
Abstract
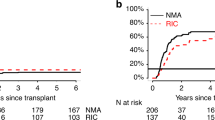
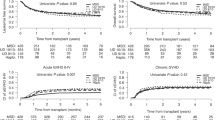
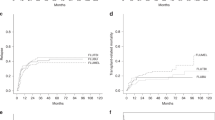
Allogeneic stem cell transplantation (SCT) provides the best mechanism of preventing relapse in acute myeloid leukaemia (AML). However non-relapse mortality (NRM) negates this benefit in older patients. Reduced intensity conditioning (RIC) permits SCT with reduced NRM, but its contribution to cure is uncertain. In the MRC AML15 Trial, patients in remission without favourable risk disease could receive SCT from a matched sibling or unrelated donor (MUD). If aged >45 years, a RIC was recommended and in patients aged 35–44 years, either RIC or myeloablative conditioning was permitted. The aim was to determine which approach improved survival and within which prespecified cytogenetic groups. RIC transplants significantly reduced relapse (adjusted hazard ratio (HR) 0.66 (0.50–0.85), P=0.002) compared to chemotherapy The 5-year overall survival from a sibling RIC (61%) was superior to a MUD RIC (37%; adjusted HR 1.50 (1.01–2.21), P=0.04) due to lower NRM (34 vs 14%, P=0.002) In adjusted analyses, there was a survival benefit for sibling RIC over chemotherapy (59 vs 49%, HR 0.75 (0.57–0.97), P=0.03), with consistent results in intermediate and adverse-risk patients. In patients aged 35–44 years, best outcomes were seen with a sibling RIC transplant, although a comparison with chemotherapy and myeloablative transplant was not significant in adjusted analyses (P=0.3).
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others
References
Burnett AK, Hills RK, Milligan D, Kjeldsen L, Kell J, Russell NH et al. Identification of patients with acute myeloblastic leukemia who benefit from the addition of gemtuzumab ozogamicin: results of the MRC AML15 trial. J Clin Oncol 2011; 29: 369–377.
Castaigne S, Pautas C, Terre C, Raffoux E, Bordessoule D, Bastie JN et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet 2012; 379: 1508–1516.
Burnett AK, Russell NH, Hills RK, Kell J, Freeman S, Kjeldsen L . Addition of gemtuzumab ozogamicin to induction chemotherapy improves survival in older patients with acute myeloid leukemia. J Clin Oncol 2012; 30: 3924–3931.
Cornelissen J, van Putten WLJ, Verdonck LF, Theobald M, Jacky E, Daenen SM et al. Results of a HOVON/SAKK donor versus no-donor analysis of myeloablative HLA-identical sibling stem cell transplantation in first remission acute myeloid leukemia in young and middle-aged adults: benefits for whom? Blood 2007; 109: 3658–3666.
Koreth J, Schlenk R, Kopecky KJ, Honda S, Sierra J, Djulbegovic BJ et al. Allogeneic stem cell transplantation for acute myeloid leukemia in first complete remission: systematic review and meta-analysis of prospective clinical trials. JAMA 2009; 301: 2349–2361.
Walter RB, Pagel JM, Gooley TA, Petersdorf EW, Sorror ML, Woolfrey AE et al. Comparison of matched unrelated and matched related donor myeloablative hematopoietic cell transplantation for adults with acute myeloid leukemia in first remission. Leukemia 2010; 24: 1276–1282.
Burnett AK, Hills RK, Milligan DW, Goldstone AH, Prentice AG, McMullin MF et al. Attempts to optimize induction and consolidation treatment in acute myeloid leukemia: results of the MRC AML12 trial. J Clin Oncol 2010; 28: 586–595.
Schlenk RF, Dohner K, Mack S., Stoppel M, Király F, Götze K et al. Prospective evaluation of allogeneic hematopoietic stem-cell transplantation from matched related and matched unrelated donors in younger adults with high-risk acute myeloid leukemia: German-Austrian Trial AMLHD98A. J Clin Oncol 2010; 28: 4642–4648.
Mohty M, Bay JO, Faucher C, Choufi B, Bilger K, Tournilhac O et al. Graft-versus host disease following allogeneic transplantation from HLA-identical siblings with antithymocyte globulin-based reducedintensity preparative regimen. Blood 2003; 102: 470–476.
Hegenbart U, Niederwieser D, Sandmaier BM, Maris MB, Shizuru JA, Greinix H et al. Treatment for acute myelogenous leukemia by lowdose, total-body irradiation-based conditioning and hematopoietic cell transplantation from related and unrelated donors. J Clin Oncol 2006; 24: 444–453.
Mohty M, de Lavallade H, El-Cheikh J, Ladaique P, Faucher C, Fürst S et al. Reduced intensity conditioning allogeneic stem cell transplantation for patients with acute myeloid leukemia: long term results of a “donor” versus “no donor” comparison. Leukemia 2009; 23: 194–196.
Burnett AK, Russell NH, Hills RK, Hunter AE, Kjeldsen L, Yin J et al. Optimization of chemotherapy for younger patients with acute myeloid leukemia: results of the medical research council AML15 trial. J Clin Oncol 2013; 31: 3360–3368.
Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML: 10 Trial. Blood 1998; 92: 2322–2333.
Cheson BD, Bennett JM, Kopecky KJ, Büchner T, Willman CL, Estey EH et al. Revised recommendations of the international Working Group for diagnosis, standardization of response criteria treatment outcomes, and reporting standards for therapeutic trials in acute myeloid leukemia. J Clin Oncol 2003; 21: 4642–4649.
Mantel N, Byar DP . Evaluation of response-time data involving transient states: An illustration using heart-transplant data. J Am Stat Assoc 1974; 69: 81–86.
McClune BL, Weisdorf DJ, Pedersen TL, Tunes da Silva G, Tallman MS, Sierra J et al. Effect of age on outcome of reduced-intensity hematopoietic cell transplantation for older patients with acute myeloid leukemia in first complete remission or with myelodysplastic syndrome. J Clin Oncol 2010; 28: 1878–1887.
Sorror ML, Maris MB, Storer B, Sandmaier BM, Diaconescu R, Flowers C et al. Comparing morbidity and mortality of HLA-matched unrelated donor hematopoietic cell transplantation after nonmyeloablative and myeloablative conditioning: influence of pretransplantation comorbidities. Blood 2004; 104: 961.
Acknowledgements
The research costs of the AML15 trial were supported by the UK Medical Research Council. Research Funding for this trial was provided by the Medical Research Council of Great Britain.
Author Contributions
AKB, NHR and RKH were responsible for the conception and design of the study. AKB, NHR, LK, AP, CC, REC and JAY provided the study materials or patients. AKB, NHR, RKH, LK, AP, CC, REC and JAY were responsible for the collection and assembly of the data. AKB, NHR, RKH, AH were responsible for data analysis and interpretation. All the authors contributed to the writing and final approval of the manuscript.
UK NCRI Adult AML Working Party
The following centres performed transplants analysed in this study: Aberdeen Royal Infirmary; Addenbrooke's Hospital; Auckland City Hospital; Beatson West of Scotland Cancer Centre; Belfast City Hospital; Birmingham Heartlands Hospital; Bristol BMT Unit; Christchurch Hospital; Christie Hospital; Derriford Hospital; Glasgow Royal Infirmary; Guy's Hospital; Hammersmith Hospital; John Radcliffe Hospital; King's College Hospital; Leeds General Infirmary; Leicester Royal Infirmary; Manchester Royal Infirmary; Nottingham City Hospital; Queen Elizabeth Hospital Birmingham; Rigshospitalet; Royal Free Hospital; Royal Hallamshire Hospital Sheffield; Royal Liverpool University Hospital; Royal Marsden Hospital; Royal Victoria Infirmary; Southampton General Hospital; St Bartholomew's Hospital; St George's Hospital; St James University Hospital; University College Hospital; University Hospital of Wales; Wellington Hospital; Western General Hospital.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on the Leukemia website
Supplementary information
Rights and permissions
About this article

Cite this article
Russell, N., Kjeldsen, L., Craddock, C. et al. A comparative assessment of the curative potential of reduced intensity allografts in acute myeloid leukaemia. Leukemia 29, 1478–1484 (2015). https://doi.org/10.1038/leu.2014.319
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/leu.2014.319
This article is cited by
-
Age and allogeneic hematopoietic cell transplantation outcomes in acute myeloid leukemia
International Journal of Hematology (2023)
-
Poor prognostic implications of myelodysplasia-related mutations in both older and younger patients with de novo AML
Blood Cancer Journal (2023)
-
Predicting non-relapse mortality following allogeneic hematopoietic cell transplantation during first remission of acute myeloid leukemia
Bone Marrow Transplantation (2021)
-
Long-term results of reduced-intensity conditioning allogeneic hematopoietic cell transplantation for older patients with acute myeloid leukemia: a retrospective analysis of 10-year follow-up data
Bone Marrow Transplantation (2020)
-
Allogeneic Hematopoietic Stem Cell Transplantation for Older Patients With Acute Myeloid Leukemia
Current Treatment Options in Oncology (2018)
