
Abstract
Bordetella pertussis causes whooping cough, an infectious disease of the respiratory tract that is re-emerging despite high vaccine coverage. Here we examined the role of Toll-like receptor (TLR) adapter protein Mal in the control of B. pertussis infection in the lungs. We found that B. pertussis bacterial load in the lungs of Mal-defective (Mal−/−) mice exceeded that of wild-type (WT) mice by up to 100-fold and bacteria disseminated to the liver in Mal−/− mice and 50% of these mice died from the infection. Macrophages from Mal−/− mice were defective in an early burst of pro-inflammatory cytokine production and in their ability to kill or constrain intracellular growth of B. pertussis. Importantly, the B. pertussis bacterial load in the lungs inversely correlated with the number of alveolar macrophages. Despite the maintenance and expansion of other cell populations, alveolar macrophages were completely depleted from the lungs of infected Mal−/− mice, but not from infected WT mice. Our findings define for the first time a role for a microbial pattern-recognition pathway in the survival of alveolar macrophages and uncover a mechanism of macrophage-mediated immunity to B. pertussis in which Mal controls intracellular survival and dissemination of bacteria from the lungs.
Similar content being viewed by others


INTRODUCTION
The incidence of pulmonary infection with Bordetella pertussis, the causative agent of whooping cough (pertussis), is increasing in many developed nations. Despite the introduction of whole-cell and acellular pertussis vaccines, the WHO (World Health Organization) estimated that in 2008 there were 16 million cases of B. pertussis infection, causing nearly 200,000 infant fatalities, mostly in developing countries.1 The recent resurgence of B. pertussis has been attributed to waning immunity or a failure of current acellular pertussis vaccines, which are composed of purified B. pertussis antigens absorbed to alum, to induce appropriate immune responses required for optimal immunity, in particular interferon-γ (IFN-γ)-secreting T helper type 1 cells.2 Studies in baboons and mice have suggested that these vaccines are not capable of inducing sterilizing immunity and consequently fail to prevent transmission from infected immunized to nonimmunized individuals.3, 4 Therefore, further investigation of the pathogenesis of B. pertussis infection is required to enable the rational design of vaccines that confer long-term sterilizing immunity.
B. pertussis expresses a number of virulence factors, some of which function as pathogen-associated molecular patterns and others that are putative protective antigens and components of acellular pertussis vaccines. B. pertussis lipooligosaccharide is a variant of the Toll-like receptor 4 (TLR4) agonist, lipopolysaccharide,5 and plays a crucial role in innate and adaptive immunity to B. pertussis.6, 7, 8 MyD88 adaptor-like protein (Mal; also known as TIRAP) is an important TIR domain-containing TLR adaptor that bridges TLR4 (and TLR2) with the central signaling adaptor MyD88 to mediate transcriptional activation of antibacterial and immunomodulatory genes, including those encoding pro-inflammatory cytokines and others involved in macrophage activation.9, 10, 11
A single-nucleotide polymorphism in the genes encoding MAL/TIRAP (TIRAP S180L) is associated with susceptibility to a number of pathogens, including Mycobacterium tuberculosis,12, 13 Streptococcus pneumoniae,12 Trypanasoma cruzi,14 Plasmodium falciparum,12 and HIV.15 Furthermore, studies in mice have indicated that Mal is more complicated than a simple MyD88-bridging adaptor.16 Apart from the core functional binding sites for MyD88,17 TLR4,17 TRAF6,18 PIP2,19 and IRAKs,20 Mal has binding sites for SOCS-1,21 Btk,22 and caspase-1.23 Mal is thought to be able to signal independently of MyD88, and has been reported to localize to both the plasma and endosomal membranes and thereby function as a “promiscuous” sorting adaptor that can be involved in sensing of viral nucleic acids.24
C3H/HeJ mice, which have defective TLR4, are more susceptible to B. pertussis infection of the lungs than TLR4-sufficient C3H/HeN mice,6, 7, 8 suggesting that innate immune cells, including macrophages and dendritic cells (DCs), that express TLR4 and Mal might play a central role in protective immunity to B. pertussis. Indeed, we have shown that local CD11c+CD8α+CD103+ DCs protect against B. pertussis infection of the lungs by promoting the induction of T helper type 1 cells after migration to the draining lymph nodes.25 However, the protective function of alveolar macrophages is still unclear and the role of TLR adaptors in B. pertussis infection has not been studied. Mal has been shown to play a role in protection of mice against severe disease after infection of the lungs with Escherichia coli26 or Klebsiella pneumoniae;27 however, the cellular responses involved in this protection were not well characterized. Mal is also involved in intestinal epithelial barrier maintenance and immunity to Salmonella typhimurium.28
Alveolar macrophages that express TLRs, including TLR2 and TLR4, are thought to be involved in the initial response to bacterial infection of the lungs by activating innate antibacterial and subsequent adaptive immune responses.29 Furthermore, B. pertussis has been detected inside human and mouse alveolar macrophages,30, 31 indicating that either phagocytosis by these cells is instrumental in the host immune response or alveolar macrophages can be hijacked by B. pertussis as a microbial mechanism of immuno-avoidance.
In this study, we have examined the role of Mal in the innate and adaptive immune responses and in the susceptibility of mice to B. pertussis infection. We demonstrated exacerbated, disseminating infection, often with a lethal outcome, in Mal-defective (Mal−/−) mice that was associated with defects in early inflammatory responses, increased numbers of intracellular B. pertussis, and increased cell death in alveolar macrophages. Our findings identify an important role for macrophages in controlling infection and demonstrate a critical role for Mal in their homeostasis and activation to kill intracellular bacteria, and thereby identify Mal as a major mediator of innate immune protection against B. pertussis.
RESULTS
A key role for Mal in controlling B. pertussis infection and preventing lethality
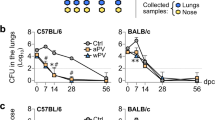
To assess the role of Mal in colonization of the lungs with B. pertussis, the kinetics of bacterial growth in wild-type (WT) and Mal−/− mice was examined by quantifying viable B. pertussis colony-forming units (CFUs) at various times after aerosol challenge with live B. pertussis. More than 104 CFUs were detected in the lungs of WT and Mal−/− mice 2 h after B. pertussis challenge and this had increased after 24 h in both genotypes (Figure 1a). However, on day 4 of infection, the bacterial load in the Mal−/− mice was >10-fold higher than in WT mice (P<0.01). The peak of lung bacterial load in both genotypes was evident at 7 days after challenge, but there were almost 40-fold more bacteria in the lungs of Mal−/− mice compared with WT mice (P<0.01). At 14 days after infection, the bacterial load in the lungs of WT mice had started to decline, suggesting that WT host immune responses were active in clearing bacteria. In contrast, the bacterial load persisted at a high level (∼107 CFUs) in the lungs of Mal−/− mice and was ∼100-fold higher than in WT mice (P<0.001), indicative of a failure of Mal−/− mice to control the infection. Consistent with this observation, 45% of Mal−/− mice died between days 14 and 21, whereas 100% of WT mice survived the infection (Figure 1b).

Enhanced bactrial load and lethality in Bordetella pertussis-infected MyD88 adaptor-like (Mal)-defective (Mal−/−) mice. Wild-type (WT) and Mal−/− mice were exposed to an aerosol of live B. pertussis (1 × 109 per ml). (a) B. pertussis colony-forming units (CFUs) in the lungs were enumerated at various times after challenge. Data are the mean±s.e.m. for four mice per group at each time point and are representative of three independent experiments. **P<0.01 and ***P<0.001 by two-way analysis of variance (ANOVA) with Bonferroni test. (b) Mice were checked daily for severe morbidity or mortality and survival percentage was plotted over the course of 6 weeks. Data are pooled from three independant experiments. Log-rank test confirmed that survival curves for WT and Mal−/− mice were significantly different. (c) Photomicrographs illustrating the earlier development and more severe nature of pulmonary inflammation in Mal−/− relative to WT mice. Note inflammatory infiltration of admixed neutrophils and macrophages at bronchoalveolar junction with attendant focal breakdown of lung parenchyma at day 4 (d4) after infection in Mal−/− mice. Whereas inflammation is lymphoplasmacytic and largely confined to perivascular/periairway locations in WT mice by day 14 (d14) after infection, in Mal−/− mice there is extensive, severe flooding of contiguous alveoli by cellular (neutrophils and macrophages) and proteinaceous exudate. Hematoxylin and eosin stain. Scale bar=50 μm.
The exacerbated course of infection and fatalities in B. pertussis-infected Mal−/− mice suggest that Mal is critical for the innate immune response to B. pertussis, perhaps by controlling inflammation. Therefore, we carried out histological examination of the lungs from infected mice. Pulmonary histology of uninfected WT and Mal−/− mice indicated no morphological abnormalities (data not shown). Alveolar wall thickening was evident 24 h after B. pertussis infection, but limited inflammation was observed in Mal−/− or WT mice (data not shown). However, 4 days after B. pertussis infection, substantial foci of inflammation were noted at the bronchoalveolar junctions of Mal−/− mice, but little equivalent inflammation in the lungs of WT mice (Figure 1c). Perivascular cuffing and infiltration of alveoli with neutrophils and macrophages was evident in the lungs of Mal−/− mice. Inflammation was also observed in the lungs of B. pertussis-infected WT mice 7 days after challenge, but this was resolving by day 14 (Figure 1c). In contrast, pulmonary inflammation did not resolve in Mal−/− mice, with persistence of extensive cellular and proteinaceous exudate indicating alveolar wall injury, along with pleurisy (Figure 1c), all predictive of poor clinical outcome. Our findings demonstrate that Mal is critical for controlling a primary infection with B. pertussis and the associated pulmonary inflammation.
Disseminating infection and inflammation in B. pertussis-infected Mal−/− mice
We had previously observed that deaths from B. pertussis in immunocompromised mice were associated with organ failure because of bacterial dissemination from the lungs to other organs, especially the liver.32, 33 Therefore, we quantified CFUs from the livers of B. pertussis-infected Mal−/− and WT mice. B. pertussis CFUs were not detected in the livers of infected WT mice, but 7 and 14 days after infection 4,000–5,000 CFUs were detected per liver lobe in Mal−/− mice (Figure 2a). These findings indicate that Mal-dependent host immune responses control bacterial growth in the lungs and prevent dissemination and lethal infection with B. pertussis.

Dissemination of Bordetella pertussis and inflammatory pathology in the liver of MyD88 adaptor-like (Mal)-defective (Mal−/−) mice. Wild-type (WT) and Mal−/− mice were infected with B. pertussis as described in Figure 1. (a) At various times after infection, colony-forming units (CFUs) were enumerated in homogenized liver. Data are mean±s.d. (n ≥3 mice) from one experiment that is representative from three independant experiments. ***P<0.001 by two-way analysis of variance (ANOVA) with Bonferroni test. (b) High-magnification photomicrographs illustrating one of the multifocal inflammatory infiltrates (subtle aggregates of admixed neutrophils and macrophages) in the liver of Mal−/− mice, and the absence of such inflammation in WT mice, by day 14 after infection. Hematoxylin and eosin stain. Scale bar=25 μm.
Histopathology showed inflammatory foci in the livers of Mal−/− mice 7 days after B. pertussis infection and the number of these foci had increased 14 days after infection (Figure 2b). These foci consisted of dense aggregates of neutrophils and macrophages, and were not detected in livers from uninfected mice or from B. pertussis-infected WT mice. These data are consistent with the dissemination of B. pertussis from the primary site of infection in the lungs of Mal−/− mice to the liver, where they cause substantial, and potentially lethal, pathology.
Mal is required for a burst of early innate pro-inflammatory cytokines in response to B. pertussis infection
Having demonstrated enhanced inflammatory pathology in the lungs of B. pertussis-infected Mal−/− mice, we examined local inflammatory cytokine production in the lungs. A transient peak of the inflammatory cytokines and chemokines interleukin (IL)-1β, tumor necrosis factor (TNF), macrophage inflammatory protein (MIP)-1α, and MIP-2α, typically produced by innate immune cells including macrophages and DCs, was detected in the lungs of WT mice 2 h after challenge with B. pertussis (Figure 3). Importantly, and despite equivalent bacterial numbers in the lungs at this time, the early burst of IL-1β, TNF, MIP-1α, and MIP-2α production was either substantially muted or was entirely defective in the lungs of Mal−/− mice (Figure 3). More than sixfold more IL-1β (P<0.001), twofold more TNF (P<0.05), 2.5-fold more MIP-1α (P<0.001), and 10-fold more MIP-2α (P<0.001) were detected in the lungs of WT mice than in the lungs of Mal−/− mice at 2 h after challenge. These cytokines had returned to baseline 24 h after infection. However, at later stages of infection (≥4 days), the concentration of these pro-inflammatory cytokines was much higher in the lungs of Mal−/− mice when compared with WT mice (P<0.001). Typical T cell-associated cytokines, IL-17A, IL-17F, and IFN-γ, were barely detected at early stages of infection, but were increased in the lungs 7–14 days after B. pertussis infection, with much higher concentrations in Mal−/− than in WT mice (Figure 3). Interestingly, IL-10 concentrations were not significantly different in WT and Mal−/− mice. These findings indicate that Mal is required for optimal pro-inflammatory cytokine production by lung-resident cells in immediate response to B. pertussis infection. In contrast, higher local inflammatory responses detected in Mal−/− mice later in infection might reflect the higher bacterial load in the lungs of these mice. However, when WT and Mal−/− mice had a lower initial B. pertussis burden in the lungs, we detected the same differences in inflammatory responses as that seen in mice with higher bacterial loads (data not shown).

MyD88 adaptor-like (Mal) is required for early innate cytokine responses to Bordetella pertussis infection. Wild-type (WT) and Mal-defective (Mal−/−) mice were aerosol infected with B. pertussis. At various times after infection, lung lobes were homogenized and cytokine concentrations were quantified by enzyme-linked immunosorbent assay (ELISAs). Data are mean±s.e.m. (n=3 mice) from one experiment that is representative of three independent experiments. *P<0.05, **P<0.01, and ***P<0.001 by two-way analysis of variance (ANOVA) with Bonferroni test. IFN-γ, interferon-γ; IL, interleukin; MIP, macrophage inflammatory protein; TNF, tumor necrosis factor.
Enhanced infiltration of IL-17- and IFN-γ-producing T cells in the lungs of Mal−/− mice
In order to examine the possible role of T cells and the influence of Mal-driven innate immune responses on adaptive immunity to B. pertussis, we examined T-cell infiltration and cytokine production in the lungs of infected mice by intracellular staining and flow cytometry analysis. Lung-infiltrating leukocytes, including CD4+ T cells and γδ T cells, were evident in WT mice on days 14–21 of infection and this number was significantly greater in Mal−/− mice (Figure 4). There were up to 10-fold more leukocytes, CD4+ T cells, and γδ T cells in Mal−/− compared with WT mice at the peak of cellular infiltration on day 14 (P<0.001). Intracellular cytokine staining and fluorescence-activated cell sorting (FACS) analysis showed that there were significantly more IFN-γ-producing CD4+ T cells and γδ T cells in the lungs of Mal−/− mice than in WT mice 14 days after infection (P<0.001; Figure 4). The number of IL-17A-producing CD4+ T cells and γδ T cells was also higher, although not significantly, in the lungs of Mal−/− mice than in the WT mice (Figure 4). These finding are consistent with those in Figure 3, demonstrating enhanced inflammatory responses in the lungs of Mal−/− mice at the peak of infection.

Enhanced infiltrating T helper type 1 (Th1) and T helper type 17 (Th17) cells in the lungs in the late stages of Bordetella pertussis infection of MyD88 adaptor-like (Mal)-defective (Mal−/−) mice. Wild-type (WT) and Mal−/− mice were aerosol infected with B. pertussis. At various times after infection, lung mononuclear cells were prepared. Cells were permeabilized and fixed for intracellular cytokine staining and fluorescence-activated cell sorting (FACS) analysis. Cells were stained for surface CD3, CD4, and T cell receptor-δ (TCRδ), and for intracellular interferon-γ (IFN-γ) and interleukin-17 (IL-17). Data are mean±s.e.m. (n=3 mice) from one experiment that is representative of three separate experiments. ***P<0.001, statistical analysis by two-way analysis of variance (ANOVA) with Bonferroni test.
Alveolar macrophages are depleted in the lungs of Mal−/− mice after infection with B. pertussis
Our results so far have indicated that Mal regulates inflammatory responses at the peak of infection, possibly indirectly by modulating the early innate immune responses that control the growth of B. pertussis in the lungs. However, we also found that Mal is required for an early burst of the pro-inflammatory cytokines IL-1β, TNF, MIP-1α, and MIP-2α. Therefore, we examined the possible role of lung-resident innate immune cells in controlling the early infection with B. pertussis. Alveolar macrophages, which are known to produce IL-1β and TNF, are present principally in the alveolar spaces and are the main resident cell type in the uninfected lung. Alveolar macrophages were the dominant cell type in bronchoalveolar lavage fluid (BAL-F) from uninfected mice, with a smaller number of neutrophils, monocytes, and DCs (data not shown). After aerosol challenge with B. pertussis, Ly6G+Ly6C+ neutrophils were detected in the lungs of WT mice by day 7 and this peaked at day 14 (Figure 5a). However, in Mal−/− mice, infiltration of these cells was detected after 24 h and was more pronounced. Similarly, the numbers of inflammatory monocytes and infiltrating macrophages were significantly greater in Mal−/− compared with WT mice (Figure 5a). In contrast, there was a striking reduction in the percentage and absolute numbers of resident alveolar macrophages in Mal−/− mice within 4 days of B. pertussis challenge, and these cells were completely depleted by day 14, whereas the number of alveolar macrophages increased during the course of B. pertussis infection of WT mice (Figure 5a,b).

Enhanced recruitment of neutrophils and inflammatory monocytes, but depletion of alveolar macrophages, in Bordetella pertussis-infected MyD88 adaptor-like (Mal)-defective (Mal−/−) mice. Wild-type (WT) and Mal−/− mice were aerosol challenged with B. pertussis. Bronchoalveolar lavage fluid (BAL-F) was taken from mice and analyzed by fluorescence-activated cell sorting (FACS) for various cell subsets. (a) Data are mean±s.e.m. (n=3 mice) from one experiment that is representative of three separate experiments. (b) Representative FACS plots for alveolar macrophages. *P<0.05, **P<0.01 and ***P<0.001 by two-way analysis of variance (ANOVA) with Bonferroni test.
Apoptosis-induced cell death of alveolar macrophages in B. pertussis-infected Mal−/− mice
We have shown that B. pertussis can disseminate from the lungs and infect the livers of Mal−/− mice. Furthermore, the disappearance of alveolar macrophages from the lungs of B. pertussis-infected Mal−/− mice might result from emigration of these cells from the lungs or local killing of alveolar macrophages after severe infection with B. pertussis. We first analyzed lung-draining mediastinal lymph nodes and blood for disseminating alveolar macrophages by FACS. A small population of autofluorescent MHC IIintCD11b+F4/80+CD11c−Ly6G−Siglec-F+B220−CD3− cells, characteristic of alveolar macrophages, was detected in the lymph nodes of uninfected WT and Mal−/− mice (Figure 6a,b). This number increased significantly 3 and 7 days after B. pertussis infection in both genotypes, but the increase was significantly greater (P<0.01) in WT (∼3% at day 3 and ∼5% at day 7) than in Mal−/− mice (∼0.4% at day 3 and ∼0.8% at day 7). Consistent with this result, cells with an alveolar macrophage phenotype were also detected in the blood 7 days after B. pertussis infection (data not shown). These data indicate that alveolar macrophages emigrate from the lungs during B. pertussis infection, but this is less pronounced in Mal−/− mice, suggesting that other mechanisms might account for the total disappearance of alveolar macrophages from the lungs of infected Mal−/− mice.

Reduced migration and increased apoptotic cell death of alveolar macrophages in Bordetella pertussis-infected MyD88 adaptor-like (Mal)-defective (Mal−/−) mice. Wild-type (WT) and Mal−/− mice were exposed to a 20-min aerosol challenge with 1 × 109 B. pertussis per ml. At various times after infection, mediastinal lymph nodes were analyzed by fluorescence-activated cell sorting (FACS) for alveolar macrophages. Data are mean values for 6 mice per group (a) with sample FACS plots (b) and are representative of two experiments. **P<0.01, statistical analysis by two-way analysis of variance (ANOVA) with Bonferroni test. (c) At various times after infection, bronchoalveolar lavage fluid (BAL-F) was analyzed by FACS for LIVE/DEAD Aqua-positive and Annexin V-positive alveolar macrophages. Data are mean (n=3 mice) from one experiment that is representative of two independent experiments.
We next examined the possibility that cell death accounts for the disappearance of alveolar macrophages in the lungs of Mal−/− during B. pertussis infection. We performed flow cytometry analysis using LIVE/DEAD Aqua as a measure of cell death and Annexin V as a measure of apoptosis. Over the course of B. pertussis infection, the percentage of apoptotic alveolar macrophages increased in WT and Mal−/− mice (Figure 6c). However, the percentage increase was greater in the Mal−/− mice than the WT mice. This difference was evident throughout the course of the infection, as early as 24 h (Mal−/− ∼20%; WT ∼6%), but was most substantial 7 days after infection (Mal−/− ∼38%; WT ∼13%). Most apoptotic cells were identified as “early apoptotic” (LIVE/DEAD negative, Annexin V positive). These data suggest that cell death might account for depletion of alveolar macrophages from the lungs of B. pertussis-infected Mal−/− mice, but do not exclude other mechanisms.
Pro-inflammatory cytokine production and a reduction in numbers of intracellular B. pertussis in macrophages is dependent on Mal
Our findings suggest that Mal might mediate an early innate inflammatory response to B. pertussis infection in the lungs, but surprisingly might also be involved in survival or sequestration of alveolar macrophages in the lungs. To better understand the function of Mal-dependent responses in macrophages, we examined its role in inflammatory cytokine production and bacterial killing after in vitro infection of macrophages with B. pertussis. We first used bone marrow-derived macrophages (BMDMs) to optimize the assays, before moving on to ex vivo alveolar macrophages, where cell numbers are a limitation to extensive experiments. We found that B. pertussis infection of BMDMs from WT mice induced production of significantly higher concentrations of MIP-2α and TNF at 2 h after infection and significantly greater IL-1β at 24 h after infection (Figure 7a). These experiments were repeated over a narrower multiplicity of infection range using alveolar macrophages purified from BAL-F. These cells were large, autofluorescent CD11b−CD11c+Ly6G−F4/80+MHC-IIintSiglec-F+ cells with 95% purity by FACS analysis. B. pertussis infection of alveolar macrophages from WT mice resulted in a rapid production of pro-inflammatory cytokines and chemokines (MIP-2α, TNF, and IL-1β), similar to that seen with BMDMs. These responses were almost completely abrogated in B. pertussis-infected alveolar macrophages from Mal−/− mice (Figure 7b).

MyD88 adaptor-like (Mal) is required for early cytokine production and a reduction in Bordetella pertussis numbers in macrophages. (a) Bone marrow-derived macrophages (BMDMs) from wild-type (WT) and Mal-defective (Mal−/−) mice were co-cultured with live B. pertussis over a range of relative multiplicity of infection (MOI). After 2 or 24 h, supernatants were removed for quantification of cytokines by enzyme-linked immunosorbent assay (ELISA). Data are mean±s.e.m. (n=3 mice) from one representative experiment from three independant experiments. *P<0.05, **P<0.01, and ***P<0.001 by two-way analysis of variance (ANOVA) with Bonferroni test. (b) Alveolar macrophages from WT or Mal−/− mice (n=10) were pooled to obtain suffient cells for the assays and co-cultured with live B. pertussis for 2 or 24 h. Supernatants were removed for quantification of cytokines by ELISA. Data are representative of two separate experiments. (c) BMDMs from WT and Mal−/− mice were infected with B. pertussis. At 2 or 24 h after infection, supernatants were removed and cell monolayers were washed three times and then lysed and plated onto BG blood agar for colony-forming unit (CFU) enumeration. Data are mean ±s.d. (n ≥3) from one experiment that is representative of three separate experiments.
We next examined the role of Mal in survival of B. pertussis in macrophages. BMDMs were infected with B. pertussis, and after 2 h were washed to remove extracellular bacteria, and were cultured for a further 2 or 24 h, then lysed to estimate intracellular bacterial load by quantifying CFUs. The number of CFUs was dependent on the multiplicity of infection, indicating that B. pertussis had invaded the macrophages from WT and Mal−/− mice and there was no significant difference in the number of CFUs between the genotypes 2 h after infection (Figure 7c). However, 24 h after B. pertussis infection, there were approximately fourfold more intracellular bacteria in macrophages from Mal−/− compared with WT mice (P<0.001). Over the course of the 24 h assay, B. pertussis proliferated fourfold inside WT macrophages and 10-fold inside macrophages from Mal−/− mice. These data suggest that Mal plays a significant role in inflammatory cytokine production by B. pertussis-infected macrophages and in limiting the growth of intracellular B. pertussis in macrophages.
DISCUSSION
This study describes for the first time a critical role for the TLR2/4 adapter protein Mal in the pathogenesis of B. pertussis infection in mice. Our findings demonstrate that mice defective in this innate signaling molecule are unable to control the infection; the bacteria multiply more rapidly in macrophages and disseminate out of the lungs to the liver, resulting in lethality in nearly 50% of mice. We have shown that Mal plays a role in the early local innate burst of pro-inflammatory cytokines by alveolar macrophages in the lungs and importantly in preventing apoptosis-induced cell death and depletion of alveolar macrophages from the lungs of B. pertussis-infected mice.
B. pertussis infection of immunocompetent mice and humans is normally confined to the lungs and upper respiratory tract. However, viable B. pertussis has been cultured from the livers and blood of airway-infected IFN-γ receptor-defective mice32 and in mice depleted of natural killer cells.33 As natural killer cells produce IFN-γ, these studies suggested that early IFN-γ might be required to activate intracellular killing of B. pertussis by macrophages.34 IFN-γ is known to activate nitric oxide that is involved in killing intracellular bacteria, including B. pertussis.35 The findings of the current study, showing intracellular survival of B. pertussis in macrophages and dissemination of bacteria from the lungs, is consistent with these reports. However, our current study suggests that activation of TLR pathways that utilize the Mal adapter molecule might also play a critical role in activating intracellular killing or preventing survival of B. pertussis in macrophages.
We found that an early burst of pro-inflammatory cytokines and chemokines, including TNF, IL-1β, and MIP-2α, produced by B. pertussis-infected macrophages in vitro and in the lungs of B. pertussis-infected mice was significantly reduced or abrogated in the absence of Mal. Furthermore, apoptosis-induced cell death in alveolar macrophages, which might be linked to a greater intracellular bacterial load, was exacerbated in B. pertussis-infected Mal−/− mice. It has previously been reported that B. pertussis induces apoptosis of macrophages in vitro and of alveolar macrophages in the lungs of B. pertussis-infected mice through the activity of adenylate cyclase/hemolysin.36, 37 Consistent with these findings, we found evidence of alveolar macrophage apoptosis in WT mice infected with B. pertussis, but the alveolar macrophage apoptosis was significantly greater in Mal−/− mice, suggesting that although adenylate cyclase/hemolysin might induce apoptosis, this may be partly restrained by Mal-mediated signals from TLR2 or TLR4 ligands produced by B. pertussis. Interestingly, TLR4 signaling through Mal has been reported to have an important role in protection against alveolar cell apoptosis.38
Our findings indicate that an optimal alveolar macrophage effector function is vital for prevention of disseminating infection and lethality from B. pertussis. Dissemination of live bacteria inside macrophages, a type of “Trojan horse” phenomenon, has been documented for Bacillus anthracis.39 Bacterial dissemination, inside mouse DCs, has also been observed with S. pneumoniae,40 a bacterial species for which susceptibility is associated with the TIRAP S180L single-nucleotide polymorphism.12 Although we found live bacteria in the liver of Mal−/− mice and enhanced B. pertussis survival in macrophages, the migration of alveolar macrophages to the blood and lymph node was less pronounced in Mal−/− mice compared with WT mice. In contrast, we did find evidence of enhanced programmed cell death of alveolar macrophages in the infected lungs of Mal−/− mice. Together, these data suggest that Mal signaling compromises bacterial growth or enables optimal intracellular killing of B. pertussis by alveolar macrophages, minimizing the survival of bacteria in the lungs and thereby preventing both alveolar macrophage apoptosis and live B. pertussis from disseminating from the lungs inside emigrant cells. Previous studies have identified a critical role for alveolar macrophages in limiting susceptibility to lung bacterial infection; the risk of secondary bacterial pneumonia after influenza infection has been attributed to virus-induced depletion of alveolar macrophages.41 However, a possible alternative explanation for the dissemination of B. pertussis out of the lungs of Mal−/− mice is that the lung epithelial barrier in these mice might have been compromised. Mal has been implicated in the maintenance of the intestinal barrier and in resistance to S. enterica serovar Typhimurium.28 Our histology analysis showed substantial pleurisy and cellular and proteinaceous exudate in the lungs of infected Mal−/− mice but not in infected WT mice.
Polymorphism analyses in humans have demonstrated that TIRAP S180L mutation is associated with increased susceptibility to infection with M. tuberculosis and S. pneumoniae.12, 13 However, it has also been reported that the TIRAP C539T polymorphism significantly correlated with a reduced risk of M. tuberculosis infection.42 We have previously demonstrated an exacerbated lung bacterial load in B. pertussis-infected and TLR4-defective C3H/HeJ mice.7 Although these mice had exacerbated pulmonary inflammation, we did not observe bacterial dissemination or deaths from the infection, suggesting that Mal might mediate some of its effects in our infection model independently of TLR4. Interesting, we have recently identified a number of novel TLR2 lipoprotein agonists produced by B. pertussis.43 Therefore, TLR2 might also have a critical role in macrophage activation and protective immunity to B. pertussis.
We have shown that Mal is essential for anti-B. pertussis macrophage effector functions that prevent fatality. Optimal pro-inflammatory cytokine production and a reduction in bacterial numbers in macrophages, as well as the maintenance of the resident alveolar macrophage population, were dependent on Mal. We believe that this Mal-dependent homeostasis requires intracellular killing of B. pertussis that prevents the death or apoptosis of alveolar macrophages. Our data also suggest that Mal might be vital in the prevention of emigrant alveolar macrophages carrying live B. pertussis out of the lungs and disseminating the infection. Therefore, Mal appears to be a critical regulator of alveolar macrophage-mediated protection against B. pertussis infection.
METHODS
Mice. Female specific pathogen-free C57BL/6 and Mal−/− mice on a C57BL/6 background11 were bred in-house. Mice were 7–12 weeks old and age matched at the beginning of experiments. Mice were killed by cervical dislocation or asphyxiation with CO2. All animal experiments were conducted in accordance with the recommendations and guidelines of the HPRA (Health Products Regulatory Authority), the competent authority in Ireland responsible for the implementation of Directive 2010/63/EU on the protection of animals used for scientific purposes in accordance with the requirements of the S.I No 543 of 2012. Trinity College Dublin is an authorized breeder, user, and supplier of laboratory animals (HPRA Establishment Authorization Number: AE19136). Animal experiments were carried out under license (B100/2412) approved by the HPRA and in accordance with protocols approved by Trinity College Dublin Animal Research Ethics Committee.
B. pertussis infection. Respiratory infection of mice was performed by exposure to an aerosol of B. pertussis (strain Tohama 1; 1 × 109/ml) for 15 min as previously described.44 The course of B. pertussis infection was followed by counting CFUs from lungs and livers from groups of 4–5 mice at intervals after challenge. The lungs and livers were aseptically removed and homogenized in 1 ml of sterile physiological saline with 1% casein on ice. Undiluted and serially diluted homogenate (100 μl) from individual lungs or individual liver lobes was spotted in triplicate onto Bordet–Gengou agar plates, and the number of CFUs was calculated after 5 days of incubation at 37 °C.
Enzyme-linked immunosorbent assay. Lung homogenates were diluted and used for detection of cytokines and chemokines by enzyme-linked immunosorbent assay (ELISA) duosets (R&D Systems, Minneapolis, MN). Phosphate-buffered saline (PBS) plus 0.1% Tween-20 was used as a wash buffer. H2SO4 at 0.16 M was used as a stop solution. Concentration was calculated by colorimetric change with horseradish peroxidase and TMB, relative to 1:10 dilution standards of purified cytokine according to the manufacturer’s instructions on a Versamax spectrophotometer (Molecular Devices, Sunnyvale, CA).
Lung cell isolation. BAL-F was isolated by inserting a cannula into the trachea of killed mice and injecting three 1 ml volumes of ice-cold PBS without rupturing the lungs. BAL-F was then centrifuged at 300 × g for 5 min. Cells were then resuspended in ice-cold PBS. Alternatively, disrupted lungs were cut into small pieces and then rotated for 30 min at 37 °C in RPMI containing Collagenase IV (Life Technologies, Carlsbad, CA), DNase I (Sigma-Aldrich, St Louis, MO), and Brefeldin A (BioLegend, San Diego, CA). Digested lung material was then passed through a 100 μm filter. Red blood cells were lysed and leukocytes were collected for analysis. BAL-F was incubated on plastic for 2 h to allow alveolar macrophages to adhere. Nonadherent cells were washed away and Flow cytometry analysis performed on scraped cells that were typically >95% pure, viable, large, autofluorescent CD11b−CD11c+Ly6G−F4/80+MHC-IIintSiglec-F+ cells.
Flow cytometry analysis. Cells (1 × 106 cells in 50 μl PBS) were stained with 0.5 μl Fc Block (anti-CD16, anti-CD32) and then surface stained with fluorescent-conjugated anti-mouse antibodies for various markers (CD49b, NK1.1, γδ-TCR, CD3, CD4, CD8, CD11b, F4/80, Ly6C, Ly6G, MHC II, Siglec-F, and CD11c; eBioscience, San Diego, CA) for 20 min on ice. Cells were incubated with 0.5 μl LIVE/DEAD Aqua (Invitrogen, Life Technologies) as per the manufacturer’s instructions and then centrifuged at 300 × g for 3 min in FACS tubes. For intracellular FACS analysis, cells were resuspended in Fix/Perm (eBioscience) for 20 min as per the manufacturer’s instructions. Antibodies for intracellular cytokines were added in permeabilization buffer (IFN-γ, IL-17A, IL-17F, IL-4, and IL-10). FMO (fluorescence minus one) and nonspecific isotype antibodies were used as controls. FACS samples were analyzed in 100 μl of FACS buffer or permeabilization buffer (eBioscience). Samples were calibrated with antibody-labeled single-stained microbeads and run on a FACSCalibur or FACSCanto 2 (BD, Franklin Lakes, NJ). Data were analyzed using FlowJo software (Ashland, OR), and plotted with GraphPad Prism (GraphPad Software Inc., La Jolla, CA).
In vitro infection of macrophages with B. pertussis. BMDMs were prepared from tibias and femurs of both back legs of mice. Bone marrow was flushed with a 3 ml syringe and 21-gauge needle into Dulbecco’s modified (Sigma-Aldrich) supplemented with 10% fetal calf serum. Red blood cells were lysed with RBC lysis buffer (0.829 g NH4Cl, 0.109 g KHCO3, 0.037 g disodium EDTA (Sigma-Aldrich), 100 ml H2O, pH 7.3–7.4) and remaining cells were washed and resuspended at a concentration of 1 × 106/ml in Dulbecco’s modified Eagle’s medium supplemented with 10% fetal calf serum and 20% macrophage colony-stimulating factor-containing L929 supernatant (L929, fibrosarcoma cell line was cultured at a density of 0.5 × 106/ml in Dulbecco’s modified Eagle’s medium for 7 days. The supernatant was harvested and filter sterilized. Then, 10 ml of cells were incubated in 10 cm non-tissue culture-treated dishes for 6 days. On day 6, supernatant was removed and 5 ml of ice-cold PBS was added to each dish. BMDMs were gently dislodged from the dish by scraping. Cells were counted and reseeded at a density of 0.5 × 106/ml and 2 ml per well on a 6-well dish and incubated overnight in Dulbecco’s modified Eagle’s medium and 10% fetal calf serum with L929. After 24 h, heat-killed B. pertussis or live B. pertussis was added and cultures were incubated for 2 or 24 h at 37 °C with 5% CO2. Cell culture supernatants were removed for cytokine enzyme-linked immunosorbent assay. BMDMs were then washed four times and then lysed in double-distilled H2O, and lysate was plated onto horse blood agar plates for 4 days to enumerate intracellular bacteria.
Histology. At least three lungs and livers were removed at various times after aerosol infection with B. pertussis and placed into 10% neutral-buffered formalin for tissue sectioning and hemotoxylin and eosin staining.
Statistical analysis. GraphPad Prism software was used for comparison of WT and Mal−/− mice by two-way analysis of variance with Bonferroni post-tests, or log-rank tests for statistical significance (as marked in figure legends).
References
Black, R.E. et al. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet 375, 1969–1987 (2010).
Mills, K.H., Ross, P.J., Allen, A.C. & Wilk, M.M. Do we need a new vaccine to control the re-emergence of pertussis? Trends Microbiol. 22, 49–52 (2014).
Warfel, J.M., Zimmerman, L.I. & Merkel, T.J. Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model. Proc. Natl. Acad. Sci. USA 111, 787–792 (2014).
Smallridge, W.E., Rolin, O.Y., Jacobs, N.T. & Harvill, E.T. Different effects of whole-cell and acellular vaccines on Bordetella transmission. J. Infect. Dis. 209, 1981–1988 (2014).
Peppler, M.S. Two physically and serologically distinct lipopolysaccharide profiles in strains of Bordetella pertussis and their phenotype variants. Infect. Immun. 43, 224–232 (1984).
Higgins, S.C., Jarnicki, A.G., Lavelle, E.C. & Mills, K.H. TLR4 mediates vaccine-induced protective cellular immunity to Bordetella pertussis: role of IL-17-producing T cells. J. Immunol. 177, 7980–7989 (2006).
Higgins, S.C. et al. Toll-like receptor 4-mediated innate IL-10 activates antigen-specific regulatory T cells and confers resistance to Bordetella pertussis by inhibiting inflammatory pathology. J. Immunol. 171, 3119–3127 (2003).
Mann, P.B., Kennett, M.J. & Harvill, E.T. Toll-like receptor 4 is critical to innate host defense in a murine model of bordetellosis. J. Infect. Dis. 189, 833–836 (2004).
Fitzgerald, K.A. et al. Mal (MyD88-adapter-like) is required for Toll-like receptor-4 signal transduction. Nature 413, 78–83 (2001).
Horng, T., Barton, G.M., Flavell, R.A. & Medzhitov, R. The adaptor molecule TIRAP provides signalling specificity for Toll-like receptors. Nature 420, 329–333 (2002).
Yamamoto, M. et al. Essential role for TIRAP in activation of the signalling cascade shared by TLR2 and TLR4. Nature 420, 324–329 (2002).
Khor, C.C. et al. A Mal functional variant is associated with protection against invasive pneumococcal disease, bacteremia, malaria and tuberculosis. Nat. Genet. 39, 523–528 (2007).
Castiblanco, J. et al. TIRAP (MAL) S180L polymorphism is a common protective factor against developing tuberculosis and systemic lupus erythematosus. Infect. Genet. Evol. 8, 541–544 (2008).
Ramasawmy, R. et al. Heterozygosity for the S180L variant of MAL/TIRAP, a gene expressing an adaptor protein in the Toll-like receptor pathway, is associated with lower risk of developing chronic Chagas cardiomyopathy. J. Infect. Dis. 199, 1838–1845 (2009).
Papadopoulos, A.I. et al. Association of Mal/TIRAP S180L variant polymorphism with decreased infection risk in patients with advanced HIV-1 infection. Cytokine 60, 104–107 (2012).
Bernard, N.J. & O'Neill, L.A. Mal, more than a bridge to MyD88. IUBMB Life 65, 777–786 (2013).
Bovijn, C. et al. Identification of binding sites for myeloid differentiation primary response gene 88 (MyD88) and Toll-like receptor 4 in MyD88 adapter-like (Mal). J. Biol. Chem. 288, 12054–12066 (2013).
Mansell, A., Brint, E., Gould, J.A., O'Neill, L.A. & Hertzog, P.J. Mal interacts with tumor necrosis factor receptor-associated factor (TRAF)-6 to mediate NF-kappaB activation by toll-like receptor (TLR)-2 and TLR4. J. Biol. Chem. 279, 37227–37230 (2004).
Kagan, J.C. & Medzhitov, R. Phosphoinositide-mediated adaptor recruitment controls Toll-like receptor signaling. Cell 125, 943–955 (2006).
Dunne, A. et al. IRAK1 and IRAK4 promote phosphorylation, ubiquitination, and degradation of MyD88 adaptor-like (Mal). J. Biol. Chem. 285, 18276–18282 (2010).
Mansell, A. et al. Suppressor of cytokine signaling 1 negatively regulates Toll-like receptor signaling by mediating Mal degradation. Nat. Immunol. 7, 148–155 (2006).
Gray, P. et al. MyD88 adapter-like (Mal) is phosphorylated by Bruton’s tyrosine kinase during TLR2 and TLR4 signal transduction. J. Biol. Chem. 281, 10489–10495 (2006).
Ulrichts, P. et al. Caspase-1 targets the TLR adaptor Mal at a crucial TIR-domain interaction site. J. Cell. Sci. 123, 256–265 (2010).
Bonham, K.S. et al. A promiscuous lipid-binding protein diversifies the subcellular sites of toll-like receptor signal transduction. Cell 156, 705–716 (2014).
Dunne, P.J., Moran, B., Cummins, R.C. & Mills, K.H. CD11c+CD8{alpha}+ dendritic cells promote protective immunity to respiratory infection with Bordetella pertussis. J. Immunol. 183, 400–410 (2009).
Jeyaseelan, S. et al. Toll-IL-1 receptor domain-containing adaptor protein is critical for early lung immune responses against Escherichia coli lipopolysaccharide and viable Escherichia coli. J. Immunol. 175, 7484–7495 (2005).
Jeyaseelan, S. et al. Toll/IL-1R domain-containing adaptor protein (TIRAP) is a critical mediator of antibacterial defense in the lung against Klebsiella pneumoniae but not Pseudomonas aeruginosa. J. Immunol. 177, 538–547 (2006).
Corr, S.C. et al. MyD88 adaptor-like (Mal) functions in the epithelial barrier and contributes to intestinal integrity via protein kinase C. Mucosal Immunol. 7, 57–67 (2014).
Kovach, M.A. & Standiford, T.J. Toll like receptors in diseases of the lung. Int. Immunopharmacol. 11, 1399–1406 (2011).
Friedman, R.L., Nordensson, K., Wilson, L., Akporiaye, E.T. & Yocum, D.E. Uptake and intracellular survival of Bordetella pertussis in human macrophages. Infect. Immun. 60, 4578–4585 (1992).
Vandebriel, R.J. et al. Association of Bordetella pertussis with host immune cells in the mouse lung. Microb. Pathog. 35, 19–29 (2003).
Mahon, B.P., Sheahan, B.J., Griffin, F., Murphy, G. & Mills, K.H. Atypical disease after Bordetella pertussis respiratory infection of mice with targeted disruptions of interferon-gamma receptor or immunoglobulin mu chain genes. J. Exp. Med. 186, 1843–1851 (1997).
Byrne, P., McGuirk, P., Todryk, S. & Mills, K.H. Depletion of NK cells results in disseminating lethal infection with Bordetella pertussis associated with a reduction of antigen-specific Th1 and enhancement of Th2, but not Tr1 cells. Eur. J. Immunol. 34, 2579–2588 (2004).
Mahon, B.P. & Mills, K.H. Interferon-gamma mediated immune effector mechanisms against Bordetella pertussis. Immunol. Lett. 68, 213–217 (1999).
Canthaboo, C., Xing, D., Wei, X.Q. & Corbel, M.J. Investigation of role of nitric oxide in protection from Bordetella pertussis respiratory challenge. Infect. Immun. 70, 679–684 (2002).
Gueirard, P., Druilhe, A., Pretolani, M. & Guiso, N. Role of adenylate cyclase-hemolysin in alveolar macrophage apoptosis during Bordetella pertussis infection in vivo. Infect. Immun. 66, 1718–1725 (1998).
Khelef, N. & Guiso, N. Induction of macrophage apoptosis by Bordetella pertussis adenylate cyclase-hemolysin. FEMS Microbiol. Lett. 134, 27–32 (1995).
Ruwanpura, S.M. et al. Non-essential role for TLR2 and its signaling adaptor Mal/TIRAP in preserving normal lung architecture in mice. PLoS One 8, e78095 (2013).
Guidi-Rontani, C. The alveolar macrophage: the Trojan horse of Bacillus anthracis. Trends Microbiol. 10, 405–409 (2002).
Rosendahl, A., Bergmann, S., Hammerschmidt, S., Goldmann, O. & Medina, E. Lung dendritic cells facilitate extrapulmonary bacterial dissemination during pneumococcal pneumonia. Front. Cell. Infect. Microbiol. 3, 21 (2013).
Ghoneim, H.E., Thomas, P.G. & McCullers, J.A. Depletion of alveolar macrophages during influenza infection facilitates bacterial superinfections. J. Immunol. 191, 1250–1259 (2013).
Liu, Q., Li, W., Li, D., Feng, Y. & Tao, C. TIRAP C539T polymorphism contributes to tuberculosis susceptibility: evidence from a meta-analysis. Infect. Genet. Evol. 27C, 32–39 (2014).
Dunne, A. et al. A novel TLR2 agonist from Bordetella pertussis is a potent adjuvant that promotes protective immunity with an acellular pertussis vaccine. Mucosal Immunol. advance online publication, 15 October 2014; doi: 10.1038/mi.2014.93 (e-pub ahead of print) (2014).
McGuirk, P., McCann, C. & Mills, K.H. Pathogen-specific T regulatory 1 cells induced in the respiratory tract by a bacterial molecule that stimulates interleukin 10 production by dendritic cells: a novel strategy for evasion of protective T helper type 1 responses by Bordetella pertussis. J. Exp. Med. 195, 221–231 (2002).
Acknowledgements
This work was supported by Science Foundation Ireland Principal Investigator grants to Luke O’Neill and Kingston Mills (06/IN.1/B87) and a PhD scholarship to Nicholas Bernard from the Irish Health Research Board. We thank Brian Cloak for his assistance in the preparation of the photomicrographs.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
K.H.G. Mills is a co-founder and shareholder in Opsona Therapeutics and TriMod Therapeutics, the university spin-out companies involved in the development of immunotherapeutics. L.A. O’Neill is a co-founder, shareholder, and board member in Opsona Therapeutics. The other authors declared no conflict of interest.
Rights and permissions
About this article

Cite this article
Bernard, N., Finlay, C., Tannahill, G. et al. A critical role for the TLR signaling adapter Mal in alveolar macrophage-mediated protection against Bordetella pertussis. Mucosal Immunol 8, 982–992 (2015). https://doi.org/10.1038/mi.2014.125
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/mi.2014.125
