
Abstract
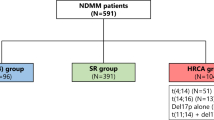
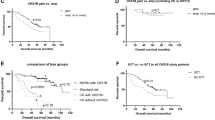
Translocation (11;14) on interphase fluorescent in situ hybridization in plasma cells is regarded as a standard risk prognostic marker in multiple myeloma based on studies conducted before introduction of current therapies. We identified 365 patients with t(11;14), and 730 matched controls:132 patients with non-(11;14) translocations and 598 patients with no chromosomal translocation. The median progression-free survival for the three groups were 23.0 (95% confidence interval (CI), 20.8–27.6), 19.0 (95% CI, 15.8–22.7) and 28.3 (95% CI, 25.7–30.6) months, respectively (P<0.01). The median overall survival (OS) for t(11;14), non-(11;14) translocation and no-translocation groups were 74.4 (95% CI, 64.8–89.3), 49.8 (95% CI, 40.0–60.6) and 103.6 (95% CI, 85.2–112.3) months, respectively (P<0.01). Excluding those with 17p abnormality, the median OS in the three groups were 81.7 (95% CI, 67.0–90.7), 58.2 (95% CI, 47.0–76.4) and 108.3 (95% CI, 92.4–140.1) months, respectively (P<0.01). The above relationship held true in patients with age <65 years, international staging system (ISS) I/II stage or those who received novel agent-based induction. Advanced age (hazard ratio (HR): 1.98), 17p abnormality (HR: 2.2) and ISS III stage (HR: 1.59) at diagnosis predicted reduced OS in patients with t(11;14). These results suggest that outcomes of t(11;14) MM are inferior to other standard risk patients.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Rajkumar SV . Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management. Am J Hematol 2016; 91: 719–734.
Avet-Loiseau H, Facon T, Grosbois B, Magrangeas F, Rapp M-J, Harousseau J-L et al. Oncogenesis of multiple myeloma: 14q32 and 13q chromosomal abnormalities are not randomly distributed, but correlate with natural history, immunological features, and clinical presentation. Blood 2002; 99: 2185–2191.
Fonseca R, Blood EA, Oken MM, Kyle RA, Dewald GW, Bailey RJ et al. Myeloma and the t(11;14)(q13;q32); evidence for a biologically defined unique subset of patients. Blood 2002; 99: 3735–3741.
Segges P, Braggio E, Minnicelli C, Hassan R, Zalcberg IR, Maiolino A . Genetic aberrations in multiple myeloma characterized by cIg-FISH: a Brazilian context. Braz J Med Biol Res 2016; 49: e5034.
Avet-Loiseau H, Attal M, Moreau P, Charbonnel C, Garban F, Hulin C et al. Genetic abnormalities and survival in multiple myeloma: the experience of the Intergroupe Francophone du Myelome. Blood 2007; 109: 3489–3495.
An G, Xu Y, Shi L, Zou D, Deng S, Sui W et al. t(11;14) multiple myeloma: a subtype associated with distinct immunological features, immunophenotypic characteristics but divergent outcome. Leuk Res 2013; 37: 1251–1257.
Avet-Loiseau H, Garand R, Lode L, Harousseau JL, Bataille R . Translocation t(11;14)(q13;q32) is the hallmark of IgM, IgE, and nonsecretory multiple myeloma variants. Blood 2003; 101: 1570–1571.
Moreau P, Facon T, Leleu X, Morineau N, Huyghe P, Harousseau JL et al. Recurrent 14q32 translocations determine the prognosis of multiple myeloma, especially in patients receiving intensive chemotherapy. Blood 2002; 100: 1579–1583.
Garand R, Avet-Loiseau H, Accard F, Moreau P, Harousseau JL, Bataille R . t(11;14) and t(4;14) translocations correlated with mature lymphoplasmacytoid and immature morphology, respectively, in multiple myeloma. Leukemia 2003; 17: 2032–2035.
Robillard N, Avet-Loiseau H, Garand R, Moreau P, Pineau D, Rapp MJ et al. CD20 is associated with a small mature plasma cell morphology and t(11;14) in multiple myeloma. Blood 2003; 102: 1070–1071.
Kumar SK, Rajkumar SV, Dispenzieri A, Lacy MQ, Hayman SR, Buadi FK et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood 2008; 111: 2516–2520.
Kumar SK, Dispenzieri A, Lacy MQ, Gertz MA, Buadi FK, Pandey S et al. Continued improvement in survival in multiple myeloma: changes in early mortality and outcomes in older patients. Leukemia 2014; 28: 1122–1128.
Sasaki K, Lu G, Saliba RM, Bashir Q, Hosing C, Popat U et al. Impact of t(11;14)(q13;q32) on the outcome of autologous hematopoietic cell transplantation in multiple myeloma. Biol Blood Marrow Transplant 2013; 19: 1227–1232.
Shin HJ, Kim K, Lee JJ, Song MK, Lee EY, Park SH et al. The t(11;14)(q13;q32) translocation as a poor prognostic parameter for autologous stem cell transplantation in myeloma patients with extramedullary plasmacytoma. Clin Lymphoma Myeloma Leuk 2015; 15: 227–235.
Kaufman GP, Gertz MA, Dispenzieri A, Lacy MQ, Buadi FK, Dingli D et al. Impact of cytogenetic classification on outcomes following early high-dose therapy in multiple myeloma. Leukemia 2016; 30: 633–639.
International Myeloma Working Group. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Bri J Haematol 2003; 121: 749–757.
Durie BG, Harousseau JL, Miguel JS, Blade J, Barlogie B, Anderson K et al. International uniform response criteria for multiple myeloma. Leukemia 2006; 20: 1467–1473.
Kyle RA, Rajkumar SV . Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia 2009; 23: 3–9.
Rajkumar SV, Harousseau JL, Durie B, Anderson KC, Dimopoulos M, Kyle R et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood 2011; 117: 4691–4695.
Rajkumar SV, Richardson P, San Miguel JF . Guidelines for determination of the number of prior lines of therapy in multiple myeloma. Blood 2015; 126: 921–922.
Fonseca R, Blood E, Rue M, Harrington D, Oken MM, Kyle RA et al. Clinical and biologic implications of recurrent genomic aberrations in myeloma. Blood 2003; 101: 4569–4575.
Chesi M, Bergsagel PL, Brents LA, Smith CM, Gerhard DS, Kuehl WM . Dysregulation of cyclin D1 by translocation into an IgH gamma switch region in two multiple myeloma cell lines. Blood 1996; 88: 674–681.
Gabrea A, Bergsagel PL, Chesi M, Shou Y, Kuehl WM . Insertion of excised IgH switch sequences causes overexpression of cyclin D1 in a myeloma tumor cell. Mol Cell 1999; 3: 119–123.
Specht K, Haralambieva E, Bink K, Kremer M, Mandl-Weber S, Koch I et al. Different mechanisms of cyclin D1 overexpression in multiple myeloma revealed by fluorescence in situ hybridization and quantitative analysis of mRNA levels. Blood 2004; 104: 1120–1126.
Bergsagel PL, Chesi M, Nardini E, Brents LA, Kirby SL, Kuehl WM . Promiscuous translocations into immunoglobulin heavy chain switch regions in multiple myeloma. Proc Natl Acad Sci USA 1996; 93: 13931–13936.
Chesi M, Bergsagel P, Brents L, Smith C, Gerhard D, Kuehl W . Dysregulation of cyclin D1 by translocation into an IgH gamma switch region in two multiple myeloma cell lines [see comments]. Blood 1996; 88: 674–681.
Fonseca R, Witzig TE, Gertz MA, Kyle RA, Hoyer JD, Jalal SM et al. Multiple myeloma and the translocation t(11;14)(q13;q32): a report on 13 cases. Br J Haematol 1998; 101: 296–301.
Fonseca R, Hoyer JD, Aguayo P, Jalal SM, Ahmann GJ, Rajkumar SV et al. Clinical Significance of the Translocation (11;14)(q13;q32) in Multiple Myeloma. Leuk Lymphoma 1999; 35: 599–605.
Leiba M, Duek A, Amariglio N, Avigdor A, Benyamini N, Hardan I et al. Translocation t(11;14) in newly diagnosed patients with multiple myeloma: Is it always favorable? Genes Chromosomes Cancer 2016; 55: 710–718.
Kumar S, Fonseca R, Ketterling RP, Dispenzieri A, Lacy MQ, Gertz MA et al. Trisomies in multiple myeloma: impact on survival in patients with high-risk cytogenetics. Blood 2012; 119: 2100–2105.
Kumar S, Vij R, Kaufman JL, Mikhael J, Facon T, Pegourie B et al. Venetoclax Monotherapy for Relapsed/Refractory Multiple Myeloma: Safety and Efficacy Results from a Phase I Study. Am Soc Hematology 2016. Annual meeting of American Society of Hematology, San Diego, CA, December 4, 2016.
Acknowledgements
Author contributions
AL and MAM collected and analyzed the data, wrote the first draft and approved the final version of the manuscript; SVR, AD, MAG, FKB, MQL, DD, ALF, SRH, MAH, WIG, YLH, PK, NL, RSG, YL, TVK, JAL, SJR and SRZ performed patient management, revised the manuscript critically and approved the final version of the manuscript; RAK performed patients’ follow-up, revised the manuscript critically, and participated in final data analysis and approval of the final version of the manuscript; and SKK designed the study, analyzed the data, wrote the first draft, approved the final version of the manuscript and performed patient management.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
AD received research funding from Celgene, Millennium, Pfizer and Janssen and travel grant from Pfizer. MAG received consulting fees from Millenium and honoraria from Celgene, Millenium, Onyx, Novartis, Smith Kline, Prothena, Ionis and Amgen. MQL received research funding from Celgene. PK received research funding from Takeda, Celgene and Amgen. SKK received consulting fees from Celgene, Millennium, Onyx, Janssen and BMS and research funding from Celgene, Millennium, Novartis, Onyx AbbVie, Janssen and BMS. The remaining authors declare no competing financial interest.
Additional information
Presented as oral presentation at the 16th International Myeloma Workshop, New Delhi, India, 3 March 2017 and as poster at the annual meeting of American Society of Clinical Oncology, Chicago, IL, USA, 5 June 2017.
Supplementary Information accompanies this paper on the Leukemia website
Supplementary information
Rights and permissions
About this article

Cite this article
Lakshman, A., Alhaj Moustafa, M., Rajkumar, S. et al. Natural history of t(11;14) multiple myeloma. Leukemia 32, 131–138 (2018). https://doi.org/10.1038/leu.2017.204
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/leu.2017.204
This article is cited by
-
Multiple myeloma with t(11;14): impact of novel agents on outcome
Blood Cancer Journal (2023)
-
Combination venetoclax and selinexor effective in relapsed refractory multiple myeloma with translocation t(11;14)
npj Precision Oncology (2022)
-
High-risk disease in newly diagnosed multiple myeloma: beyond the R-ISS and IMWG definitions
Blood Cancer Journal (2022)
-
Treatment patterns and outcomes according to cytogenetic risk stratification in patients with multiple myeloma: a real-world analysis
Blood Cancer Journal (2022)
-
Venetoclax in combination with carfilzomib and dexamethasone in relapsed/refractory multiple myeloma harboring t(11,14)(q13;q32): two case reports and a review of the literature
Journal of Medical Case Reports (2020)
