
Abstract
Patients with X-linked agammaglobulinemia (XLA) can present with sensorineural deafness. This can result from a gross deletion that not only involved the Bruton's tyrosine kinase (BTK) gene, but also TIMM8A, mutations in which underlie the Mohr-Tranebjærg syndrome (MTS). We analyzed the genomic break points observed in three XLA–MTS patients and compared these with deletions break points from XLA patients. Patient 1 had a 63-kb deletion with break points in intron 15 of BTK and 4 kb upstream of TAF7L. Patients 2 and 3 had 149.7 and 196 kb deletions comprising BTK, TIMM8A, TAF7L and DRP2. The break points in patients 1 and 3 were located in Alu and endogenous retrovirus (ERV) repeats, whereas the break points in patient 2 did not show involvement of transposable elements. Comparison of gross deletion sizes and involvement of transposable elements in XLA and XLA–MTS patients from the literature showed preferential involvement of Alu elements in smaller deletions (<10 kb). These results show further insights into the molecular mechanisms underlying gross deletions in patients with primary immunodeficiency.
Similar content being viewed by others

Introduction
X-linked agammaglobulinemia (XLA) is an inherited primary immunodeficiency characterized by early onset of recurrent bacterial infections, profound hypogammaglobulinemia and markedly reduced circulating B cells.1 The gene responsible for XLA was identified in 1993,2, 3 and named Bruton's tyrosine kinase (BTK). The BTK gene is mapped to the Xq21.3–Xq22 region, encompasses 37.5 kb of genomic DNA and contains 19 exons (the initiation codon is in exon 2). Only 770 bp centromerically of the BTK gene is the gene TIMM8A (formerly DDP1) located; it consists of two exons and produces a 97 amino acid polypeptide.4 Mutations in TIMM8A cause the rare X-linked neurodegenerative Mohr-Tranebjærg syndrome (MTS), which is clinically characterized by a progressive neurological deficits, including early onset of sensorineural deafness.5, 6, 7
A large number of BTK mutations, scattered over the entire gene, have been reported and deposited in an international mutation database (http://bioinf.uta.fi/BTKbase/). The most commonly found mutations are missense (34%), followed by nonsense mutations (20%). Mutations affecting splice sites were reported in 18% and small insertions and deletions in another 18% of XLA families. Disruption of the BTK gene by gross deletions occurs in about 3.5% of XLA families.1 As BTK and TIMM8A are positioned in close genomic proximity, gross gene deletions can result in disruption of both genes causing a contiguous deletion syndrome of XLA and MTS, which has been observed previously in nine families.4, 8, 9, 10
In this study, we describe three patients with gross deletions including the BTK and TIMM8A genes. We characterized the deletions and identified the genomic break points by combining comparative genomic hybridization (CGH) array, DNA fluorescence in situ hybridization (FISH) and long accurate (LA)-PCR analyses. The results of these investigations provide new insight into the genetic mechanisms causing the XLA–MTS deletion syndrome and allow accurate genetic analysis of patients and carriers.
Materials and methods
Patients
Patient 1 is a 15-year-old Japanese boy without a family history of immunodeficiency or neurological deficits. He was diagnosed with XLA at 7 years of age when he developed recurrent bacterial infections. Deafness was noticed 1 year earlier and gradually worsened.
Patient 2 is a 10-year-old Japanese boy, who has a history of recurrent otitis media and sinusitis since 12 months of age. He had been diagnosed with deafness and autism at 18 months of age. Agammaglobulinemia and lack of circulating B cells were recognized at 8 years of age, and was diagnosed with XLA.
Both patients are doing well on immunoglobulin replacement therapy. They have no dystonia, but their hearing losses are severe and progressive.
Patient 3 corresponds to patient 6 who was described in a previous report.9 He was diagnosed with XLA at 8 months of age, and was found to have sensorineural hearing loss at 3 years of age. Genetic analysis resulted in the identification of a gross deletion involved the entire coding regions of the BTK, TIMM8A, TAF7L and DRP2 genes.
Gene analysis of BTK
Informed consent for genetic analysis was obtained from the patients and their parents under a protocol approved by the Institutional Review Board of University of Toyama. BTK mutation analysis was performed by direct sequencing of complementary DNA and all 19 exons and exon–intron boundaries using genomic DNA as described previously.11, 12
Fluorescence in situ hybridization
Peripheral blood mononuclear cells from patients and controls were stimulated in culture with phytohemagglutinin for 72 h, followed by treatment with a 0.075 M. KCl solution and fixation with Carnoy's solution (3:1 methanol and acetic acid) for metaphase preparation. A BTK–TIMM8A-specific genomic probe (5231 bp long) was prepared using the LA-PCR Kit (Takara, Kyoto, Japan) with primer pairs reflecting exon 19 of BTK and exon 2 of TIMM8A (5′-AGCATTCTGGCATGAATGTTCCCTGAAC-3′ and 5′-ATCTCTCCGGGTTGCAGATAATAACTG C-3′, respectively). In addition, probes were designed to detect the TAF7L and DRP2 genes, which are located centromerically of TMM8A. The TAF7L- and DRP2-specific genomic probes (5662 and 5975 bp) were prepared similarly by LA-PCR Kit (Takara) with primers derived from exons 2 and 5 of TAF7L (5′-GCTTAGGTAGCCACCAACGTGTTGTTGA-3′ and 5′-GACGTCCCTGTTTCACAAGGAATTAGGA-3′) and from exons 7 and 12 of DRP2 (5′-CGTGACTGTATTAAAGGGCTCAACCATG-3′ and 5′-GCAGTACTTCCTGTCACAAAGCAGTTGC-3′), respectively. For FISH analysis, denatured metaphase spreads were hybridized with probes labeled with digoxigenin-11-deoxyuridine triphosphate using a nick translation kit (Roche Diagnostics KK, Tokyo, Japan). The Spectrum Green-labeled X-chromosome probe (DXZ1, Abbott Japan, Tokyo, Japan) was used as a control. The BTK–TIMM8A-, TAF7L- and DRP2-specific probes were detected with anti-digoxigenin rhodamine (Roche Diagnostics KK) providing a red signal, whereas DXZ1 was detected by a green signal. Metaphases were counterstained with 4′, 6-diamino-2-phenylindole dihydrochloride, and the images of the hybridization captured by fluorescence microscopy (Carl Zeiss Co., Tokyo, Japan). At least 20 metaphases were observed in each setting.
Array CGH analysis
Array CGH analysis was performed using the Agilent kit (Agilent Technologies, Palo Alto, CA, USA) as described.13 A total of 1 μg DNA from patients and male controls were double-digested with RsaI and AluI for 4 h at 37 °C. After column purification, each digested sample was labeled by random priming for 2 h using Cy3-deoxyuridine triphosphate for the patient DNA and Cy5-deoxyuridine triphosphate for the control DNA. Labeled products were purified by Microcon YM-30 filter units (Millipore, Billerica, MA, USA). After probe determination and pre-annealing with Cot-1 DNA (Invitrogen, Carlsbad, CA, USA), hybridization was performed at 65 °C with rotation for 40 h. The hybridized array was analyzed with the Agilent scanner and the Feature Extraction software (v9.5.3.1; Agilent). A graphical overview was obtained using the CGH analytics software (v3.5.14; Agilent). The UCSC Genome Browser was used to retrieve the reference genome sequence (http://www.genome.ucsc.edu).
LA-PCR and sequencing
LA-PCR reaction was performed with the appropriate forward and reverse primers that were used to map the gross deletion boundaries as described previously.14 PCR products were excised from the gel, purified with the QIAquick Gel Extraction Kit (Qiagen, Valencia, CA, USA), and sequenced on ABI Prism 3130XL sequence detection system (Applied Biosystems, Foster City, CA, USA).
Results
BTK mutation analysis
PCR analysis of genomic DNA resulted in the amplification of BTK exons 1–15, but not of exons 16–19 in patient 1, and amplifications of exons 1–5, but not of exons 6–19 in patient 2.
FISH analysis
To confirm a large deletion in the BTK gene and to investigate a possible deletion of the TIMM8A gene, we performed FISH analysis with a BTK–TIMM8A-specific probe. Cells from both patients 1 and 2 lacked signals of this probe (Figures 1a and b), indicating a contiguous gene deletion syndrome of XLA and MTS. To study the extent of the deletion further, we performed additional FISH experiments using TAF7L- and DRP2-specific probes. Lymphocytes from patient 1 showed normal signals for both probes (Figures 1d and g), but cells from patient 2 failed to give signals for either TAF7L or for DRP2 (Figures 1e and h). We conclude that the genomic deletion in patient 1 is restricted to the BTK and TIMM8A genes, whereas the deletion in patient 2 is considerably larger involving TAF7L and DRP2.

Identification of multigene detections by fluorescence in situ hybridization analysis with Bruton's tyrosine kinase (BTK)–TIMM8A- (a–c), TAF7L- (d–f) and DRP2-specific probes (g–i) and the X-chromosome-specific DXZ1 probe in patient 1 (a, d and g), patient 2 (b, e and h) and healthy male control (c, f and i). The DZX1 probe is shown in green (arrow heads), whereas the BTK–TIMM8A, TAF7L and DRP2 probes are shown in red (arrows).
Array CGH analysis
To study the extent of the deletions in patients 1 and 2, we performed array CGH analysis of genomic DNA. In patient 1, we found an interstitial loss in copy number in the Xq22 region, involving the BTK and TMM8A genes, spanning a minimum of 63 kb (Figure 2). In patient 2, we observed a deletion of at least 138 kb including the BTK, TIMM8A, TAF7L and DRP2 genes (Figure 2). These results confirmed the FISH analysis of patient 1 having a deletion of BTK and TIMM8A, and of patient 2 having a deletion involving the BTK, TIMM8A, TAF7L and DRP2 genes, similar to what was found for patient 3.9

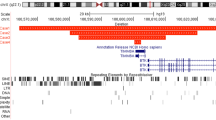
Array comparative genomic hybridization analysis of the X-chromosomes of patient 1 (upper panel) and patient 2 (lower panel). Grey belts indicate regions of continuously reduced copy number around Xq22. Upper panel discloses a deletion of at least 65.8 kb including the Bruton's tyrosine kinase (BTK) and TIMM8A genes in patient 1, and lower panel discloses a deletion of at least 138 kb including the BTK, TIMM8A, TAF7L and DRP2 genes in patient 2. A full color version of this figure is available at the Journal of Human Genetics journal online.
Analysis of the break point junctions
On the basis of FISH and array CGH results, PCR primers were designed to span the putative break points. Sequence analysis of the PCR products from patient 1 revealed that recombination had occurred between a site in intron 15 of BTK and a site 4.4 kb upstream of TAL7L (Figure 3). It is an unequal crossover, which shares a 22-bp stretch of 100% homology and resulted in the deletion of 63 kb. To determine whether the break points were located in transposable elements, we analyzed the ±1000 bp genomic sequences flanking the break point regions against reference collection repeats.15 The results revealed that both the distal and proximal deletion break points of patient 1 are located within short interspersed element of the Alu subclass (Figure 4).

Sequences of the gross deletion break point junctions of three patients compared with control sequences. The upper, middle and lower panels indicate patient 1, patient 2 and patient 3. Microhomology regions at the junctions are boxed. BTK, Bruton's tyrosine kinase.

A ±1000 bp flanking the gross deletion break points of patient 1 (upper panel), patient 2 (middle panel) and patient 3 (lower panel). Besides coding elements, four types of transposable elements are indicated: DNA transposons, endogenous retrovirus (ERV), long interspersed element (LINE) and short interspersed element (SINE). BTK, Bruton's tyrosine kinase.
In patient 2, the deletion extended from a site 4.4 kb upstream of DRP2 to a site in intron 5 of BTK, encompassing 149.7 kb (Figure 3). Break point junction analysis revealed 3 bp microhomology between the two break point regions. Neither of the break points was located in DNA sequences derived from transposable elements (Figure 4).
The gross deletion in patient 3 encompassed 196 kb, and the junction showed microhomology between the 5′ and 3′ break points (Figure 3). The 5′ break point was located upstream of the DRP2 gene in a repeat derived from an endogenous retrovirus 2 (ERV2), whereas the 3′ break point in intron 1 of BTK was not located in a transposable element, but close to an Alu element (Figure 4).
Thus, two of the three break point regions of the XLA–MTS patients we studied showed involvement of transposable elements. Although six out of eight break points of BTK deletions were found to be located in an Alu element in previous studies,14, 16, 17 we observed Alu element involvement only in patient 1.
Transposable element involvement in XLA and XLA–MTS
It was previously shown that BTK gross deletion break points were frequently located in Alu elements. To study whether gross deletions resulting in XLA or XLA–MTS are derived from similar deletion mechanisms, we analyzed all reported gross deletions in XLA and XLA–MTS patients (Figure 5).9, 14, 16, 17 Including our patients, we collected data from five XLA and six XLA–MTS deletions. The deletion size clearly differed: XLA–MTS patients, as expected, had much larger disease-causing deletions. As BTK and TIMM8A are in close genomic proximity, a deletion <10 kb can already disrupt both genes.

Schematic representation of all molecularly characterized gross deletions in patients with XLA and XLA–MTS. The patients are listed according to the size of the gross deletion and for each patient, the disorder (XLA or XLA–MTS) is given as well as the involvement of transposable elements. BTK, Bruton's tyrosine kinase; ERV, endogenous retrovirus; LINE, long interspersed element; MTS, Mohr-Tranebjærg syndrome; XLA, X-linked agammaglobulinemia.
Interestingly, all deletions <10 kb involved Alu elements, whereas only two out of six deletions >10 kb had break points located in Alu elements (Figure 5). These results imply that Alu elements are more frequently associated with smaller deletions, whereas other elements, such as long interspersed elements and ERV elements, seem to be more frequently associated with larger deletions. As XLA–MTS deletions are on average larger than XLA deletions, they show less frequently involvement of Alu elements.
Discussion
The contiguous gene deletion syndrome involving BTK and TIMM8A has previously been described in 12 patients from nine unrelated families with deletion sizes ranging from 20–196 kb.8, 9, 10 Of these, only three break point junctions have been cloned.14, 16 In this study, we describe three patients with 63, 150 and 196 kb large deletions at the Xq22 region, which included BTK and TIMM8A.
Short interspersed elements of the Alu subclass are the most frequently occurring interspersed repeat elements in the human genome: the 280-bp sequence occurs approximately every 4 kb in the human genome.18 Mispairing between such repeats has been shown to be frequent causes of deletions and duplications. Alu/Alu-mediated genomic rearrangements are classical homologous recombination that result in a loss or gain in the number of nucleotide bases, causing approximately 0.3% of human genetic diseases.19, 20 Recently, the break point junctions of eight XLA patients with a BTK gross deletion were analyzed for the presence of transposon-derived repetitive elements. Most of the break points were located in Alu elements.14 These observations have suggested a general role for Alu sequences in promoting recombination in the BTK gene. Besides deletions, Alu-mediated recombination may also promote genomic duplications in BTK, depending on how the break points are joined.16 The 5′ and 3′ break points in patient 1 were located in Alu elements, similar to most XLA patients with gross deletions affecting the BTK gene.14, 16, 17 The break points of patients 2 and 3, however, were not located in Alu elements, and, intriguingly, the homology regions were very small repeat fragments of only 3 or 5 bp nucleotides, implying that the deletion was not due to an unequal homologous recombination.
A comparison of the deletion size and the presence of transposable elements resulting in gross deletions causing XLA and XLA–MTS strongly suggests that Alu elements are mainly involved in <10 kb deletions. As most deletions underlying XLA–MTS are >10 kb, the involvement of Alu elements in deletions causing XLA–MTS is less frequent than in those associated with XLA. Thus, it is likely that the majority of the deletions underlying XLA–MTS arise from mechanisms that are different from those underlying XLA.
We used a combined approach of DNA FISH, array CGH and LA-PCR to characterize the break point regions in our patients and clone the break point regions. In doing so, we were able to establish a genetic basis of the disease. This is important for patient care with respect to genetic counseling and carriership analysis in family members. Wide use of DNA FISH and array CGH analysis to establish genetic abnormalities will support higher rates of gross lesions. This will not contribute to patient care, but to general understanding of complexity and frequency of these types of genetic lesions.
In patients 2 and 3, the TAF7L and DRP2 genes were deleted in addition to BTK and TIMM8A. TAF7L encodes an RNA polymerase II TATA-box-binding protein-associated factor II protein, which is expressed only in male spermatogonia and may have a role in pre-meiotic stages of mammalian spermatogenesi.21 The DRP2 gene encodes the dystrophin-related protein 2, which is a member of the dystrophin family of proteins performing a critical role in the maintenance of membrane-associated complexes at points of intercellular contact in vertebrate cells.22 It is expressed principally in the brain and spinal cord. Disruption of the DRP2-dystroglycan complex is followed by hypermyelination and destabilization of the Schwann cell-axon unit in Prx (−/−) mice.23 However, no human pathology has been reported due to any mutation in these genes. Both patients presented with recurrent infections and hearing loss as typical symptoms of contiguous gene deletion syndrome of XLA and MTS, and showed no pathological findings which might be associated with the deletion of TAF7L and DRP2 genes. Therefore, these genes might not have a critical function in humans or other proteins might compensate for their loss.
In conclusion, sensorineural hearing loss in XLA should raise concerns about a possible contiguous gene deletion syndrome. Array CGH analysis combined with FISH analysis can provide a more accurate diagnosis of large deletions. Not only transposable elements and microhomology, but also other mechanisms may contribute to gross rearrangements involving the BTK gene.
References
Conley, M. E., Broides, A., Hernadez-Trujillo, V., Howard, V., Kanegane, H., Miyawaki, T. et al. Genetic analysis of patients with defects in early B-cell development. Immunol. Res. 203, 216–234 (2005).
Tsukada, S., Saffran, D. C., Rawlings, D. J., Parolini, O., Allen, R. C., Klisak, I. et al. Deficient expression of a B cell cytoplasmic tyrosine kinase in human X-linked agammaglobulinemia. Cell 172, 279–290 (1993).
Vetrie, D., Vořechovský, I., Sideras, P., Holland, J., Davies, A., Flinter, F. et al. The gene involved in X-linked agammaglobulinaemia is a member of the src family of protein-tyrosine kinases. Nature 361, 226–233 (1993).
Vořechovský, I., Vetrie, D., Holland, J., Bentley, D. R., Thomas, K., Zhou, J. N. et al. Isolation of cosmid and cDNA clones in the region surrounding the BTK gene at Xq21.3-q22. Genomics 21, 517–524 (1994).
Jin, H., May, M., Tranebjærg, L., Kendall, E., Fontán, G., Jackson, J. et al. A novel X-linked gene, DDP, shows mutations in families with deafness (DFN-1), dystonia, mental deficiency and blindness. Nat. Genet. 14, 177–180 (1996).
Tranebjærg, L., Hamel, B. C. J., Gabreels, F. J. M., Renier, W. O. & Van Ghelue, M. A de novo missense mutation in a critical domain of the X-linked DDP gene causes the typical deafness-dystonia-optic atrophy syndrome. Eur. J. Hum. Genet. 8, 464–467 (2000).
Binder, J., Hofmann, S., Kreisel, S., Wöhrle, J. C., Bäzner, H., Krauss, J. K. et al. Clinical and molecular findings in a patient with a novel mutation in the deafness-dystonia peptide (DDP1) gene. Brain 126, 1814–1820 (2003).
Richter, D., Conley, M. E., Rohrer, J., Myers, L. A., Zahradka, K., Kelecić, J. et al. A contiguous deletion syndrome of X-linked agammaglobulinemia and sensorineural deafness. Pediatr. Allergy Immunol. 12, 107–111 (2001).
Šedivá, A., Smith, C. I. E., Asplund, A. C., Hadač, J., Janda, A., Zeman, J. et al. Contiguous X-chromosome deletion syndrome encompassing the BTK, TIMM8A, TAF7L and DRP2 genes. J. Clin. Immunol. 27, 640–646 (2007).
Jyonouchi, H., Geng, L., Törüner, G. A., Vinekar, K., Feng, D. & Fitzgerald-Bocarsly, P. Monozygous twins with a microdeletion syndrome involving BTK, DDP1, and two other genes; evidence of intact dendritic cell development and TLR responses. Eur. J. Pediatr. 167, 317–321 (2008).
Hashimoto, S., Tsukada, S., Matsushita, M., Miyawaki, T., Niida, Y., Yachie, A. et al. Identification of Bruton's tyrosine kinase (Btk) gene mutations and characterization of the derived proteins in 35 X-linked agammaglobulinemia families: a nationwide study of Btk deficiency in Japan. Blood 88, 561–573 (1996).
Kanegane, H., Futatani, T., Wang, Y., Nomura, K., Shinozaki, K., Matsukura, H. et al. Clinical and mutational characteristics of X-linked agammaglobulinemia and its carrier identified by flow cytometric assessment combined with genetic analysis. J. Allergy Clin. Immunol. 108, 1012–1020 (2001).
Yamada, M., Arai, T., Oishi, T., Hanano, N., Kobayashi, I., Kubota, M. et al. Determination of the deletion breakpoints in two patients with contiguous gene syndrome encompassing CYBB gene. Eur. J. Med. Genet. 53, 383–388 (2010).
van Zelm, M. C., Geertsema, C., Nieuwenhuis, N., de Ridder, D., Conley, M. E., Schiff, C. et al. Gross deletions involving IGHM, BTK, or Artemis: a model for genomic lesions mediated by transposable elements. Am. J. Hum. Genet. 82, 320–332 (2008).
Kohany, O., Gentles, A. J., Hankus, J. & Jurka, J. Annonation, submission and screening of repetitive elements in Repbase: RepbaseSubmitter and Cancer. BMC Bioinformatics 7, 474 (2006).
Rohrer, J., Minegishi, Y., Richter, D., Eguiguren, J. & Conley, M. E. Unusual mutations in Btk: an insertion, a duplication, an inversion and four large deletions. Clin. Immunol. 90, 28–37 (1999).
Jo, E. K., Wang, Y., Kanegane, H., Futatani, T., Song, C. H., Park, J. K. et al. Identification of mutations in the Bruton's tyrosine kinase gene, including a novel genomic rearrangements resulting in large deletion, in Korean X-linked agammaglobulinemia patients. J. Hum. Genet. 48, 322–326 (2003).
International Human Genome Sequencing Consortium. Initial sequencing and analysis of the human genome. Nature 409, 860–921 (2001).
Purandare, S. M. & Patel, P. I. Recombination hot spots and human disease. Genome Res. 7, 773–786 (1997).
Deininger, P. L. & Batzer, M. A. Alu repeats and human disease. Mol. Genet. Metab. 67, 183–193 (1999).
Wang, P. J., McCarrey, J. R., Yang, F. & Page, D. C. An abundance of X-linked genes expressed in spermatogonia. Nat. Genet. 27, 422–426 (2001).
Roberts, R. G., Freeman, T. C., Kendall, E., Vetrie, D. L., Dixon, A. K., Shaw-Smith, C. et al. Characterization of DRP2, a novel human dystrophin homologue. Nat. Genet. 13, 223–226 (1996).
Sherman, D. L., Fabrizi, C., Gillespie, C. S. & Brophy, P. J. Specific disruption of a Schwann cell dystrophin-related protein complex in a demyelinating neuropathy. Neuron 30, 677–687 (2001).
Acknowledgements
This study was supported in part by a grant from the Ministry of Education, Culture, Sports, Science and Technology of Japan and by a grant from the Ministry of Health, Labour and Welfare of Japan. We thank Chikako Sakai, Hitoshi Moriuchi and Noboru Hosogai for their excellent technical assistance. We are also grateful to the support, cooperation and trust of the patients and their families.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arai, T., Zhao, M., Kanegane, H. et al. Genetic analysis of contiguous X-chromosome deletion syndrome encompassing the BTK and TIMM8A genes. J Hum Genet 56, 577–582 (2011). https://doi.org/10.1038/jhg.2011.61
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2011.61
Keywords
This article is cited by
-
Familial 5.29 Mb deletion in chromosome Xq22.1–q22.3 with a normal phenotype: a rare pedigree and literature review
BMC Medical Genomics (2023)
-
Identification and analysis of deletion breakpoints in four Mohr-Tranebjærg syndrome (MTS) patients
Scientific Reports (2022)
-
Phenotype prediction of Mohr-Tranebjaerg syndrome (MTS) by genetic analysis and initial auditory neuropathy
BMC Medical Genetics (2019)
-
Exome sequencing in multiplex autism families suggests a major role for heterozygous truncating mutations
Molecular Psychiatry (2014)
-
Chronic granulomatous disease, the McLeod phenotype and the contiguous gene deletion syndrome-a review
Clinical and Molecular Allergy (2011)
