamous cell carcinoma of the head and neck is a mixed variant that can be further resolved by HPV status. Am J Surg Pathol 2008;32:1044–1050.
Jo VY, Mills SE, Stoler MH et al. Papillary squamous cell carcinoma of the head and neck: frequent association with human papillomavirus infection and invasive carcinoma. Am J Surg Pathol 2009;33:1720–1724.
Brandwein-Gensler M, Smith RV . Prognostic indicators in head and neck oncology including the new 7th edition of the AJCC staging system. Head Neck Pathol 2010;4:53–61.
Acknowledgements
We are grateful to Ingrid Lopez for the technical support and Gema Laguna for the secretarial assistance. This work was funded by Instituto de Salud Carlos III (ICSiii)-Fondos de Investigación Sanitaria and ERDF ‘one way to Europe’ (PI11/01570, PI12/01165) and the Fundacion Mutua Madrileña (FMM 2011 AP94722011).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Larque, A., Hakim, S., Ordi, J. et al. High-risk human papillomavirus is transcriptionally active in a subset of sinonasal squamous cell carcinomas. Mod Pathol 27, 343–351 (2014). https://doi.org/10.1038/modpathol.2013.155
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2013.155
Keywords
This article is cited by
-
Evaluation of high-risk human papillomavirus in sinonasal papillomas and squamous cell carcinomas
Virchows Archiv (2023)
-
Histopathologic Diagnosis of Sinonasal Tumors: Challenges and the Importance of Establishing the Correct Diagnosis
Current Otorhinolaryngology Reports (2023)
-
Nuclear expression of AFF2 C-terminus is a sensitive and specific ancillary marker for DEK::AFF2 carcinoma of the sinonasal tract
Modern Pathology (2022)
-
Accuracy of liquid-based brush cytology and HPV detection for the diagnosis and management of patients with oropharyngeal and oral cancer
Clinical Oral Investigations (2022)
-
Human Papillomavirus-Related Carcinomas of the Sinonasal Tract
Current Otorhinolaryngology Reports (2022)
