
Abstract
Objective:
Our objective was to evaluate the impact of a dedicated resuscitation and stabilization (RAS) room and process changes on infant stabilization time.
Study Design:
A prospective quality improvement study was conducted on preterm infants in a tertiary care center. A dedicated RAS room, preresuscitation huddle, infant–isolette–ventilator pairing and improved documentation were implemented. The primary outcome was median time to stabilization and secondary outcomes were illness severity on day 1 and morbidity at discharge.
Results:
A sustained reduction in median time to stabilization from 90 min in the preimplementation phase to 72 min in the sustainability phase was observed. All planned and iterative process changes were integrated into the RAS team’s daily routine. Time to completion of procedures decreased, illness severity and morbidity remained unchanged.
Conclusion:
A dedicated RAS room adjacent to the delivery suite in conjunction with process changes improves efficiency of care.
Similar content being viewed by others


Introduction
Almost every preterm infant <33 weeks gestational age needs some form of resuscitation at birth. Preterm infants often require life-saving interventions for cardiorespiratory stability, and they are invariably transferred to the neonatal intensive care unit (NICU) for subsequent management.1, 2 Management during the ‘golden hour’ involves multiple procedures and investigations, extensive handling, invasive and non-invasive monitoring and titrating treatment according to response. This period has been described as intense, chaotic and prone to error and miscommunication and requires a seamless coordination of multiple health-care providers.3
The resuscitation and stabilization (RAS) environment and organized care during this period are crucial in optimizing outcomes and enhancing patient safety. Technical procedures, vigilant monitoring, teamwork and avoidance of errors are best accomplished in an environment conducive for critical care.4, 5 Moreover, preterm infants are at greater thermal risk and often require additional personnel, equipment and time to optimize RAS.6 Seventeen percent of neonatal programs in the United States7 and 43% of neonatologists in Canada8 reported resuscitating newborns in an area adjacent to the delivery room. The benefits of a dedicated infant RAS room have not been reported.8
Problem description
In 2010, resuscitation in our center was performed in several delivery rooms and infants were quickly transferred to the NICU for stabilization. An internal audit identified the following missed opportunities for improvement: (i) unfavorable environment during resuscitation, including limited space, variation in type and arrangement of equipment in every delivery room, low ambient room temperature and overcrowding, (ii) major handling and exposure to three ventilators and three infant beds in the first 4 days of life, (iii) multiple handovers between interprofessional team members as admission and stabilization teams were different, (iv) inadequate documentation of interventions employed and response to treatment, and (v) disruption of care, chaos, excessive traffic and noise in the NICU during the process.
We hypothesized that commissioning a dedicated RAS room in the labor and delivery vicinity and streamlining care processes would improve efficient delivery of care resulting in reduction in time to stabilization. We believed that RAS conducted in a non-stressful, familiar environment with better monitoring equipment would improve vigilance, timely decision-making and efficiency of care. Our primary quality improvement (QI) objective was to reduce median time to stabilization by 25% in preterm inborn infants within 12 months of commissioning a dedicated RAS room. Secondary objectives were to improve care processes associated with RAS.
Methods
This was a prospective QI study.
Study population and setting
The institutional Research Ethics Board with a waiver of consent approved the study. The hospital has a 47-bed level-3 NICU. The labor and delivery facility is located adjacent to the NICU and comprises 10 delivery rooms and 2 dedicated operating rooms. Annually about 3000 deliveries occur in our center, and approximately 200 inborn infants <33 weeks’ gestation are resuscitated, stabilized and admitted to the NICU. A neonatal fellow, nurse practitioner, trained resuscitation nurse and a respiratory therapist attend all deliveries. A neonatologist is in attendance for infants born at <26 weeks’ gestation.
In 2010, a large QI project aimed at improving practices during resuscitation, stabilization and the initial hours of life in preterm infants was introduced. The commission of a dedicated RAS room was an initiative nested within the larger QI project. A subgroup involving a nurse practitioner, registered nurse and physicians (project lead and medical director) was formed to plan the transition and successful implementation of the RAS room. In order to ensure progress and momentum, the team met once every 2 weeks till the RAS room was authorized for service.
The commissioning of the RAS room and evaluation of its impact was performed in four phases to track changes over time: preimplementation (Phase 1, February 2011–January 2012), implementation (Phase 2, February–July 2012), postimplementation (Phase 3, August 2012–July 2013), and sustainability (Phase 4, August 2013–June 2014). At the beginning of the preimplementation phase, the subteam’s goal was to describe the project charter, including aims, measures and projected changes, and develop a key driver diagram and necessary Plan, Do, Study, Act cycle. During the first two months, the QI subteam assembled the floor plan, designed the RAS room layout and created a list of equipment and fixtures that would be necessary to optimize functionality of the RAS room. They also reviewed the existing workflow sequence starting from receiving a call and attendance at delivery until the infant was admitted and stabilized in the NICU. Similarly, specific team preparation, performance, documentation and handovers related to the resuscitation and NICU teams were reviewed. At the outset, the QI subteam identified RAS related process changes that needed improvement and not specific to the place of stabilization. This included infant-specific team preparation, definition of the RAS period and transporting infants from the delivery room to the RAS room and subsequently to the NICU. The subteam recognized that redesigning processes would include avoidance of excessive infant handling and use of several devices, planning efficient handover and reviewing caregiver workload and workflow integration. Three interventions were tested a priori before commissioning the RAS room: preresuscitation team (August–October 2011), infant–isolette–ventilator pairing (March–May 2011), and improve documentation of care (March–June 2011). Using simulated scenarios, the new environment of care in the RAS room was tested by performing six mock drills (November–December 2011). Based on evaluation of above interventions for team satisfaction, feasibility and desire to integrate into RAS team routine, 16 new pairing devices were ordered and a request was sent to information technology services to incorporate ‘delivery room summary of care’ fields in electronic patient charts. The QI team recognized the importance of contextual and explanatory factors related to the implementation process in order to facilitate ongoing evaluation and implementation of sequential changes.9
Interventions
The following interventions were implemented sequentially every 4 weeks in that order.
-
1
Relocate stabilization of infants from NICU to the RAS room. It was believed that there would be a conceivable improvement in environment that would result in seamless coordination of multiple caregivers, room climate and design, equipment availability and fewer distractions.
-
2
Preresuscitation huddle: A daily, 15-min, mandatory preresuscitation team huddle on planned high-risk deliveries were scheduled. For unplanned high-risk deliveries, an ad hoc huddle was encouraged. The aim of the huddle was to clarify member roles, achieve team situational awareness and ensure team preparation for the anticipated risks. The huddles were led by a neonatal fellow and supervised by the neonatal attending in charge of RAS. When significant problems were anticipated, the resuscitation team developed a plan to prevent or mitigate the risk. This process provided a standardized opportunity for a more experienced clinician to watch those less experienced in both infant management and communication escalation techniques.
-
3
Infant–isolette–ventilator pairing: Historically, infants were resuscitated in delivery rooms, transferred to the NICU using a transport incubator and ventilator and subsequently stabilized in the NICU on another ‘resuscitaire’ and ventilator. Over the next 4 days, ventilators were changed to provide different modalities of ventilation, not offered by a single device. This process interrupted care and resulted in unnecessary infant handling and diverse equipment exposure. Based on our pilot work, we implemented the ‘one baby, one bed and one ventilator for the first 96 h’ intervention as a standard of care by using an equipment coupling device (mac-link).
-
4
Improve documentation of delivery room summary of care: The principal aim was to rapidly identify process flaws and direct this information to the QI subteam and unit managers. In order to achieve this objective, ‘delivery room summary of care’ data fields were created in electronic health records; nursing staff, respiratory therapists and physicians were educated on completing the birth record, procedure notes and medication record; and process data was included in the monthly newsletter and distributed to all caregivers. Lessons learnt and suggestions for improvement were shared among the QI subteam, medical director and unit-level managers.
-
5
Others: Processes were developed, manuals were created and the RAS team members were educated on obstetric and neonatal team member roles, distinguish RAS periods, identify infants appropriate for stabilization in the RAS room and optimize modes of transfer between the delivery, operating rooms and the RAS room and subsequently from the RAS room to the NICU. Resuscitation team members, including the attending in charge of RAS for the day, were identified and posted and the obstetric and NICU services were notified. Resuscitation team members were encouraged to plan RAS as a continuum and focus on better vigilance, decision-making and procedural performance by appropriately skilled personnel, titration of treatment and timely completion of tasks. The QI subteam and unit-level managers coached resuscitation team members to dissolve the prevalent mindset of quick resuscitation and quick hand over to the NICU team, without due consideration of the stabilization process. Lessons learnt and suggestions for ongoing improvement were shared among the QI subteam, medical director and unit-level managers (Supplementary Table S1). Other guidelines and procedures related to RAS did not change during the entire study period.1, 10, 11 amd 12
Study of the intervention
Two investigators (SS and LB) reviewed 30 consecutive records at the beginning of the preimplementation phase to identify measures that could accurately reflect the effectiveness and efficiency of care during RAS. Given the number of processes involved during RAS, stabilization time was selected as the primary outcome measure, as it was easy to measure, understand and track over time. Moreover, efficiency of care is one of the domains for evaluating the quality of care. Stabilization time was defined as the time interval between birth and initiation of developmentally supportive care positioning. It encompassed episodes of handling, transport to RAS room, collection of blood samples, portable radiograph, administration of vitamin K and erythromycin eye ointment, procedure of initiation of intravenous therapy, reviewing and adjusting vascular lines and tubes and admission to NICU. Developmentally supportive care positioning was defined as ‘infant positioned supine, side lying or prone but maintained in flexed position using one or more methods, including swaddling, nesting, cloth boundaries or commercially available devices.13 We chose initiation of developmentally supportive care positioning as the end point of stabilization, as it was an easily identifiable event, performed on all infants and was usually established when the infant was stable. Though stabilization time has not been correlated with other established proximal measures of neonatal outcome, such as Score for Neonatal Acute Physiology-Perinatal Extension-II (SNAPPE-II) or morbidity, we choose to use it as a process measure and a surrogate measure of quality. Finally, it was also easy to advertise a goal of completing stabilization within 60 min. We believed that such an emphasis would encourage team members’ to focus on tasks aimed at periodic infant assessment, decision-making and appropriate actions in the first 60 min, as opposed to multiple handoffs, waiting for equipment/personnel/radiograph and documentation.
The implementation strategy14 included creating awareness, improving access to project documents, monitoring compliance and reinforcing the use of all interventions consistently and acknowledging and addressing caregivers’ concerns about the interventions.
Chart reviews by the project coordinator captured process data within 24 h of birth. Outcome data were collected using hospital patient records, housed in the Canadian Neonatal Network database.15 The QI subteam members assembled data during the testing and piloting phases of the project. Data were collected on process measures: proportion of infants stabilized in the RAS room, use of the mac-link pairing device (Hamilton Health Sciences, Biomedical Technology, Hamilton, Ontario, Canada), time to NICU arrival, and documentation of care during the RAS period.
Outcomes
The primary outcome measure was stabilization time. The secondary outcome measures were the time to completion of procedures, SNAPPE-II16 and morbidity at discharge. Disruption of care during transition from resuscitation to stabilization and workflow, major handling episodes, exposure to multiple devices, chaos, perceived traffic and noise levels in the NICU at admission were audited on 30 admissions by QI subteam members during the postimplementation phase. However, components of teamwork: preparation, consistency of care, decision-making, vigilance, individualized care planning, and treatment changes, could not be measured. Any procedure (umbilical or peripheral venous catheterization, surfactant administration or intubation) performed after 3 h of life was regarded as ‘late’ and was excluded in determining the infant stabilization time. The ongoing assessment of contextual elements that contributed to the success, failure and efficiency were documented through field notes during multiple participant observations and monthly QI subteam meetings.
Analysis
The process outcome measures were analyzed by using statistical process control charts (QI Macros for excel 2015, KnowWare International, Inc., Denver, CO, USA). The results were tracked by using X median R charts. Established rules for identifying special cause were employed.17, 18 and 19 Comparison of patient demography, proportion of infants receiving various interventions during stabilization and outcomes at discharge across the study phases were performed using chi-square test for categorical variables and Kruskal–Wallis test for continuous variables (SPSS Statistics for Windows, Version 22.0, IBM, IBM Corp., Armonk, NY, USA).
Results
The study flow diagram with eligible infants in various study phases is provided in Figure 1. There were 229, 97, 229 and 176 infants in the preimplementation, implementation, postimplementation and sustainability phases, respectively. Patient demographic characteristics were similar (Table 1). The proportion of infants receiving interventions during RAS was similar during the four phases (Table 2).

Study flow diagram showing pathways for resuscitation and stabilization (RAS). Number of infants (%) in the various phases are shown at the bottom. Pathways: A=Resuscitation in the delivery room (DR)/operating room (OR) and stabilization in neonatal intensive care unit (NICU), B=RAS in the RAS room, C=Resuscitation in DR/OR and stabilization in RAS room.
One hundred and eighty NICU interprofessional care providers received orientation to the location, layout and access to the RAS room. Eighty-two (~80%) of resuscitation team members attended the didactic sessions, open forums and participated in the ‘seek and find’ self-directed orientation events. The QI subteam provided didactic sessions and covered topics pertaining to the RAS room during day and night shifts. All 36 respiratory therapists received training in the mac-link coupling device.
The median time to stabilization decreased from 90 min in preimplementation Phase 1 to 72 min in Phase 4 (Figure 2). Control chart analysis showed an initial decline in stabilization time in Phase 2 and early Phase 3, meeting the criteria for a special cause variation (2 out of 3 points below 2 sigma and 4 out of 5 points below 1 sigma). However, the stabilization time increased in the latter part of Phase 3. Following an awareness campaign and strengthening the orientation process for all learners and new staff, the median stabilization further declined to 72 min in Phase 4.

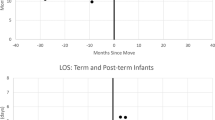
Control chart showing median time to stabilization over different phases of the program. Footnote: CL, central line; red dotted lines upper (UCL) and lower (LCL) control limits; Red solid line—undesirable special causes variation; green solid line—desirable special cause variation. A color version of this figure is available online.
The proportion of infants stabilized in the RAS room increased over the study period from 54% in Phase 2 to 92% in Phase 4 (Figure 1). During the first 3 months of implementation, the mac-link device use, preresuscitation huddle days, documentation of delivery room summary of care increased from 0% to 60%, from 20% to 80% and from 0% to 80%, respectively. Time to arrival in the NICU increased from a median of 19 min in Phase 1 to 69 min in Phase 4 (Figure 3).

Time to completion of various stabilization events. x Axis: year and month; y axis: median time to neonatal intensive care unit (NICU) arrival and completion of procedures in minutes. PIV; peripheral intravenous catheter; UAC, umbilical arterial catheter; UVC, umbilical venous catheter.
The secondary outcome measures: times to first successful intubation, umbilical arterial and venous catheter and peripheral intravenous insertion and radiography declined over time, and met the criteria for special cause variation. However, there was no sustained change in the time to surfactant administration (Figure 3). The median SNAPPE-II scores remain unchanged. There was no difference in the proportion of infants with mortality, sepsis and bronchopulmonary dysplasia at 36 weeks postmenstrual age, postnatal steroid use, patent ductus arteriosus treated medically or surgically, pneumothorax and intracranial lesions on ultrasonography (Table 3). Concomitantly, a significant increase was noted in necrotizing enterocolitis during the implementation phase. The ongoing assessment of contextual elements that contributed to the success, failure and efficiency of the project are provided in Supplementary Table S2.
Discussion
We have demonstrated a sustained 20% reduction in time to stabilization and time to complete interventions during RAS after implementing a dedicated RAS room and changes in care processes.
Several other features were also noted during the project. First, infant stabilization time was chosen to assess efficiency and effective teamwork during RAS. One of the concerns expressed was that resuscitation team members were forced into rapid decision-making in order to complete the stabilization within 60 min thereby erring on performing more interventions than necessary, for example, intubation. Similarly, a reduction in interventions during the stabilization period may falsely reduce the stabilization time. However, the results indicate a significant reduction in stabilization time without a reduction in frequency of interventions. We believe that effective and efficient care delivery in a structured familiar environment may have contributed to above observation. Second, a decline in performance and an increase in time to stabilization and completion of interventions were noted in the latter part of Phase 3. Staff complacency, a brief decline in the QI subteam’s support and a lack of orientation for learners and new staff or inability to cope up with changes in functional routines could have contributed to the undesirable outcome. Resolution was achieved through reinforcement of education and consistent performance monitoring. Third, the time to surfactant administration remained unchanged, but this is unlikely to be altered by a new RAS room with preexisting standardized intervention and treatment policies. Fourth, there was a corresponding reduction in chaos, traffic, noise and disruption of the normal NICU routine and caregivers’ workflow owing to a seamless, transition of admissions to the NICU. Fifth, infants born in the operating room were directly transferred to the RAS room for RAS. This meant parents and obstetric team members could no longer visualize an infant’s progress following delivery. Inviting parent participation in the RAS room and introducing mandatory mother–infant–caregiver contact after stabilization mitigated the concern. Finally, no data exist on the definition for RAS time during intrahospital delivery and transfer. Stabilization times can serve as a benchmark and can be used for quality assurance purposes and to plan staffing requirements.20 Similarly, the criteria for optimal stabilization and readiness for transfer out of the RAS room has not been previously defined. The QI subteam developed pragmatic definitions to measure stabilization time, which were sensible, feasible to adopt, easy to use and were responsive to process changes made during RAS.
The QI subteam members observed and reported other benefits arising out of this project during team meetings. Disruption of care in infants receiving stabilization as well as other infants receiving care in NICU were reported to be lower. Similarly, chaos, traffic and noise during admission of an infant to the NICU were perceived to be lower. Parents’ request for observing resuscitation and/or stabilization was accommodated and ‘mother–infant–caregiver contact’ following stabilization and enroute to the NICU was integrated into the transfer process. Necessary changes in admission processes and maintenance of the RAS room were made to optimize workflow.
Overall, there was little impact on mortality and morbidity at hospital discharge. The transient increase in the incidence of necrotizing enterocolitis observed during Phase 1 was probably unrelated to our interventions, as there was no ongoing trend during the later phases. Although the RAS room with other process changes led to improved efficiency of care, it did not impact severity of illness score in first 12 h of admission to NICU or patient outcomes, which may only be affected by a broader multifaceted set of interventions. This is the first study to demonstrate the impact of a dedicated RAS room for preterm infants adjacent to the labor and delivery suite. Our QI study adds value to health care by improving quality without adverse consequences. Assessing efficiency of care during RAS by identifying an acceptable process measure is an additional strength of this study. Other tertiary perinatal centers could easily adopt the process interventions and implementation strategy. The following factors had a significant role in achieving a sustained reduction in stabilization time: identifying and testing interventions prior to commissioning of the RAS room, empowering frontline staff to identify and mitigate challenges at the out start, adequate support from administrators including funding to build the mac-link device, and articulating and supporting caregivers’ efforts to complete stabilization within 60 min. Moreover, clarifying member roles and expectations within all professional groups, teaching the implementation process and presenting the impact to all caregivers at regular intervals, using multiple education strategies while moving to the new RAS room, and empowering caregivers’ to assume ownership on implementing, modifying and addressing challenges all contributed to a positive outcome.
Our study has several limitations. During the study period, undetected changes that affected our measured results could have occurred secondary to variation in leadership and procedural skills of resuscitation team members. Some of the findings could also be attributed to differences in patient variables in the various phases or differences that were not apparent on comparison of basic demographic factors. The definition of stabilization time was developed by the QI subteam. However, a data-intensive evaluation on construct validity, inter-rater and intra-rater reliability and responsiveness could not be performed in view of the pragmatic nature of the study. Finally, a cost effectiveness analysis, adaptability of the guidelines to a different population or a different unit and a survey to elicit the acceptability of the RAS room by caregivers and parents was not performed.
Conclusions
Commissioning a dedicated RAS room adjacent to the delivery rooms when combined with interventions to facilitate team preparation and member roles, minimized infant handling, improved documentation and, collectively reduced time to stabilization and completion of procedures. Sustained improvement in delivery of efficient care during RAS was feasible in a tertiary perinatal center.
References
Kattwinkel J (ed). Textbook of Neonatal Resuscitation, 5th edn. American Academy of Pediatrics and American Heart Association: Elk Grove Village, IL, USA, 2006.
Taylor RM, Price-Douglas W . The S.T.A.B.L.E. program: post resuscitation/pre transport stabilization care of sick infants. J Perinat Neonatal Nurs 2008; 22 (2): 159–165.
Wilcox L, Jedrzejek C. The Golden Hour, Implementing a Team Approach to Resuscitation of the Very Low Birth Weight (VLBW) Infant. Association of Women's Health, Obstetric and Neonatal Nurses Conference 2008, Abstract 511 C. June 21-25, 2008. AWHONN: Washington, DC, USA. Available at: https://awhonn.confex.com/awhonn/2008/webprogram/Paper2338.html (accessed on 20 September 2015).
Vento M, Aguar M, Leone TA, Finer NN, Gimeno A, Rich W et al. Using intensive care technology in the delivery room: a new concept for the resuscitation of extremely preterm neonates. Pediatrics 2008; 122 (5): 1113–1116.
Finer N, Rich W . Neonatal resuscitation for the preterm infant: evidence versus practice. J Perinatol 2010; 30 (Suppl): S57–S66.
White RD. Report of the eighth consensus conference on newborn ICU design. Consensus Committee on Recommended Design Standards for Advanced Neonatal Care: Clearwater Beach, FL, USA, 2012.
Leone TA, Rich W, Finer NN . A survey of delivery room resuscitation practices in the United States. Pediatrics 2006; 117 (2): e164–e175.
El-Naggar W, McNamara PJ . Delivery room resuscitation of preterm infants in Canada: current practice and views of neonatologists at level III centers. J Perinatol 2012; 32 (7): 491–497.
Balasubramanian BA, Cohen DJ, Davis MM, Gunn R, Dickinson LM, Miller WL et al. Learning evaluation: blending quality improvement and implementation research methods to study healthcare innovations. Implement Sci 2015; 10: 31.
Kattwinkel J (ed). Textbook of Neonatal Resuscitation, 6th edn. American Academy of Pediatrics and American Heart Association: Elk Grove Village, IL, USA, 2011.
Shahid S, Dutta S, Symington A, Shivananda S . McMaster University NICU. Standardizing umbilical catheter usage in preterm infants. Pediatrics 2014; 133 (6): e1742–e1752.
Zaharie G, Ion DA, Schmidt N, Popa M, Kudor-Szabadi L, Zaharie T . Prophylactic CPAP versus therapeutic CPAP in preterm newborns of 28-32 gestational weeks. Pneumologia 2008; 57 (1): 34–37.
Zarem C, Crapnell T, Tiltges L, Madlinger L, Reynolds L, Lukas K et al. Neonatal nurses' and therapists' perceptions of positioning for preterm infants in the neonatal intensive care unit. Neonatal Netw 2013; 32 (2): 110–116.
Shaver LF, Cone SK . Designing an orientation for staff moving to a single family room newborn intensive care unit. Newborn Infant Nurs Rev 2010; 10 (2): 87–91.
The Canadian neonatal network. Abstractor’s manual. v.2.1.1. 2013. Available at: http://www.canadianneonatalnetwork.org/Portal/LinkClick.aspx?fileticket=krvGeUTtLck%3d&tabid=69 (accessed on 23 March 2013).
Richardson DK, Corcoran JD, Escobar GJ, Lee SK . SNAP-II and SNAPPE-II: simplified newborn illness severity and mortality risk scores. J Pediatr 2001; 138 (1): 92–100.
Shewhart WA (ed). Economic Control of Quality of Manufactured Product. D. Van Nostrand Company, Inc: New York, NY, USA, 1931.
Shewhart WA, Deming WE (eds). Statistical Method from the Viewpoint of Quality Control. The Graduate school, the Department of agriculture: Washington, DC, USA, 1939.
Wheeler DJ (ed). Understanding Variation: The Key to Managing Chaos. SPC Press: Knoxville, TN, USA, 1993.
Whitfield JM, Buser MK . Transport stabilization times for neonatal and pediatric patients prior to interfacility transfer. Pediatr Emerg Care 1993; 9 (2): 69–71.
Acknowledgements
We thank the NICU staff for participating and taking ownership during the implementation of the initiative and changing their practices during resuscitation and stabilization. We thank all the neonatologists for supporting this project. We also thank the database manager Wendy Seidlitz for providing the data and David Pogorzelski for collecting data during the preimplementation phase. This study was funded by Hamilton Health Sciences Centre for Healthcare Optimization, Research and Delivery.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Journal of Perinatology website
Supplementary information
Rights and permissions
About this article

Cite this article
Shivananda, S., Gupta, S., Thomas, S. et al. Impact of a dedicated neonatal stabilization room and process changes on stabilization time. J Perinatol 37, 162–167 (2017). https://doi.org/10.1038/jp.2016.205
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jp.2016.205
This article is cited by
-
Quality improvement in the golden hour for premature infants: a scoping review
BMC Pediatrics (2024)
-
Huddles and their effectiveness at the frontlines of clinical care: a scoping review
Journal of General Internal Medicine (2021)
