
Abstract
Hexanucleotide expansion mutations in the chromosome 9 open reading frame 72 (C9orf72) gene is the most common genetic cause for frontotemporal dementia (FTD) and amyotrophic lateral sclerosis (ALS). SNP haplotype analyses have suggested that all C9orf72 expansion mutations originate from a common founder. However, not all C9orf72 expansion mutation carriers have the same haplotype. To investigate if the C9orf72 expansion mutation carriers in Sweden share a common founder, we have genotyped SNPs flanking the C9orf72 expansion mutation in cases with FTD, FTD–ALS or ALS to perform haplotype analysis. We have genotyped 57 SNPs in 232 cases of which 45 carried the C9orf72 expansion mutation. Two risk haplotypes consisting of 31 SNPs, spanning 131 kbp, were found to be significantly associated with the mutation. In summary, haplotype analysis on Swedish C9orf72 expansion mutation carriers indicates that the C9orf72 expansion mutation arose on at least two risk haplotypes.
Similar content being viewed by others

Main
A hexanucleotide, G4C2, expansion mutation in the chromosome 9 open reading frame 72 (C9orf72) gene is the most common genetic cause for frontotemporal dementia (FTD) and amyotrophic lateral sclerosis (ALS).1, 2, 3, 4, 5
The mutation frequencies of C9orf72 expansion mutations in FTD and ALS vary, with the highest frequency in European countries, especially in Finland (29% in FTD cases and 28% in ALS cases), Sweden (21% in FTD cases and 35% in ALS cases) and Spain (25% in FTD cases).2, 4, 5, 6 A common founder haplotype, of 232 kbp, has been reported in two-thirds of the Finnish C9orf72 expansion mutation carriers (MC).4, 7 European MC shared a 110 kbp haplotype which corresponds to a part of the Finnish founder haplotype.6, 8
To investigate if the high mutation frequency of C9orf72 expansion mutations in Sweden is due to a common founder we have performed genetic screening for the C9orf72 expansion mutation, using repeat-primed PCR complemented by a short tandem repeat-assay and genotyped 68 tagged SNPs (tSNPs) spanning 281 kbp on chromosome 9p21.2 in 256 patients diagnosed with FTD, FTD–ALS or ALS. The tSNPs covering three linkage disequilibrium (LD) blocks were identified in Haploview 4.2 (http://www.broadinstitute.org/mpg/haploview) using SNP data from 527 neurologically healthy controls from Sweden (provided by Professor Tomas Olsson9). Immunohistochemical staining for the detection of poly-dipeptides translated from the C9orf72 expansion mutation (NBP2-25018, Novus Biologicals, Littleton, CO, USA 1/5000) were performed on cases with available post mortem tissue from cerebellum. See Supplementary Information for details regarding the methods used.
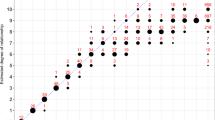
After quality control, 57 SNPs and 232 cases remained (the success rate for SNPs in the 232 cases was 98.9%). Among the cases, 45 index C9orf72 MC were detected. The demography of the cases is described in Table 1. SNPs in LD block 2 were highly associated in the C9orf72 MC (n=45) when compared to controls (n=527) (Table 2). LD block 2 includes 31 SNPs, from rs10511816 to rs2477518, and spans 131 kbp. Haploview 4.2 was used to estimate the frequencies of the most likely haplotypes based on the genotypes in C9orf72 MC and controls in LD block 2. Association analysis of the haplotype frequencies between MC and controls demonstrated two haplotypes A (P=5.2 × 10−20) and B (P=1.2 × 10−7) segregating with the C9orf72 expansion mutation (Table 3). These haplotypes differed at two SNPs (rs7868845 and rs2477518) and were found at a haplotype frequency of 39 and 16% respectively among C9orf72 expansion MC, compared with 8 and 4% of the controls. Haplotypes A and B were also confirmed by segregation analysis in additional family members. Moreover, haplotype A was found in four heterozygote C9orf72 MC who were homozygous for the A haplotype. In a UK population a similar founder haplotype was observed by Mok et al.8 However, Mok et al. allowed for both alleles C and T at both rs7868845 and rs2477518 which therefore does not distinguish between our haplotypes A and B (see Table 2). Furthermore, in cases without the expansion mutation the haplotype frequencies of A and B were similar to controls (data not shown). Three of the C9orf72 MC were observed to be heterozygous for three shorter variants of haplotypes A and B (data not shown).
Of the 57 SNPs, 29 were part of the previously reported Finnish risk-haplotype which spans 230 kbp (between rs10121765 and rs2477518), that is, which is longer than LD block 2 identified in this study in Swedish control samples (Table 2). Performing haplotype association analysis based on those 29 SNPs showed that 11 out of 45 MC in Sweden had the Finnish founder haplotype. Furthermore, there were four carriers in our cohort that were of known Finnish origin and three of them carried the founder haplotype.
The finding of two haplotypes segregating with the C9orf72 expansion mutation argues for multiples origin for the C9orf72 expansion mutation in Sweden. The most common alleles at rs7868845 and rs2477518 are C (69%) and T (71%), respectively, but none of the associated haplotypes carries this combination which is in line with the hypothesis that the mutation has arisen more than once. The most frequent haplotype A in C9orf72 MC has the minor allele T at rs7868845 and the common allele T at rs2477518 whereas haplotype B carries the opposite allele combination (C–C). However, it cannot be excluded that there was one original haplotype that gave rise to several haplotypes due to recombination and/or SNP mutation events taking place over time.
In summary, there are two significantly associated haplotypes present in the C9orf72 expansion MC indicating that there is no common founder in patients from Sweden.
References
Dejesus-Hernandez, M., Mackenzie, I. R., Boeve, B. F., Boxer, A. L., Baker, M., Rutherford, N. J. et al. Expanded GGGGCC hexanucleotide repeat in noncoding region of C9ORF72 causes chromosome 9p-linked FTD and ALS. Neuron 72, 245–256 (2011).
Gijselinck, I., Van Langenhove, T., van der Zee, J., Sleegers, K., Philtjens, S., Kleinberger, G. et al. A C9orf72 promoter repeat expansion in a Flanders-Belgian cohort with disorders of the frontotemporal lobar degeneration-amyotrophic lateral sclerosis spectrum: a gene identification study. Lancet Neurol. 11, 54–65 (2011).
Majounie, E., Renton, A. E., Mok, K., Dopper, E. G., Waite, A., Rollinson, S. et al. Frequency of the C9orf72 hexanucleotide repeat expansion in patients with amyotrophic lateral sclerosis and frontotemporal dementia: a cross-sectional study. Lancet Neurol. 11, 323–330 (2012).
Renton, A. E., Majounie, E., Waite, A., Simon-Sanchez, J., Rollinson, S., Gibbs, J. R. et al. A hexanucleotide repeat expansion in C9ORF72 is the cause of chromosome 9p21-linked ALS-FTD. Neuron 72, 257–268 (2011).
van der Zee, J., Gijselinck, I., Dillen, L., Van Langenhove, T., Theuns, J., Engelborghs, S. et al. A pan-European study of the C9orf72 repeat associated with FTLD: geographic prevalence, genomic instability, and intermediate repeats. Hum. Mutat. 34, 363–373 (2013).
Smith, B. N., Newhouse, S., Shatunov, A., Vance, C., Topp, S., Johnson, L. et al. The C9ORF72 expansion mutation is a common cause of ALS+/-FTD in Europe and has a single founder. Eur. J. Hum. Genet. 21, 102–108 (2013).
Laaksovirta, H., Peuralinna, T., Schymick, J. C., Scholz, S. W., Lai, S. L., Myllykangas, L. et al. Chromosome 9p21 in amyotrophic lateral sclerosis in Finland: a genome-wide association study. Lancet Neurol. 9, 978–985 (2010).
Mok, K., Traynor, B. J., Schymick, J., Tienari, P. J., Laaksovirta, H., Peuralinna, T. et al. Chromosome 9 ALS and FTD locus is probably derived from a single founder. Neurobiol. Aging. 33, 209.e3–8 (2012).
International Multiple Sclerosis Genetics Consortium, Wellcome Trust Case Control Consortium 2, Sawcer, S., Hellenthal, G., Pirinen, M., Spencer, C. C. et al. Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis. Nature 476, 214–219 (2011).
Acknowledgements
We thank the patients and their families included in this study. We also acknowledge Vesna Jelic at the Karolinska University hospital for her contribution in the study. Financial support was provided through the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet, Swedish Research Council, the King Gustaf V and Queen Victoria's Foundation of Freemasons, Swedish Brain Power Program, Karolinska Institutet Strategic Neuroscience Program, Gun and Bertil Stohne’s foundation, Gamla tjänarinnors foundation, Swedish Alzheimer foundation, Swedish Dementia foundation, Marianne and Marcus Wallenberg foundation, and Knut and Alice Wallenberg foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Journal of Human Genetics website
Supplementary information
Rights and permissions
About this article

Cite this article
Chiang, HH., Forsell, C., Lindström, AK. et al. No common founder for C9orf72 expansion mutation in Sweden. J Hum Genet 62, 321–324 (2017). https://doi.org/10.1038/jhg.2016.108
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2016.108
