
Abstract
Primary cutaneous marginal zone B-cell lymphoma is considered the cutaneous counterpart of extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue. Although its molecular pathogenesis is currently unknown, an etiological link with Borrelia burgdorferi infection has been identified in European, but not in American or Asian cases. To better understand the pathogenesis and the geographical differences of cutaneous marginal zone B-cell lymphoma, 60 cases from the East Asia, Germany, and the United States at their initial presentation were subjected to the following analyses; (1) clinicopathological comparison between the geographical regions, (2) detection of B. burgdorferi DNA, (3) detection of the API2–MALT1 fusion transcript, a gene alteration specific to mucosa-associated lymphoid tissue lymphoma, and (4) inactivation of tumor suppressor genes (death-associated protein kinase (DAPK), p16INK4a, p14ARF, MGMT, TIMP3, CDH1, and RARB) by hypermethylation of the CpG islands. Cases from the three geographical regions showed similar clinicopathological features. However, moderate/marked tissue eosinophilia was found in 9/25 Asian cases, but only 1/23 German cases (P=0.011) and 0/12 American cases (P=0.015). All 60 cases were negative for either Borrelia DNA or API2–MALT1 fusion. Tumors from the three regions were highly methylated for DAPK (38–50% of the cases, mean 43%) and p16INK4a (42–70%, mean 49%), and the positivities were significantly higher than those of nonneoplastic skin (8%, P=0.0010 and 14%, P=0.0032, respectively). Methylation of these genes had no significant association with progressive features of the tumor. Primary cutaneous marginal zone B-cell lymphomas from the three geographical regions have common clinicopathological features, however, moderate/marked tissue eosinophilia is a feature found almost exclusively in Asian cases. Borrelia infection and API2–MALT1 fusion are not significant in this tumor. Methylation of DAPK and p16INK4a genes is a frequent event in this lymphoma at its initial presentation, but may not be associated with tumor progression.
Similar content being viewed by others


Main
Primary cutaneous marginal zone B-cell lymphoma is now considered a distinct entity in the World Health Organization (WHO)–European Organization Research and Treatment of Cancer (EORTC) classification of cutaneous lymphomas.1, 2 This tumor is histologically characterized by small B cells including marginal zone (centrocyte-like), monocytoid, and plasmacytoid lymphocytes, and plasma cells, and is considered part of the broad group of extranodal marginal zone B-cell lymphomas commonly involving mucosa-associated lymphoid tissue (MALT). This lymphoma is rare, often affects adults aged more than 40 years of age with no clear gender preponderance, and has a favorable prognosis.1, 2, 3
The etiology of cutaneous marginal zone B-cell lymphoma has not been well clarified. Evidence suggesting a link between this lymphoma and Borrelia burgdorferi infection has been reported from many European countries including Germany, and penicillin therapy may cure B. burgdorferi-associated cases.4, 5, 6, 7 However, this association has not been evident in the United States or Asia.8, 9 API2–MALT1 fusion, resulting from t(11;18)(q21;q21) is specific to MALT lymphoma, and has been found in 10–20% of gastric cases and in up to 50% of pulmonary cases, but is rare in autoimmune-associated cases.10 This gene alteration has been reported in 0–7.8% of cutaneous marginal zone B-cell lymphomas,9, 11, 12, 13, 14, 15, 16 but overall its frequency is not clear.
As the skin is one of the most important immune defense systems, cutaneous lymphoproliferative disorders are considered to be associated with environmental or geographical factors, especially in marginal zone B-cell lymphoma, which shows a close association with chronic inflammation. The present international study with cutaneous marginal zone B-cell lymphoma from East Asia, Germany, and the United States was designed to investigate any possible geographical differences among these cases, and to detect underlying biologic or genetic abnormalities. We analyzed the clinicopathological features of 60 cases of primary cutaneous marginal zone B-cell lymphoma, and searched for B. burgdorferi infection and API2–MALT1 fusion involvement. In addition, we studied inactivation of tumor suppressor genes by hypermethylation of the CpG islands, which is one of the important steps in the development of clinically overt tumors including malignant lymphoma.
Materials and methods
Case Selection
Asian cases of primary cutaneous marginal zone B-cell lymphoma were retrieved from the files of Department of Pathology, Chang Gung University, Taiwan, and Department of Pathology, Nagoya City University, Japan. Cases from Germany and the United States were retrieved from the files of the Department of Pathology, University of Wuerzburg, and the Department of Pathology, University of Pittsburgh, respectively. A total of 105 cases suspected of cutaneous marginal zone B-cell lymphoma were reviewed by hematopathologists. Of them, 55 cases were excluded either because they did not fulfill the criteria of the criteria for a cutaneous marginal zone B-cell lymphoma according to the criteria of WHO–EORTC classification for cutaneous lymphomas,1, 2 they were recurrences, or they lacked demonstrable monoclonality either based on immunoglobulin light chain restriction or IGH gene rearrangement.9 Clinical data (age, sex, primary site, treatment, response, and follow-up) were obtained. Clinical data concerning gross appearance and number of lesions (solitary or multiple) were available in Asian cases. In all cases, there was no history of extracutaneous lymphoma, either previous or concurrent, and no evidence of extracutaneous lymphoma for 6 months after the appearance of the cutaneous lesion.
All cases were within the morphological boundaries of primary cutaneous marginal zone B-cell lymphoma, and exhibited the following immunophenotype: CD20(+), CD79a(+), CD3(−), CD45RO(−), CD5(−), CD10(−), CD23(−), BCL2(+), BCL6(−), and cyclin D1(−). The following pathological/phenotypic factors were analyzed in the cases from three geographical regions: proliferation pattern, increased lymphoid follicles, marked plasma cells, increased large cells, tissue eosinophilia, and nuclear BCL10 expression. When most lymphoma cells showed intense nuclear BCL10 expression, the case was considered as positive. Cases were considered to have increased large cells when more than 5% and less than 10% large cells were observed without solid or sheet-like proliferations.17 Tissue eosinophilia was semi-quantified into three groups: absent or mild, less than 50 eosinophils/10 high power fields (HPFs); moderate, 50–200 eosinophils/10 HPFs; and marked, more than 200 eosinophils/10 HPFs. Local ethical guidelines were followed for the use of archival materials for research, and such use was approved by the ethics committees of the authors' institutions where required. As a control, 29 nonneoplastic skin biopsies were obtained from Japanese patients. All specimens were fixed in formalin, and embedded in paraffin. Some of the tumors from Asian cases in this series were included in our previous study.9
Extraction of Genomic DNA and Total RNA
Genomic DNA and total RNA were extracted from paraffin sections in digestion buffer containing proteinase K as previously described.18 For lymphoma cases, only lymphomatous areas were scraped with examination of tissue sections under a dissecting microscope, using a serial H&E section as a guide. For control skin, only the dermal layer was scraped. We confirmed that all cases had a sufficient quality of DNA and RNA by polymerase chain reaction (PCR) for β-globin gene and reverse transcription (RT)–PCR for β-actin mRNA, respectively.
PCR Detection of Borrelia DNA
As reported previously, we performed PCR using consensus primers for B. burgdorferi hbb gene, which encodes a protein of histone-like family. The PCR product is expected to be 184 bp in length, and well suited to DNA extraction from paraffin tissue materials.9 This PCR assay should cover 39 Borrelia strains. DNA extracted from heat-treated B. burgdorferi (Kirkegaad and Perry Lab, Gathersburg, MD, USA) was used as a positive control. The sequence analysis of the PCR product of the positive control showed 98% homology with the reference B. burgdorferi strain, B31.9 Normal human DNA extracted from various paraffin-embedded materials, including the skin, spleen, and lymph nodes, yielded no positive bands in this PCR assay.
Multiplex RT–PCR for the API2–MALT1 Fusion Transcript
The API2–MALT1 fusion transcript was detected according to the method we previously described.19 All eight variant transcripts known to date can be detected with this assay. Briefly, total RNA was subjected to first-round multiplex one-tube RT–PCR, then to second-round nested multiplex PCRs (three in parallel). This RT–PCR assay using paraffin tissues is highly efficient and has 94% of the sensitivity and 100% of the specificity obtained with RT–PCR using frozen materials.20
Methylation-Specific PCR
As described elsewhere, DNA from the specimens was first subjected to bisulfite treatment.21 Denatured DNA was modified by reaction with sodium bisulfite under conditions that convert all unmethylated cytosine residues to uracil by deamination. Modified DNA was purified, and modification was completed by NaOH treatment, followed by ethanol precipitation. Bisulfite-modified DNA was then subjected to PCR amplification using primers designed to anneal specifically to the methylated and unmethylated DNA within a given gene. In this study, we analyzed the hypermethylation status in the promotor CpG islands of following seven tumor suppressor genes: death-associated protein kinase (DAPK), p16INK4a (p16), p14ARF (p14), O-6-methylguanine-DNA methytransferase (MGMT), tissue inhibitor of metalloproteinase 3 (TIMP3), E-cadherin (CDH1), and retinoic acid receptor-β (RARB). The primer sequences are shown in Supplementary data 1. PCR was performed for 35 cycles, and the annealing temperature ranged from 55 to 63°C depending on the primer pairs used.
Statistical Analysis
Statistical comparisons were performed using Fischer's exact test and χ2-test. To identify the parameters significantly associated with an overall survival, the statistical difference was estimated using the log-rank and Wilcoxon tests. All analyses were two tailed. A value of P<0.05 for each test was regarded as statistically significant. All of the analyses were performed using the statistical package JMP (SAS Institute Inc., Cary, NC, USA).
Results
Clinicopathological Findings
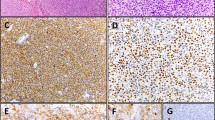
All 60 cases of primary cutaneous marginal zone B-cell lymphoma occurred in adults (mean age of 56 years, median 57, range 26–87), with no differences in age between patients from the three regions (Asia, Germany, and the United States; Table 1). No gender preponderance was noted. In 25 Asian cases, tumors were found in the head and neck, trunk, and upper extremities in 10 (40%), 8 (32%), and 7 (28%) cases, respectively. Tumors were frequently found on the trunk (9/23, 39%) and upper extremities (6/23, 26%) in German cases, and mostly on the trunk (9/12, 75%) in the cases from the United States. The cases from the three geographical regions showed similar histological findings (Figure 1a–d). The dermis showed a nonepidermotropic diffuse and nodular proliferation of small- to medium-sized lymphoid cells with reactive lymphoid follicles. The lymphoid cells had centrocyte-like or monocytoid appearance with pale cytoplasm, slightly irregular nuclei, and inconspicuous nucleoli. Marked plasmacytic differentiation was found in 19/60 (32%) cases, and increased large cells in 12/60 (20%) cases. Moderate or marked tissue eosinophilia in the tumor tissue was detected frequently in 9 (36%) of 25 Asian cases (Figure 1e), but in only 1 (4%) of 23 German, and none of 12 American cases (P=0.011, Asia vs Germany; P=0.015, Asia vs the United States; Table 1). There were no significant differences between Asian cases with and without tissue eosinophilia with regard to the following clinicopathological factors: age, sex, primary site, gross appearance, solitary or multiple, proliferation pattern, increased lymphoid follicles, marked plasma cells, and nuclear BCL10 expression. Nuclear BCL10 expression was detected in 30–40% of the cases, and there were no regional differences (Table 1).

Histopathological findings in primary cutaneous marginal zone B-cell lymphoma. (a) Nodular proliferation of dense lymphoid cells mainly in the dermis. H&E staining, original magnification × 40. (b) Lymphoid and plasmacytic cells with frequent intranuclear pseudoinclusions (Dutcher bodies, arrows), H&E staining, original magnification × 400. (c, d) Tumor cells showing immunoglobulin light chain restriction (c, κ-type; d, λ-type), hematoxylin counterstain, original magnification × 400. (e) A representative case of tissue eosinophilia (an Asian case). This case is graded as ‘moderate’. H&E staining, original magnification × 200.
Follow-up data were retrieved from 27 cases (Table 2). The follow-up period ranged from 7 to 180 months (median 36 months, mean 57 months). After a variety of treatments including surgical excision, topical steroid, psoralen and ultraviolet A phototherapy, and chemotherapy, 17 patients achieved a complete remission and 3 patients showed a partial remission, whereas 2 patients showed no change, and 3 showed progressive disease. Response to treatment was unknown in two cases. Of 17 patients with a complete remission, 5 relapsed. One case, which was observed with no treatment, showed spontaneous regression and no recurrence during the follow-up (Case 2, Table 2). Another case, which had no treatment, showed partial tumor regression but with persistent tumor 60 months after its initial presentation (Case 13, Table 2). None of the patients died of the lymphoma.
Borrelia DNA and the API2–MALT1 Fusion Transcript
Satisfactory preservation of DNA was verified in all 60 cases by successful amplification of the β-globin DNA fragments. Borrelia DNA was not found in any case from Asia, Germany, or the United States (Figure 2). This negative result was confirmed by at least two separate experiments whereas the positive control for Borrelia DNA constantly showed a distinct PCR band. The API2–MALT1 fusion transcript was examined using multiplex RT–PCR. A sufficient quality of RNA was preserved in all 60 cases as evidenced by amplification of reference β-actin mRNA. No case showed the fusion transcript, a finding that was confirmed by repeat assays (Figure 3). Positive controls yielded definite bands.

Detection of Borrelia DNA by PCR amplifying a fragment of conserved hbb gene. N, negative control; P, positive control; lanes 1–7, tumor cases showing no detectable PCR products. bp, base pair.

Detection of API2–MALT1 fusion transcript by multiplex RT–PCR (second PCR-B). N, negative control; P1–P4, four variants of API2–MALT1 fusion used as positive controls (note that PCR bands vary in size); lanes 1–7, tumor cases negative for the fusion transcript.
Gene Methylation Status
As shown in Figure 4, the promoter regions of seven tumor suppressor genes (DAPK, p16, p14, MGMT, TIMP3, CDH1, and RARB) were analyzed for gene methylation in 89 skin biopsies (60 tumor cases and 29 cases of nonneoplastic skin). As summarized in Figure 5, methylation status was successfully evaluated for the former five genes in more than 88% of the cases, although the evaluation was somewhat lower in the latter two with mean detection rates of 77 and 73%, respectively. DAPK gene methylation was detected in 9/24 (38%), 6/12 (50%), and 10/22 (45%) of tumor cases from Asia, Germany, and the United States, respectively (differences not significant), with an average of 25/58 (43%) cases. DAPK was methylated in 2/26 (8%) nonneoplastic control cases. DAPK methylation ratios for each geographical region and that of total cases were significantly higher than that of nonneoplastic skin (Table 3). p16 gene methylation was frequently detected in cutaneous marginal zone B-cell lymphoma cases, and the detection was similar between the three regions (42, 47, and 60% in Asia, Germany, and the United States, respectively) with an average of 47% (25/53 cases). p16 gene methylation in tumor cases was significantly higher than control cases (4/28, 14%; Table 4). The other five genes (p14, MGMT, TIMP3, CDH1, and RARB) were differentially methylated in 47, 7, 15, 31, and 14% of the tumor cases, respectively. These methylation ratios were not statistically different from those of the control skin.

Methylation-specific PCR for methylation status of seven tumor suppressor genes, DAPK, p16, p14, MGMT, TIMP3, CDH1, and RARB. Cases 1–8, tumor cases; M, methylated; U, unmethylated. The PCR product sizes are shown in Supplementary data 1.

Methylation profile of seven tumor suppressor genes in 60 cases of primary cutaneous marginal zone B-cell lymphoma and 29 cases of the control skin. Filled boxes indicate methylated sites, open boxes indicate unmethylated sites, and gray boxes indicate that the methylation status is not determined.
When association of gene hypermethylation with clinicopathological factors was analyzed, none of the following factors showed a statistically significant association with the methylation status of either DAPK or p16 gene (Table 4): age, sex, primary site, gross appearance, proliferation pattern, increased lymphoid follicles, marked plasmacytic differentiation, increased large-cell element, tissue eosinophilia, and BCL10 expression. Prognostic analysis showed that p16 and DAPK hypermethylation had no impact on the disease-free survival of the patients (data not shown).
Discussion
In the present study, we examined 60 cases of primary cutaneous marginal zone B-cell lymphoma from Asia, Germany, and the United States. These cases generally showed clinicopathological features similar to those that have been described. However, a predominant localization to the trunk and upper extremities1, 2 was not shown in this study. The prognosis of the patients was excellent with no tumor-related deaths recorded in this study. However, the therapeutic response was not very satisfactory. A complete remission was achieved in 17 (68%) of 25 cases with known responses to treatment. Among these 17 patients, 5 cases showed tumor recurrence but without any lymphoma-related deaths. In total, 13/25 (52%) patients were alive with disease at the last follow-up. This finding confirmed previous observations that primary cutaneous marginal zone B-cell lymphoma is an indolent tumor, but often shows resistance to or recurrence after treatment of the tumor.3, 22
Of note, we found that moderate or marked tissue eosinophilia was observed frequently in Asian cases, which has not been noted before. In contrast, this finding was almost absent in Germany and the United States cases. Tissue eosinophilia has been reported in 4 of 15 American cases,23 although the degree of eosinophilia was not specified. In malignant lymphoma, tissue eosinophilia is often associated in Hodgkin's lymphoma and T-cell lymphoma.24, 25 This phenomenon may be associated with production of certain cytokines by the tumor cells, and may have a prognostic significance.26 In B-cell lymphomas, however, tissue eosinophilia is rare, and its significance is unknown.27 In the present series, we found no significant differences in the clinicopathological features between those with and without tissue eosinophilia. We speculate that frequent tissue eosinophilia may be associated with ethnic or geographical factors. One such example is Kimura's disease, which is characterized by marked eosinophilia.28, 29 This benign disorder, involving the skin as well as the lymph nodes, is known to be comparatively frequent in Asian countries.
A subset of primary cutaneous marginal zone B-cell lymphoma cases has been associated with B. burgdorferi, however, there appears to be geographic variation. Borrelia infection has been documented serologically, and Borrelia-specific DNA has been detected by PCR and Southern blot analysis.4, 5, 6, 7 In addition, antibiotic therapy has been effective in some cases that were positive for B. burgdorferi.6, 7 Interestingly, this association has been reported mainly from Europe, but rarely from the United States.8, 30 We previously reported that such an association is also rare in Asian cases.9 In this international study including cases from Asia, Germany, and the United States, we found that none of the cases was positive for B. burgdorferi DNA. Although this negative PCR result does not exclude the possibility of a link between the tumor and B. burgdorferi infection, the microorganism is not significant in the development or pathogenesis of the cases of primary cutaneous marginal zone B-cell lymphoma.
The molecular pathogenesis of cutaneous marginal zone B-cell lymphoma is poorly understood with the translocations associated with other MALT lymphomas reportedly found in few cases. Streubel et al12 reported API2–MALT1 translocation in 4 of 51 cases, but others, including the cases reported here, did not detect any cases with this abnormality.9, 11, 13, 14, 15, 16 The IGH–MALT1 translocation has been reported in 7/51 cases12 and 3/12 cases.15 However, it was absent in several other studies.13, 14 The explanation for these variable results remains unknown. In MALT lymphomas, an association between nuclear BCL10 expression and the presence of API2–MALT1 fusion has been suggested.10, 31 However, such an association was not evident in our series where frequent nuclear BCL10 expression in tumor cells was shown in the absence of API2–MALT1 fusion, as has been reported previously.9, 16 In cutaneous marginal zone B-cell lymphoma, nuclear BCL10 expression has not been associated with BCL10 gene mutation9 or other MALT1 gene translocations.16 These molecular data indicate that some other mechanisms exist for nuclear BCL10 expression in cutaneous marginal zone B-cell lymphoma.
Inactivation of tumor suppressor genes by hypermethylation of the CpG islands is one of the important processes in the development of clinically overt tumors. To the best of our knowledge, this epigenetic abnormality has not been studied in primary cutaneous marginal zone B-cell lymphoma. We therefore analyzed methylation of seven tumor suppressor genes, and found that DAPK and p16 genes were highly methylated in tumor cases whereas nonneoplastic skin tissues (from Asian individuals) were rarely methylated. A similar low methylation of the two genes in nonneoplastic skin has been reported from the United States.32
DAPK is a novel calcium/calmodulin-dependent and cytoskeletal-associated serine/threonine kinase with death-inducing functions.33, 34 The DAPK gene was initially isolated as a positive mediator of apoptosis induced by interferon-γ. Overexpression of DAPK in tumor cells led to cell death in the absence of any external stimuli. Recent studies showed that this molecule also participates in tumor necrosis factor-α and Fas-induced apoptosis.35, 36 The p16 gene encodes for nuclear protein that can block cell-cycle progression from the G1 to the S phase by effectively inhibiting the kinase activity of CDK4/6, thereby exerting a negative control on cell proliferation.37, 38, 39 Loss of p16 expression gives a remarkable growth advantage in cells. These observations highlight a potential role of DAPK and p16 as tumor suppressor genes. We showed that both DAPK and p16 genes were frequently methylated in tumor cases at their initial presentation (approximately 45% of the cases) and that these epigenetic alterations had no impact on clinicopathological and prognostic features of this lymphoma. These findings suggest that methylation of these genes is a molecular event that may contribute more to the development of the tumor than to its progression. In other B-cell malignancies, DAPK and p16 gene methylation has been associated with tumor progression.40, 41, 42 However, recent studies have shown that methylation of these genes may be an early event in lymphomagenesis: DAPK and p16 gene methylation is frequently found in premalignant and low-grade lymphoid disorders, not associated with tumor progression, and their methylation status is maintained in higher-grade or advanced lymphoid neoplasms.43, 44, 45, 46, 47, 48 In line with these findings, methylation of DAPK and p16 is a common, early epigenetic phenomenon that allows tumor cells to promote cell-cycle progression and escape the normal apoptosis of a non-antigen-stimulated expanded B-cell population. Unlike base substitutions or gene deletions, changes in DNA methylation are potentially reversible. A hypomethylating agent, 5-aza-2′-deoxycytidine (decitabine) has been clinically useful in hematopoietic malignancies.49, 50 The role of the agent in the tumor therapy remains to be determined or will have to be the subject of future studies.
In summary, we showed primary cutaneous marginal zone B-cell lymphomas from three geographical regions have common clinicopathological features as have been previously described. However, moderate or marked tissue eosinophilia was significantly frequent in the Asian cases. Borrelia infection and API2–MALT12 fusion, both of which have been implicated in the development of this tumor, were not detected in our series. Finally, we showed that methylation of DAPK and p16 genes was frequent in primary cutaneous marginal zone B-cell lymphoma cases at their initial presentation, and had no impact on progressive features of the tumor cases.
References
Willemze R, Jaffe ES, Burg G, et al. WHO–EORTC classification for cutaneous lymphomas. Blood 2005;105:3768–3785.
Kempf W, Burg G, Ralfkiaer E, et al. Cutaneous marginal zone B-cell lymphoma. In: LeBoit PE, Burg G, Weedon D, Sarasin A (eds). World Health Organization Classification of Tumours. Pathology and Genetics. Skin tumours. IARC Press: Lyon, 2006, pp 194–195.
Cho-Vega JH, Vega F, Rassidakis G, et al. Primary cutaneous marginal zone B-cell lymphoma. Am J Clin Pathol 2006;125:38–49.
Goodlad JR, Davidson MM, Hollowood K, et al. Primary cutaneous B-cell lymphoma and Borrelia burgdorferi infection in patients from the Highlands of Scotland. Am J Surg Pathol 2000;24:1279–1285.
Cerroni L, Zöchling N, Pütz B, et al. Infection by Borrelia burgdorferi and cutaneous B-cell lymphoma. J Cutan Pathol 1997;24:457–461.
Kutting B, Bonsmann G, Metze D, et al. Borrelia burgdorferi-associated primary cutaneous B cell lymphoma: complete clearing of skin lesions after antibiotic pulse therapy or intralesional injection of interferon alfa-2a. J Am Acad Dermatol 1997;36:311–314.
Roggero E, Zucca E, Mainetti C, et al. Eradication of Borrelia burgdorferi infection in primary marginal zone B-cell lymphoma of the skin. Hum Pathol 2000;31:263–268.
Wood GS, Kamath NV, Guitart J, et al. Absence of Borrelia burgdorferi DNA in cutaneous B-cell lymphomas from the United States. J Cutan Pathol 2001;28:502–507.
Li C, Inagaki H, Kuo TT, et al. Primary cutaneous marginal zone B-cell lymphoma: a molecular and clinicopathologic study of 24 Asian cases. Am J Surg Pathol 2003;27:1061–1069.
Inagaki H . Mucosa-associated lymphoid tissue lymphoma: molecular pathogenesis and clinicopathological significance. Pathol Int 2007;57:474–484.
Grønbaek K, Ralfkiaer E, Kalla J, et al. Infrequent somatic Fas mutations but no evidence of Bcl10 mutations or t(11;18) in primary cutaneous MALT-type lymphoma. J Pathol 2003;201:134–140.
Streubel B, Simonitsch-Klupp I, Müllauer L, et al. Variable frequencies of MALT lymphoma-associated genetic aberrations in MALT lymphomas of different sites. Leukemia 2004;18:1722–1726.
de la Fouchardiere A, Gazzo S, Balme B, et al. Cytogenetic and molecular analysis of 12 cases of primary cutaneous marginal zone lymphomas. Am J Dermatopathol 2006;28:287–292.
Wongchaowart NT, Kim B, Hsi ED, et al. t(14;18)(q32;q21) involving IGH and MALT1 is uncommon in cutaneous MALT lymphomas and primary cutaneous diffuse large B-cell lymphomas. J Cutan Pathol 2006;33:286–292.
Schreuder MI, Hoefnagel JJ, Jansen PM, et al. FISH analysis of MALT lymphoma-specific translocations and aneuploidy in primary cutaneous marginal zone lymphoma. J Pathol 2005;205:302–310.
Gallardo F, Bellosillo B, Espinet B, et al. Aberrant nuclear BCL10 expression and lack of t(11;18)(q21;q21) in primary cutaneous marginal zone B-cell lymphoma. Hum Pathol 2006;37:867–873.
Inagaki H, Nakamura T, Li C, et al. Gastric MALT lymphomas are divided into three groups based on responsiveness to Helicobacter pylori eradication and detection of API2–MALT1 fusion. Am J Surg Pathol 2004;28:1560–1567.
Inagaki H, Chan JK, Ng JW, et al. Primary thymic extranodal marginal-zone B-cell lymphoma of mucosa-associated lymphoid tissue type exhibits distinctive clinicopathological and molecular features. Am J Pathol 2002;160:1435–1443.
Inagaki H, Okabe M, Seto M, et al. API2–MALT1 fusion transcripts involved in mucosa-associated lymphoid tissue lymphoma: multiplex RT–PCR detection using formalin-fixed paraffin-embedded specimens. Am J Pathol 2001;158:699–706.
Okabe M, Inagaki H, Ohshima K, et al. API2–MALT1 fusion defines a distinctive clinicopathologic subtype in pulmonary extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue. Am J Pathol 2003;162:1113–1122.
Herman JG, Graff JR, Myöhänen S, et al. Methylation-specific PCR: a novel PCR assay for methylation status of CpG islands. Proc Natl Acad Sci USA 1996;93:9821–9826.
Hoefnagel JJ, Vermeer MH, Jansen PM, et al. Primary cutaneous marginal zone B-cell lymphoma: clinical and therapeutic features in 50 cases. Arch Dermatol 2005;141:1139–1145.
Baldassano MF, Bailey EM, Ferry JA, et al. Cutaneous lymphoid hyperplasia and cutaneous marginal zone lymphoma: comparison of morphologic and immunophenotypic features. Am J Surg Pathol 1999;23:88–96.
Asadullah K, Döcke WD, Volk HD, et al. Cytokines and cutaneous T-cell lymphomas. Exp Dermatol 1998;7:314–320.
Roufosse F, Cogan E, Goldman M . Lymphocytic variant hypereosinophilic syndromes. Immunol Allergy Clin North Am 2007;27:389–413.
von Wasielewski R, Seth S, Franklin J, et al. Tissue eosinophilia correlates strongly with poor prognosis in nodular sclerosing Hodgkin's disease, allowing for known prognostic factors. Blood 2000;1595:1207–1213.
Navarro-Román L, Medeiros LJ, Kingma DW, et al. Malignant lymphomas of B-cell lineage with marked tissue eosinophilia. A report of five cases. Am J Surg Pathol 1994;18:347–356.
Kuo TT, Shih LY, Chan HL . Kimura's disease. Involvement of regional lymph nodes and distinction from angiolymphoid hyperplasia with eosinophilia. Am J Surg Pathol 1988;12:843–854.
Abuel-Haija M, Hurford MT . Kimura disease. Arch Pathol Lab Med 2007;131:650–651.
Bogle MA, Riddle CC, Triana EM, et al. Primary cutaneous B-cell lymphoma. J Am Acad Dermatol 2005;53:479–484.
Liu H, Ye H, Dogan A, et al. T(11;18)(q21;q21) is associated with advanced mucosa-associated lymphoid tissue lymphoma that expresses nuclear BCL10. Blood 2001;98:1182–1187.
Tyler LN, Ai L, Zuo C, et al. Analysis of promoter hypermethylation of death-associated protein kinase and p16 tumor suppressor genes in actinic keratoses and squamous cell carcinomas of the skin. Mod Pathol 2003;16:660–664.
Deiss LP, Feinstein E, Berissi H, et al. Identification of a novel serine/threonine kinase and a novel 15-kD protein as potential mediators of the gamma interferon-induced cell death. Genes Dev 1995;9:15–30.
Cohen O, Feinstein E, Kimchi A . DAP-kinase is a Ca2+/calmodulin-dependent, cytoskeletal-associated protein kinase, with cell death-inducing functions that depend on its catalytic activity. EMBO J 1997;16:998–1008.
Cohen O, Inbal B, Kissil JL, et al. DAP-kinase participates in TNF-alpha- and Fas-induced apoptosis and its function requires the death domain. J Cell Biol 1999;146:141–148.
Inbal B, Cohen O, Polak-Charcon S, et al. DAP kinase links the control of apoptosis to metastasis. Nature 1997;390:180–184.
Serrano M, Hannon GJ, Beach D . A new regulatory motif in cell-cycle control causing specific inhibition of cyclin D/CDK4. Nature 1993;366:704–707.
Lukas J, Parry D, Aagaard L, et al. Retinoblastoma-protein-dependent cell-cycle inhibition by the tumour suppressor p16. Nature 1995;375:503–506.
Kamb A, Gruis NA, Weaver-Feldhaus J, et al. A cell cycle regulator potentially involved in genesis of many tumor types. Science 1994;264:436–440.
Pinyol M, Cobo F, Bea S, et al. p16 (INK4a) gene inactivation by deletions, mutations, and hypermethylation is associated with transformed and aggressive variants of non-Hodgkin's lymphomas. Blood 1998;91:2977–2984.
Villuendas R, Sanchez-Beato M, Martinez JC, et al. Loss of p16/INK4A protein expression in non-Hodgkin's lymphomas is a frequent finding associated with tumor progression. Am J Pathol 1998;153:887–897.
Mateos MV, Garcia-Sanz R, Lopez-Perez R, et al. Methylation is an inactivating mechanism of the p16 gene in multiple myeloma associated with high plasma cell proliferation and short survival. Br J Haematol 2002;118:1034–1040.
Gonzalez M, Mateos MV, Garcia-Sanz R, et al. De novo methylation of tumor suppressor gene p16/INK4a is a frequent finding in multiple myeloma patients at diagnosis. Leukemia 2000;14:183–187.
Guillerm G, Gyan E, Wolowiec D, et al. p16/INK4a and p15/INK4b gene methylation in plasma cells from monoclonal gammopathy of undetermined significance. Blood 2001;98:244–246.
Nakatsuka S, Takakuwa T, Tomita Y, et al. Role of hypermethylation of DAP-kinase CpG island in the development of thyroid lymphoma. Lab Invest 2000;80:1651–1655.
Katzenellenbogen RA, Baylin SB, Herman JG . Hypermethylation of the DAP-kinase CpG island is a common alteration in B-cell malignancies. Blood 1999;93:4347–4353.
Rossi D, Capello D, Gloghini A, et al. Aberrant promoter methylation of multiple genes throughout the clinico-pathologic spectrum of B-cell neoplasia. Haematologica 2004;89:154–164.
Takino H, Okabe M, Li C, et al. p16/INK4a gene methylation is a frequent finding in pulmonary MALT lymphomas at diagnosis. Mod Pathol 2005;18:1187–1192.
Momparler RL . Pharmacology of 5-aza-2′-deoxycytidine (decitabine). Semin Hematol 2005;42:S9–S16.
Jabbour E, Issa JP, Garcia-Manero G, et al. Evolution of decitabine development: accomplishments, ongoing investigations, and future strategies. Cancer 2008;112:2341–2351.
Acknowledgements
This work was supported in part by a Grant-in-Aid for Scientific Research (C) from Japan Society for the Promotion of Science.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure/conflict of interest
All the authors declared no competing interests.
Supplementary Information accompanies the paper on Modern Pathology website (http://www.nature.com/modpathol)
Supplementary information
Rights and permissions
About this article
Cite this article
Takino, H., Li, C., Hu, S. et al. Primary cutaneous marginal zone B-cell lymphoma: a molecular and clinicopathological study of cases from Asia, Germany, and the United States. Mod Pathol 21, 1517–1526 (2008). https://doi.org/10.1038/modpathol.2008.159
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2008.159
Keywords
This article is cited by
-
Update in Diagnosis and Management of Primary Cutaneous B-Cell Lymphomas
American Journal of Clinical Dermatology (2022)
-
Downregulation of miR-152 contributes to DNMT1-mediated silencing of SOCS3/SHP-1 in non-Hodgkin lymphoma
Cancer Gene Therapy (2019)
-
Ocular adnexal marginal zone lymphoma of mucosa-associated lymphoid tissue
Clinical and Experimental Medicine (2018)
-
The Role of Infectious Agents, Antibiotics, and Antiviral Therapy in the Treatment of Extranodal Marginal Zone Lymphoma and Other Low-Grade Lymphomas
Current Treatment Options in Oncology (2015)
-
Primary cutaneous marginal zone lymphomas with plasmacytic differentiation show frequent IgG4 expression
Modern Pathology (2013)
