
Abstract
A previous genome-wide association study (GWAS) reported three novel nephrolithiasis-susceptibility loci at 5q35.3, 7p14.3 and 13q14.1. Here, we investigated the association of these loci with nephrolithiasis by using an independent Japanese sample set. We performed case–control association analysis using 601 patients with nephrolithiasis and 201 control subjects. We selected seven single-nucleotide polymorphisms (SNPs): rs12654812 and rs11746443 from 5q35.3 (RGS14-SLC34A1-PFN3-F12); rs12669187 and rs1000597 from 7p14.3 (INMT-FAM188B-AQP1); and rs7981733, rs1170155, and rs4142110 from 13q14.1 (DGKH (diacylglycerol kinase)), which were previously reported to be significantly associated with nephrolithiasis. rs12654812, rs12669187 and rs7981733 were significantly associated with nephrolithiasis after Bonferroni’s correction (P=3.12 × 10−3, odds ratio (OR)=1.43; P=6.40 × 10−3, OR=1.57; and P=5.00 × 10−3, OR=1.41, respectively). Meta-analysis of current and previous GWAS results indicated a significant association with nephrolithiasis (P=7.65 × 10−15, 7.86 × 10−14 and 1.06 × 10−9, respectively). We observed a cumulative effect with these three SNPs; individuals with three or more risk alleles had a 5.9-fold higher risk for nephrolithiasis development than those with only one risk allele. Our findings elucidated the significance of genetic variation at these three loci in nephrolithiasis in the Japanese population.
Similar content being viewed by others

Introduction
Nephrolithiasis, also known as kidney stones, is a worldwide health problem that affects nearly all populations, causing severe acute back pain, and occasionally leading to more severe complications such as pyelonephritis or acute renal failure. The lifetime prevalence of nephrolithiasis in Japan is estimated to be 15.1% in men and 6.8% in women,1 with a recurrence rate of nearly 60% in patients within 10 years after their initial treatment.2
Nephrolithiasis is a multifactorial disease resulting from a complex interaction between environmental and genetic factors. Environmental factors, such as lifestyle, obesity, dietary habits and dehydration, have been implicated in nephrolithiasis development,3, 4 while hormonal, genetic or anatomical factors may also influence its pathogenesis.5 In addition, a family history of the disease has been reported to increase the disease risk in men by 2.57-fold,6 and the concordance rate of the disease in monozygotic twins has been found to be higher than that in dizygotic twins (32.4% vs 17.3%),7 suggesting a pivotal role for genetic factors as etiological factors for nephrolithiasis. Previous studies have indicated that genetic polymorphisms of the genes encoding the calcium (Ca)-sensing receptor, vitamin D receptor and osteopontin are highly correlated with kidney stone formation.8 Thus, these genetic polymorphisms are important putative markers for nephrolithiasis risk among Caucasian populations.
In 2012, a genome-wide association study (GWAS) of nephrolithiasis in the Japanese population, including 5796 patients with nephrolithiasis and 17 344 healthy controls, was performed.9 This study identified three novel loci for nephrolithiasis at 5q35.3 (RGS14-SLC34A1-PFN3-F12), 7p14.3 (INMT-FAM188B-AQP1) and 13q14.1 (DGKH).9 However, to evaluate the role of these genetic factors, a validation study using an independent case–control sample set is essential. Here, we performed a replication study using 601 nephrolithiasis and 201 control subjects.
Materials and Methods
Ethics statement
All subjects provided written informed consent. The study protocol conformed to the Declaration of Helsinki, and the study was approved by the ethical committees at the Nagoya City University Graduate School of Medical Sciences, Ijinkai Takeda General Hospital, and Sanjukai Hospital.
Subjects
The clinical characteristics of case and control samples are shown in Table 1. In total, 601 unrelated Japanese patients with nephrolithiasis (mean age±s.d., 55.0±14.0 years; 443 men and 158 women) were recruited at Nagoya City University Hospital, Ijinkai Takeda General Hospital, and Sanjukai Hospital (Table 1). Patients were excluded if they had a history of chronic urinary tract infection, renal failure, chronic diarrhea, gout, renal tubular acidosis, primary and secondary hyperparathyroidism or cancer. We excluded patients with struvite, cystine, ammonium-acid urate and uric acid stones. Patients with secondary nephrolithiasis caused by drugs, hyperparathyroidism or congenital anomalies of the urinary tract were also excluded. We also excluded anyone who had regularly taken diuretics, vitamin D or Ca supplements 1 or more times per week in the 6 months leading up to the diagnosis of Ca nephrolithiasis or the interview, because these substances may confound the results. The control group consisted of 201 Japanese subjects (mean age±s.d., 53.2±20.7 years; 166 men and 35 women) without a history of nephrolithiasis or a family history of kidney stone disease (Table 1). All control subjects underwent a medical examination and radiography (non-contrast-enhanced computed tomography) examination, along with routine blood and urine assays, for confirmation. All the patients with nephrolithiasis and the control subjects were recruited from the same racial, ethnic, geographical and environmental strata. The protocol was previously approved by the appropriate Institutional Review Boards, and informed consent was obtained from all the patients and control subjects enrolled in this study.
We assessed the effect of genetic variations on serum phosphorus, Ca, urate and creatinine levels; estimated glomerular filtration rate (eGFR); and body mass index. We analyzed a total of 230 case and control samples. In this analysis, disease status was used as a covariate. eGFR was calculated using the following formula:10 eGFR (ml min−1·1.73 m−2)=194 × serum creatinine (mg per 100 ml)−1.094 × age−0.287 ( × 0.739 for female subjects).
The subjects (601 cases and 201 controls) examined in this study were distinct populations, independent from those examined in the previous study (all samples were obtained from the BioBank Japan Project).9 We performed a meta-analysis combining data from the current study with those from the GWAS study (both cases and controls). DNA samples from the 5796 patients with nephrolithiasis and 17 344 control subjects used in the prior GWAS study9 were obtained from the BioBank Japan project, ‘the Leading Project for Personalized Medicine’ in the Ministry of Education, Culture, Sports, Science and Technology.11
DNA extraction
Genomic DNA was extracted from whole-blood samples by using a standard protocol. Whole-blood samples from patients and control subjects were centrifuged at 3000 r.p.m. for 10 min at 4 °C. The buffy coat was isolated from the blood samples. After lysis of the red blood cells in a lysis buffer, the samples were mixed in cell lysis buffer for several days. Protein precipitation solution was added to precipitate the contaminating cellular proteins. Finally, total genomic DNA was isolated by precipitation with 95% isopropanol and 80% ethanol.
Selection of single-nucleotide polymorphisms and genotyping
We selected a total of seven single-nucleotide polymorphisms (SNPs) at three loci at 5q35.3, 7p14.3 and 13q14.1, which had previously been reported to be significantly associated with nephrolithiasis (P<5 × 10−8).9
All the selected SNPs were subjected to genotyping using a multiplex PCR-Invader assay (Third Wave Technologies, Madison, WI, USA), using a detailed methodological protocol described previously.11 Multiplexed amplification was performed with 20 ng of genomic DNA. The total reaction volume of 50 μl for each sample consisted of 50 pmol of each primer, 10 units of Ex-Taq DNA polymerase and 0.55 μg of TaqStart (Clontech Laboratories, Palo Alto, CA, USA). Samples were amplified in the GeneAmp PCR system 9700 (Applied Biosystems, Foster City, CA, USA). Allele-specific oligonucleotide pairs and invasive probes were designed and supplied by Third Wave Technologies. Fluorescence resonance energy transfer probes were labeled with carboxyfluorescein (FAM) or VIC dye (Applied Biosystems), corresponding to each allele. Signal intensity was calculated as the ratio of FAM or VIC to ROX, an internal passive reference dye. The total reaction volume of 10 μl for each sample contained 0.5 μl of signal buffer, 0.5 μl of fluorescence resonance energy transfer probes, 0.5 μl of structure-specific cleavage enzyme, 1 μl of allele-specific probe mix and 2 μl of PCR product diluted 1:10 (v/v) in signal buffer. Samples were incubated at 95 °C for 5 min, followed by incubation at 63 °C for 15 min, in an ABI7900 Real Time PCR system (Applied Biosystems).
Statistical analysis
The statistical differences between the case and controls group were analyzed by the χ2-square test. The association of SNPs with nephrolithiasis was tested by a Cochran–Armitage trend test.12 We assumed a significance level of P=7.14 × 10−3 (0.05/7). The odds ratios (ORs) were calculated using the non-susceptible allele as a reference. The combined analysis of the results of this study and the previous GWAS was performed using the Mantel–Haenszel method. Heterogeneity across the two cohorts was examined using the Breslow-Day test.13 We conducted association and QTL analyses using the plink-1.06 toolset (pngu.mgh.harvard.edu/∼purcell/plink/).
Results
Genetic polymorphisms at 5q35.3, 7p14.3 and 13p14.1
The seven SNPs at 5q35.3, 7p14.3 and 13q14.1 loci, which were significantly associated with nephrolithiasis, were genotyped using the Invader assay. Table 2 shows the genotype frequencies of polymorphism among all subjects. The genotype frequencies of seven SNPs among case and control subjects were distributed in accordance with the Hardy–Weinberg equilibrium.
Each of the three loci in this study possesses a significant number of SNPs, assuming a significance level of P=7.14 × 10−3 (0.05/7). Three SNPs at three regions—SNP rs12654812 at the 5q35.3 region containing RGS14-SLC34A1-PFN3-F12 genes, rs12669187 at the 7p14.3 region containing INMT-FAM188B-AQP1 and SNP rs7981733 at the 13p14.1 locus of the DGKH region—were significantly associated with nephrolithiasis (P=3.12 × 10−3, OR=1.43; P=6.43 × 10−3, OR=1.57; and P=5.00 × 10−3, OR=1.41, respectively). As shown in Table 2, the T allele of rs12654812, the T allele of rs12669187 and the G allele of rs7981733 were found to increase the risk for nephrolithiasis development. Two SNPs—SNP rs1000597 at the 7p14.3 region and SNP rs1170155 at the 13p14.1 region—also indicated suggestive associations with nephrolithiasis (P<0.05). The risk alleles in all seven SNPs of this study are identical to those of the previous analysis.9
Next, we selected the most significant SNPs from each of the three genomic regions and examined the association of these SNPs with several clinical parameters. These SNPs did not associated with serum Ca, urate, creatinine, eGFR and body mass index levels, but the risk allele of rs12654812 was associated with lower serum phosphorus levels (P=0.0353; Table 3) although the association was not statistically significant after a multiple testing correction.
Cumulative effect of nephrolithiasis risk alleles
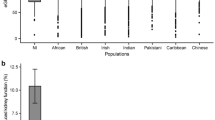
Subsequently, we examined the cumulative effects of these three SNPs (rs12654812, rs12669187, and rs7981733) in the RGS14, FAM188B and DGKH genes on nephrolithiasis susceptibility. The risk for nephrolithiasis development increased with an increasing number of risk alleles (T, T and G on rs12654812, rs12669187 and rs7981733, respectively) for three SNPs (Figure 1). Individuals with three or more risk alleles showed >5.9-fold higher risk (5.8-fold in first-stone cases and 6.4-fold in recurrent-stone cases) of developing nephrolithiasis than those with one risk allele alone. Additionally, individuals with no risk alleles showed 0.36-fold lower risk of developing nephrolithiasis than those with one risk allele. Taken together, our findings are indicative of the additive effects of variants in three loci on nephrolithiasis susceptibility.

Cumulative effect of nephrolithiasis risk alleles. (a) Distribution of risk alleles in nephrolithiasis cases (red bars) and controls (blue bars). (b) The OR for nephrolithiasis increases with increase in the number of risk alleles. The ORs are relative to the maximum number of risk alleles (number of risk allele=1) in the three SNPs (rs12654812, rs12669187, and rs7981733). The vertical bars correspond to 95% confidence interval . The horizontal line indicates the null value (OR=1).
Meta-analysis with a previous BioBank cohort
Finally, we conducted a meta-analysis of the current and the previous study (two-stage GWAS and one replication) by using a total of 5796 patients and 17 344 controls9 with a fixed-effects model using the Mantel–Haenszel method. All four stages exhibited similar trends of association. The Mantel–Haenszel P-values for independence were 7.65 × 10−15 for rs12654812 (OR=1.17; 95% confidence interval, 1.12–1.22), 7.86 × 10−14 for rs12669187 (OR=1.22; 95% confidence interval, 1.16–1.29) and 1.06 × 10−9 for rs7981733 (OR=1.15; 95% confidence interval, 1.10–1.21; Table 4).
Discussion
Nephrolithiasis is one of the most common urological diseases in the developing world. Analysis of the chemical composition of urinary stones has demonstrated that Ca oxalate stones are the most prevalent stones, occurring in ∼75–80% of cases of nephrolithiasis.1 Many case–control association studies and linkage studies have been performed to identify common genetic variations associated with nephrolithiasis. However, most of the reported variations have not been successfully reproduced experimentally. This study was performed to verify the relationship of genetic variants that were previously reported to be associated with nephrolithiasis in the Japanese population.
Here, we successfully validated three nephrolithiasis loci (5q35.5, 7p14.33 and 13q14.1) in an independent cohort. These three loci were associated with nephrolithiasis, at least in the Japanese population. Furthermore, this study showed that the accumulation of risk alleles of SNPs in these three loci increases the risk of nephrolithiasis development. The distribution of SNPs in this study was confirmed by comparison with previous GWAS data. The subjects examined in this study were independent from those of the BioBank Japan Project. As 17 344 control subjects from BioBank in previous report9 had other diseases, this complex background of control subjects may lead to false-positive or false-negative results. In contrast, nephrolithiasis was specifically excluded in our 201 control samples by medical examination (computed tomography and ultrasonography). In this replication study, the three loci showed a stronger association (OR, 1.43, 1.57 and 1.41) than those reported in the previous GWAS. Thus, these three SNPs are common nephrolithiasis loci in the Japanese population.
The results of an analysis of the protein-encoding genes near the 5q35.3, 7p14.3 and 13q14.1 loci are suggestive of several intriguing potential associations with nephrolithiasis. The SLC34A1 gene located in the RGS14-SLC34A1-PFN3-F12 region encodes NPT2a, a member of the type IIa sodium-phosphate cotransporter family, which is highly expressed in the kidney.14 The NPT2a protein family, located on the apical membrane of renal proximal tubular epithelial cells, is essential in maintaining phosphate homeostasis. Mutations in SLC34A1 have been reported to cause hypophosphatemic nephrolithiasis and osteoporosis in humans15 and severe renal phosphate wasting and hypercalciuria in mice.16 In addition, previously published GWAS reports revealed the association of variations in the SLC34A1 locus with kidney function17 and serum phosphorus concentration.18 In the QTL analyses in this study, rs12654812, located near SLC34A1, was associated with serum phosphorus levels. This result is consistent with the results of a previous study in which variants near SLC34A1 were associated with serum phosphorus levels.18 The SLC34A1 mutation was also shown to reduce renal phosphate resorption and recurrent nephrolithiasis.19 As SLC34A1 encodes the protein NPT2, a member of the type II sodium-phosphate cotransporter family, the presence of SNP rs12654812 is associated with reduced NPT2 function, resulting in subsequent reduction of serum phosphorus levels and an increased risk of nephrolithiasis development.
Targeted deletion of the Npt2a gene in mice resulted in increased urinary excretion of inorganic phosphate (Pi), an ∼80% decrease in renal brush border membrane Na/Pi cotransport, and hypophosphatemia, which leads to increased levels of serum calcitriol (1,25(OH)2D, a biologically active vitamin D metabolite), intestinal Ca channel overexpression, increased intestinal Ca hyperabsorption, hypercalcemia and hypercalciuria. NPT2a null mice develop renal deposits of apatitic Ca phosphate,18 a primary constituent of idiopathic Ca oxalate stones.20 Ca oxalate stones develop while attached to Randall’s plaques or Ca phosphate crystal deposits in renal tubules.21 Randall’s plaques are composed of poorly crystalline biologically active Ca phosphate, reported to begin at the basement membrane of the loops of Henle.22, 23 Ultrastructural investigation of Npt2a null mice uncovered the Ca phosphate crystals formed in the tubular lumina; these crystals were organized as microspheres. It has been suggested that variations in this region could regulate renal function and subsequently affect the risk of nephrolithiasis development.
In the previous study, rs11746443 at 5q35.3 was significantly associated with the reduction in eGFR by QTL analysis.9 However, we found no significant association with eGFR in this study. This could be partially explained by the smaller sample size in this study (n=229) compared with that of previous study (n=27 323).
The SNPs rs12669187 and rs1000597 on chromosome 7p14.3 are located on the FAM188B gene and between the FAM188B gene (5.2 kb downstream), and the AQP1 gene (14.2 kb upstream), respectively. However, the role of FAM188B in the pathogenesis of nephrolithiasis has not yet been elucidated. Aquaporin-1 is abundantly expressed in the kidney, functioning as a water channel.24 Moreover, Aqp1 null mice exhibit reduced osmotic permeability in the membrane of the kidney proximal tube and become severely dehydrated after water deprivation, suggesting an important role for aquaporin-1 in the urinary concentration mechanism.24 Therefore, the SNPs rs12669187 and rs1000597 are likely to be associated with the regulation of FAM188B and/or AQP1 expression and may affect the urine concentration process and increase the risk of nephrolithiasis development.
The SNP rs7981733 on DGKH is significantly associated with nephrolithiasis. DGKH, which is highly expressed in the brain, is potentially associated with psychiatric disorders such as bipolar disorder and major depressive disease,25 but its involvement in renal function or Ca homeostasis has not been reported previously. Therefore, further functional analyses are essential to elucidate the role of this variation as a causative factor for nephrolithiasis.
During examination of the cumulative effect of three SNPs in RGS14, FAM188B and DGKH, 1 risk allele was found to be the most common (35%) in control subjects. The risk of nephrolithiasis development increases with increase in the frequency of risk alleles for the three SNPs (Figure 1). In addition, patients with recurrent stones exhibited higher ORs (OR=6.4) than patients who had developed a stone for the first time (OR=5.8). Our findings clearly indicate the existence of an additive effect of these three variants on nephrolithiasis susceptibility; therefore, SNP analysis would be an effective predictor of nephrolithiasis risk and recurrence.
The previous GWAS data in Caucasian populations showed that CLDN14 is associated with nephrolithiasis.26 In the Japanese population, SNP rs2835349, located 19 kb upstream of the CLDN14 gene, exhibited a probable association with the CLDN14 gene (P=6.33 × 10−5; OR=1.22) in the GWAS stage.9 However this SNP was not identified in the replication cohort (P=0.624; OR=0.98). Thus, the CLDN14 gene is unlikely to have a strong impact on nephrolithiasis development in the Japanese population. Furthermore, another genome-wide meta-analysis has shown that Ca-sensing receptor variants are associated with serum Ca level in Caucasians and Indian Asian27 However, SNPs in the CASR gene was not associated with nephrolithiasis risk in the previous GWAS (data not shown).9
In agreement with the aforementioned findings, associations between the three novel loci (identified by GWAS and replication studies) and nephrolithiasis were observed. Our results helped elucidate the crucial roles of genetic factors related to nephrolithiasis development. Furthermore, functional analysis is necessary to completely elucidate the role of these variations in the development of nephrolithiasis.
References
Yasui, T., Iguchi, M., Suzuki, S. & Kohri, K. Prevalence and epidemiological characteristics of urolithiasis in Japan: national trends between 1965 and 2005. Urology 71, 209–213 (2008).
Strohmaier, W. L. Course of calcium stone disease without treatment. What can we expect? Eur. Urol. 37, 339–344 (2000).
Tasca, A. Metabolic syndrome and bariatric surgery in stone disease etiology. Curr. Opin. Urol. 21, 129–133 (2011).
Taylor, E. N., Stampfer, M. J. & Curhan, G. C. Obesity, weight gain, and the risk of kidney stones. J. Am. Med. Assoc. 293, 455–462 (2005).
Worcester, E. M. & Coe, F. L. Clinical practice. Calcium kidney stones. N. Engl. J. Med. 363, 954–963 (2010).
Curhan, G. C., Willett, W. C., Rimm, E. B. & Stampfer, M. J. Family history and risk of kidney stones. J. Am. Soc. Nephrol. 8, 1568–1573 (1997).
Goldfarb, D. S., Fischer, M. E., Keich, Y. & Goldberg, J. A twin study of genetic and dietary influences on nephrolithiasis: a report from the Vietnam EraTwin (VET) Registry. Kidney Int. 67, 1053–1061 (2005).
Vezzoli, G., Terranegra, A., Arcidiacono, T. & Soldati, L. Genetics and calcium nephrolithiasis. Kidney Int. 80, 587–593 (2011).
Urabe, Y., Tanikawa, C., Takahashi, A., Okada, Y., Morizono, T., Tsunoda, T. et al. A genome-wide association study of nephrolithiasis in the Japanese population identifies novel susceptible Loci at 5q35.3, 7p14.3, and 13q14.1. PLoS Genet. 8, e1002541 (2012).
Matsuo, S., Imai, E., Horio, M., Yasuda, Y., Tomita, K., Nitta, K. et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 53, 982–992 (2009).
Nakamura, Y. The BioBank Japan Project. Clin. Adv. Hematol. Oncol. 5, 696–697 (2007).
Purcell, S., Neale, B., Todd-Brown, K., Thomas, L., Ferreira, M. A., Bender, D. et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 81, 559–575 (2007).
Breslow, N. E. & Day, N. E. Statistical methods in cancer research. Volume II—The design and analysis of cohort studies. IARC Sci. Publ. 82, 1–406 (1987).
Weinman, E. J., Cunningham, R., Wade, J. B. & Shenolikar, S. The role of NHERF-1 in the regulation of renal proximal tubule sodium-hydrogen exchanger 3 and sodium-dependent phosphate cotransporter 2a. J. Physiol. 567, 27–32 (2005).
Prié, D., Huart, V., Bakouh, N., Planelles, G., Dellis, O., Gérard, B. et al. Nephrolithiasis and osteoporosis associated with hypophosphatemia caused by mutations in the type 2a sodium-phosphate cotransporter. N. Engl. J. Med. 347, 983–991 (2002).
Beck, L., Karaplis, A. C., Amizuka, N., Hewson, A. S., Ozawa, H., Tenenhouse, H. S. et al. Targeted inactivation of Npt2 in mice leads to severe renal phosphate wasting, hypercalciuria, and skeletal abnormalities. Proc. Natl Acad. Sci. USA 95, 5372–5377 (1998).
Köttgen, A., Pattaro, C., Böger, C. A., Fuchsberger, C., Olden, M., Glazer, N. L. et al. New loci associated with kidney function and chronic kidney disease. Nat. Genet. 42, 376–384 (2010).
Kestenbaum, B., Glazer, N. L., Köttgen, A., Felix, J. F., Hwang, S. J., Liu, Y. et al. Common genetic variants associate with serum phosphorus concentration. J. Am. Soc. Nephrol. 21, 1223–1232 (2010).
Lapointe, J. Y., Tessier, J., Paquette, Y., Wallendorff, B., Coady, M. J., Pichette, V. et al. NPT2a gene variation in calcium nephrolithiasis with renal phosphate leak. Kidney Int. 69, 2261–2267 (2006).
Khan, S. R. Calcium phosphate/calcium oxalate crystal association in urinary stones: implications for heterogeneous nucleation of calcium oxalate. J. Urol. 157, 376–383 (1997).
Coe, F. L., Evan, A. P., Worcester, E. M. & Lingeman, J. E. Three pathways for human kidney stone formation. Urol. Res. 38, 147–160 (2010).
Randall, A. The origin and growth of renal calculi. Ann. Surg. 105, 1009–1027 (1937).
Evan, A. P., Lingeman, J. E., Coe, F. L., Parks, J. H., Bledsoe, S. B., Shao, Y. et al. Randall's plaque of patients with nephrolithiasis begins in basement membranes of thin loops of Henle. J. Clin. Invest. 111, 607–616 (2003).
Ma, T., Yang, B., Gillespie, A., Carlson, E. J., Epstein, C. J. & Verkman, A. S. Severely impaired urinary concentrating ability in transgenic mice lacking aquaporin-1 water channels. J. Biol. Chem. 273, 4296–4299 (1998).
Barnett, J. H. & Smoller, J. W. The genetics of bipolar disorder. Neuroscience 164, 331–343 (2009).
Thorleifsson, G., Holm, H., Edvardsson, V., Walters, G. B., Styrkarsdottir, U., Gudbjartsson, D. F. et al. Sequence variants in the CLDN14 gene associate with kidney stones and bone mineral density. Nat. Genet. 41, 926–930 (2009).
Kapur, K., Johnson, T., Beckmann, N. D., Sehmi, J., Tanaka, T., Kutalik, Z. et al. Genome-wide meta-analysis for serum calcium identifies significantly associated SNPs near the calcium-sensing receptor (CASR) gene. PLoS Genet. 6, e1001035 (2010).
Acknowledgements
We thank Ms Ichikawa, Ms Kawamura, Ms Noda and Ms Kasuga for their secretarial assistance. This work was partly supported by MEXT/JSPSKAKENHI (grant numbers 23249074, 23592375, 24659716 and 24689060); the BioBank Japan Project funded by the Japanese Ministry of Education, Culture, Sports, Science and Technology; the Takeda Science Foundation; and the Japanese Urological Association. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Yasui, T., Okada, A., Urabe, Y. et al. A replication study for three nephrolithiasis loci at 5q35.3, 7p14.3 and 13q14.1 in the Japanese population. J Hum Genet 58, 588–593 (2013). https://doi.org/10.1038/jhg.2013.59
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2013.59
Keywords
This article is cited by
-
The rs1256328 (ALPL) and rs12654812 (RGS14) Polymorphisms are Associated with Susceptibility to Calcium Nephrolithiasis in a Taiwanese population
Scientific Reports (2019)
-
Renal phosphate handling and inherited disorders of phosphate reabsorption: an update
Pediatric Nephrology (2019)
-
Clinical aspects of the phosphate transporters NaPi-IIa and NaPi-IIb: mutations and disease associations
Pflügers Archiv - European Journal of Physiology (2019)
-
Meeting report of the “Symposium on kidney stones and mineral metabolism: calcium kidney stones in 2017”
Journal of Nephrology (2019)
-
Association Study of Reported Significant Loci at 5q35.3, 7p14.3, 13q14.1 and 16p12.3 with Urolithiasis in Chinese Han Ethnicity
Scientific Reports (2017)
