
Abstract
The epidermal growth factor (EGF) gene encodes a growth factor that binds to the EGF receptor (EGFR), which is involved in activating pathways that promote cellular proliferation, survival, migration and differentiation, and lack of control is characteristic of malignant development. Previous studies showed that serum EGF levels may influence the risk of cancer. In this study, we genotyped the EGF G61A polymorphism (rs4444903) and measured serum EGF levels using an enzyme immunoassay in a hospital-based case–control study of 345 patients with diagnosed renal cell carcinoma (RCC) and 346 cancer-free controls in a Chinese population. Compared with the EGF 61GG genotype, the AA genotype had a significantly increased RCC risk (odds ratio=1.80, 95% confidence interval=1.04–3.12). Besides, the mean serum EGF levels in RCC patients (858.94±391.54 pg ml–1) were significantly lower than those in controls (1281.52±568.42 pg ml–1, P<0.001). In addition, individuals carrying AA genotype had lower serum EGF levels than GA or GG carriers. These results suggested that the EGF G61A polymorphism is involved in the etiology of RCC and thus may be a marker for genetic susceptibility to RCC in Chinese populations. Larger studies are warranted to validate our findings.
Similar content being viewed by others

Introduction
Renal cell carcinoma (RCC) represents 2–3% of all cancers and is the third leading cause of death among genitourinary malignancies, with the highest incidence occurring in the developed countries.1 It is estimated that ∼37.7 men and 16.6 women per 100 000 Chinese individuals are diagnosed with RCC every year.2 Accumulative epidemiological studies have suggested that gender, obesity, cigarette smoking and a history of hypertension, along with some other less certain factors such as alcohol consumption, occupational exposures, diet, physical activity and family history of cancer are associated with RCC.3, 4 Cigarette smoking, for example, doubles the risk for RCC and contributes to as much as one-third of all cases, yet only a fraction of smokers and a low number of nonsmokers develop RCC.5 This suggests that interindividual differences including genetic susceptibility in critical genes may have an important role in RCC carcinogenesis.
Epidermal growth factor (EGF) is a member of the EGF superfamily, which also includes transforming growth factor-α, heparin-binding EGF-like growth factor, epiregulin, betacellulin and amphiregulin.6 EGF is encoded by a 4.8-kb mRNA transcript from a gene that is 110 kb in length, contains 24 exons and is located on chromosome 4q25–27.6 As a growth factor, EGF can activate DNA synthesis and cellular proliferation and stimulate mitogenesis in epidermal tissue.7, 8 In 2002, Shahbazi et al.9 first identified a G>A substitution at position 61 in the 5′-untranslated region of EGF, and the presence of the variant 61A allele led to a decreased EGF production in peripheral blood mononuclear cells. Since then, numerous studies focused on the association between the EGF G61A polymorphism and risk of cancers, including melanoma,10, 11 gastric cancer,12, 13 breast cancer14 and others.
As EGF is important for tumor growth and progression, the dysregulation of EGF gene may modulate the progression and spread of cancer. To the best of our knowledge, no reports have been published regarding the role of the EGF G61A polymorphism in RCC. Therefore, our present study was designed to investigate the association of EGF G61A gene polymorphism with risk of RCC in our ongoing hospital-based case–control study in a Chinese population. Besides, to further assess the potential functional effect of EGF G61A in RCC risk, we investigated the association of serum EGF levels with RCC risk.
Materials and methods
Study subjects
This case–control study consisted 345 RCC cases and 346 cancer-free controls. All subjects were genetically unrelated ethnic Han Chinese. Cases were patients with histopathologically confirmed incident RCC, recruited in an ongoing study starting in July 2006 at The First Affiliated Hospital of Nanjing Medical University, Nanjing, China. The cancer-free control subjects were genetically unrelated to the cases and had no individual history of cancer. The controls were recruited from healthy subjects who were seeking health care in the outpatient departments at the hospital. All controls of appropriate age and sex for frequency matching with the cases were recruited and included if they gave their informed consent. As for the cases, exclusion criteria for the controls were significant mental impairment or blood transfusion in the past months; controls were also excluded if they had symptoms suggestive of RCC, such as hematuria. Before recruitment, a standard questionnaire was administered by trained interviewers to obtain information on demographic data and related factors through face-to-face interviews. After the interview, about 5 ml venous blood sample was collected from each subject. The study was approved by the institutional review board of Nanjing Medical University.
Genotyping
Genomic DNA was isolated from leukocytes of venous blood by proteinase K digestion and phenol/chloroform extraction. The EGF G61A polymorphism was determined using the PCR–restriction fragment length polymorphism method, as previously described.9 The PCR primers for the EGF G61A polymorphism were 5′-TGTCACTAAAGGAAAGGAGGT-3′ (forward) and 5′-TTCACAGAGTTTAACAGCCC-3′ (reverse). PCR was performed in a total volume of 20 μl containing 50 ng genomic DNA, 10 × Taq buffer, 0.02 mmol l–1 of MgCl2, 0.05 mmol l–1 of dNTP mix, 10 pmol μl–1 of each primer and 1 U Taq DNA polymerase. After initial denaturation at 95 °C for 5 min, the reaction was carried out at 95 °C denaturation for 30 s, annealing for 40 s at 55 °C and extension for 45 s at 72 °C for a total of 34 cycles, and a final elongation at 72 °C for 10 min. The 242 bp amplified products were incubated with 3 U of AluI (New England Biolabs(Beijing) Ltd., Beijing, China) restriction enzyme at 37 °C overnight. The restriction fragments were then analyzed by electrophoresis in 3% agarose gel stained with 0.5% ethidium bromide and photographed under UV illumination. AluI digested the 242 bp PCR products containing the 61G allele into 193, 34 and 15 bp fragments, whereas the 61A allele produced 102, 91, 34 and 15 bp fragments. The polymorphism analysis was carried out by two persons independently in a blinded manner. More than 15% of the samples were randomly selected for confirmation, and the results were 100% concordant.
EGF serum levels quantitative measurement
Serum samples were available for 70 RCC cases and 96 controls. EGF levels were measured in serum as opposed to plasma because the major source of EGF in the blood is platelets.15 The serum was allowed to clot for 30 min at 4 °C before centrifugation at 2000 r.p.m. for 10 min at 4 °C. Serum was isolated and stored at −80 °C before use. We detected EGF concentration by using a sandwich enzyme immunoassay (Quantikine EGF immunoassay kit, R&D Systems Inc, Minneapolis, MN, USA). The EGF concentration was calculated by referring to a standard curve according to the manufacturer’s instructions.
Statistical analyses
Differences in the distributions of demographic characteristics, selected variables, and frequencies of genotypes of EGF G61A variants between the cases and controls were evaluated using the Student’s t-test (for continuous variables) or χ2-test (for categorical variables). Hardy–Weinberg equilibrium was tested using a goodness-of-fit χ2-test. The associations between EGF genotypes and risk of RCC were estimated by computing odds ratios (ORs) and their 95% confidence intervals (CIs) from unconditional logistic regression analysis with the adjustment for possible confounders. P<0.05 was considered statistically significant, and all statistical tests were two sided. All the statistical analyses were performed with Statistical Analysis System software (9.1.3; SAS Institute, Cary, NC, USA).
Results
Characteristics of the study population
The frequency distributions of selected characteristics of the cases and controls are presented in Table 1. There were no differences between the cases and controls on age, sex, body mass index, smoking and drinking status (all P>0.05). However, there were more subjects with hypertension (38.0%) and diabetes (12.8%) among the cases than among the controls (29.8 and 4.6%, respectively), and these differences were statistically significant (P=0.023 for hypertension and P<0.001 for diabetes). The majority of patients (85.5%) had the conventional clear cell carcinoma. Papillary carcinoma was presented in 9 (2.6%) patients and 21 (6.1%) had chromophobe carcinoma. In addition, there were 20 (5.8%) unclassified RCC patients. Approximately 69% of patients were in stage I, whereas 15.1, 4.9 and 10.7% of patients were found to have stage II, III and IV diseases, respectively. The nuclear grades from I to IV were 17.7, 50.4, 23.8 and 8.1% respectively.
EGF genotype and RCC risk
The genotype and allele distributions of the EGF G61A polymorphism in the cases and controls were shown in Table 2. The observed genotype frequencies for this polymorphism were in Hardy–Weinberg equilibrium in the controls (χ2=0.0026, P=0.96). For the EGF G61A polymorphism, the frequencies of the GG, GA and AA genotypes were 46.7, 40.0 and 13.3%, respectively, among the cases, and 52.9, 39.6 and 7.5%, respectively, among the controls (P=0.031). After adjusting for possible confounders (age, sex, pack-years of smoking, drinking status, hypertension and diabetes), subjects carrying GA heterozygote and AA homozygote had an increased risk of RCC (OR=1.14, 95% CI=0.82–1.58 for GA versus GG, and OR=1.80, 95% CI=1.04–3.12 for AA versus GG) (Ptrend=0.026), compared with GG homozygote. In addition, subjects carrying AA homozygote had a 1.82-fold increased risk (95% CI=1.09–3.06) than those carrying GG/GA genotypes (P=0.012), and the A allele displayed a high prevalence of RCC compared with the G allele (P=0.016). These data indicated that individuals carrying variant A allele may have a higher risk for developing RCC.
In this study, we further evaluated the effect of EGF G61A variant on RCC risk stratified by age, body mass index, sex, smoking status, pack-years of smoking and drinking status. As shown in Table 3, we found that the increased risk was more pronounced among older patients (OR=2.54, 95% CI=1.23–5.23) and never alcohol drinkers (OR=2.03, 95% CI=1.07–3.85).
EGF serum levels and RCC risk
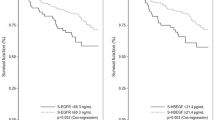
Serum samples were available for 70 RCC cases and 96 controls in this case–control study. The mean serum EGF level was 858.94 pg ml–1 (±391.54) in cases and 1281.52 pg ml–1 (±568.42) in controls (P<0.001) (Figure 1), suggesting that serum EGF level may serve as an independent protective marker against RCC.

Distribution of serum EGF levels in 70 cases and 96 controls. Mean levels of serum EGF were significantly different between cases and controls (*P<0.001).
Then, the associations between serum EGF levels and risk of RCC were further evaluated by unconditional logistic regression analyses. As shown in Table 4, when the median EGF level in controls (1281.15 pg ml–1) was used as the cutoff value for calculating the ORs, 14.3% (10 of 70) of the cases were above this median level. The serum EGF levels above this median level was associated with a dramatic decreased risk of RCC after adjustment for age, sex, pack-years of smoking, drinking status, hypertension and diabetes (OR=0.12, 95% CI=0.05–0.29). In addition, when the control quartiles of EGF levels were used to categorize the variable, a significant dose–response relationship between increased serum EGF levels and declined RCC risk was evident (ORs=0.57, 0.17 and 0.13 for the second, third and fourth quartiles, respectively) (Table 4). Furthermore, serum EGF levels in subjects carrying AA (714.64 pg ml–1) genotype was lower than those with GA (855.97 pg ml–1) or GG (893.14 pg ml–1) genotypes, but the results were not statistically significant (AA versus GA, P=0.233; AA versus GG, P=0.295).
Discussion
EGF, a potent mitogenic peptide, is a growth factor that activates a signaling transduction cascade responsible for activating genes involved in cell proliferation, differentiation or survival through binding to its receptor (EGFR),16 having an important role in carcinogenesis.17 Therefore, genetic variant in the EGF gene was hypothesized to have a critical role in tumorigenesis. In this study, we analyzed the association between a functional G61A polymorphism of EGF and the risk for developing RCC in a Chinese population. We found that the variant 61AA genotype was associated with an increased risk of RCC, compared with their GG/GA genotypes, and this increased risk was more pronounced among the older people and never drinkers.
Previous studies showed that low-serum EGF level may increase the risk of endometrium carcinoma18 and breast cancer.14 In this study, we found that there was a significantly lower serum EGF levels in RCC cases than that in controls, and individuals carrying AA homozygote had a lower serum EGF level than the GA or GG carriers. EGF is a growth factor that activates a signal transduction pathway promoting proliferation, migration and differentiation; nevertheless, some investigators showed that, after EGF binding to its receptor, they are both internalized, sourcing the formation of endosomes and ultimately degradation.19, 20 The protective effect for the EGF overexpression in G allele carriers that we observed in this study may be explained by the increased bioavailability of EGF and the subsequent removal of EGFR from the cell surface due to its degradation. In fact, other studies showed that EGFR expression on cell surface decreases abruptly when a certain concentration of EGF is added to cell lines.21, 22 Specific EGF ligands promote a long-lasting effect, inhibiting EGFR recycling.22 A low availability of EGFR will decrease the EGF/EGFR pathway activation and eventually protect RCC development. Another recent study reported that, in some cell lines, EGF paradoxically inhibits proliferation in high concentrations and induces loss of adhesion, cell-cycle arrest and apoptosis.23
In 2002, Shahbazi et al.9 first reported that EGF 61GG genotype was significantly associated with risk of malignant melanoma compared with the AA genotype (OR=4.90, 95% CI=2.30–10.20), which may appear contradictory to our present results. The discrepancy could be interpreted to suggest that different mechanisms underlie the development of malignant melanoma and RCC, and EGF gene may have different role in different tumorigenesis. It has been suggested that EGF has pleiotropic cell responses that are regulated by signals when numerous negative regulatory mechanisms act, such as availability of the ligand to the receptor and terminal signal inactivation through receptor internalization and degradation.19, 20 Moreover, this regulation varies according to the arrangements of ligand–receptor engagement, tyrosine phosphorylation and subsequent receptor dimerization combinations; as well as, depending on the stage and context of cell type and cell growth, different signaling transduction pathways can be activated.20 As active pathways are not known in different tumors, we can explain that our contradictory results for different regulatory mechanisms of EGF may depend on specific tissue or tumor type.
We also analyzed the distribution of EGF genotypes among the East Asian population and Caucasian population from the previous studies, and found that, the EGF genotypes were significantly different between the East Asian population and Caucasian population. In this study, the EGF 61A allele frequency (0.273) in control was close to that reported in the Chinese (0.297, 0.305),14, 24 Korean (0.284)25 and Japanese populations (0.313, 0.304),12, 13 but was significantly lower than that in the Caucasians (higher than 0.500).10, 11, 26, 27 Therefore, we confirmed that EGF genotypes were significantly different between the East Asian and Caucasian populations. The ethnic heterogeneity in this polymorphism suggests the possibility that constitutive EGF expression may vary between different ethnic groups. Moreover, this ethnic heterogeneity results in discrepancy between risk association case–control studies with different ethnic groups.
Our present study has some limitations. First, our sample size was small, and we did not have detailed information on environmental factors, such as occupational exposures, diet and physical activity; these may limit the statistical power of our study, especially for gene–environment interaction analyses. Second, our study was a hospital-based study design, because we could not rule out the possibility of selection bias of subjects who may have been associated with a particular genotype. However, the agreement with Hardy–Weinberg equilibrium and similar allele frequency of our controls to those reported in the East Asian populations suggested that the selection bias in terms of genotype distribution would not be substantial.
In conclusion, our study showed that the EGF G61A polymorphism was associated with RCC risk. We found that the variant AA genotype was associated with an increased risk of RCC, compared with their wild-type GG homozygote. We also observed that lower serum EGF levels were associated with an increased RCC risk. To explore the exact biological mechanism of EGF genotype and their interaction with environmental factors, further functional studies and larger well-designed prospective studies are warranted.
References
Jemal, A., Siegel, R., Ward, E., Hao, Y., Xu, J. & Thun, M. J. Cancer statistics, 2009. CA Cancer J. Clin. 59, 225–249 (2009).
Yang, L., Parkin, D. M., Ferlay, J., Li, L. & Chen, Y. Estimates of cancer incidence in China for 2000 and projections for 2005. Cancer Epidemiol. Biomarkers Prev. 14, 243–250 (2005).
Lipworth, L., Tarone, R. E. & McLaughlin, J. K. The epidemiology of renal cell carcinoma. J. Urol. 176, 2353–2358 (2006).
Setiawan, V. W., Stram, D. O., Nomura, A. M., Kolonel, L. N. & Henderson, B. E. Risk factors for renal cell cancer: the multiethnic cohort. Am. J. Epidemiol. 166, 932–940 (2007).
Hunt, J. D., van der Hel, O. L., McMillan, G. P., Boffetta, P. & Brennan, P. Renal cell carcinoma in relation to cigarette smoking: meta-analysis of 24 studies. Int. J. Cancer 114, 101–108 (2005).
Normanno, N., De Luca, A., Bianco, C., Strizzi, L., Mancino, M., Maiello, M. R. et al. Epidermal growth factor receptor (EGFR) signaling in cancer. Gene 366, 2–16 (2006).
Laurence, D. J. & Gusterson, B. A. The epidermal growth factor. A review of structural and functional relationships in the normal organism and in cancer cells. Tumour Biol. 11, 229–261 (1990).
Carpenter, G. & Cohen, S. Epidermal growth factor. J. Biol. Chem. 265, 7709–7712 (1990).
Shahbazi, M., Pravica, V., Nasreen, N., Fakhoury, H., Fryer, A. A., Strange, R. C. et al. Association between functional polymorphism in EGF gene and malignant melanoma. Lancet 359, 397–401 (2002).
Amend, K. L., Elder, J. T., Tomsho, L. P., Bonner, J. D., Johnson, T. M., Schwartz, J. et al. EGF gene polymorphism and the risk of incident primary melanoma. Cancer Res. 64, 2668–2672 (2004).
McCarron, S. L., Bateman, A. C., Theaker, J. M. & Howell, W. M. EGF +61 gene polymorphism and susceptibility to and prognostic markers in cutaneous malignant melanoma. Int. J. Cancer 107, 673–675 (2003).
Goto, Y., Ando, T., Goto, H. & Hamajima, N. No association between EGF gene polymorphism and gastric cancer. Cancer Epidemiol. Biomarkers Prev. 14, 2454–2456 (2005).
Hamai, Y., Matsumura, S., Matsusaki, K., Kitadai, Y., Yoshida, K., Yamaguchi, Y. et al. A single nucleotide polymorphism in the 5′ untranslated region of the EGF gene is associated with occurrence and malignant progression of gastric cancer. Pathobiology 72, 133–138 (2005).
Wang, Y., Tian, T., Hu, Z., Tang, J., Wang, S., Wang, X. et al. EGF promoter SNPs, plasma EGF levels and risk of breast cancer in Chinese women. Breast Cancer Res. Treat. 111, 321–327 (2008).
Lanuti, M., Liu, G., Goodwin, J. M., Zhai, R., Fuchs, B. C., Asomaning, K. et al. A functional epidermal growth factor (EGF) polymorphism, EGF serum levels, and esophageal adenocarcinoma risk and outcome. Clin. Cancer Res. 14, 3216–3222 (2008).
Olayioye, M. A., Neve, R. M., Lane, H. A. & Hynes, N. E. The ErbB signaling network: receptor heterodimerization in development and cancer. EMBO J. 19, 3159–3167 (2000).
Normanno, N., Bianco, C., Strizzi, L., Mancino, M., Maiello, M. R., De Luca, A. et al. The ErbB receptors and their ligands in cancer: an overview. Curr. Drug Targets 6, 243–257 (2005).
Tomaszewski, J., Miturski, R. & Kotarski, J. [Concentration of epidermal growth factor (EGF) in serum of women with endometrial cancer]. Ginekol. Pol. 67, 248–253 (1996).
Wells, A. EGF receptor. Int. J. Biochem. Cell Biol. 31, 637–643 (1999).
Singh, A. B. & Harris, R. C. Autocrine, paracrine and juxtacrine signaling by EGFR ligands. Cell Signal 17, 1183–1193 (2005).
Salazar, G. & Gonzalez, A. Novel mechanism for regulation of epidermal growth factor receptor endocytosis revealed by protein kinase A inhibition. Mol. Biol. Cell 13, 1677–1693 (2002).
Friedman, L. M., Rinon, A., Schechter, B., Lyass, L., Lavi, S., Bacus, S. S. et al. Synergistic down-regulation of receptor tyrosine kinases by combinations of mAbs: implications for cancer immunotherapy. Proc. Natl Acad. Sci. USA 102, 1915–1920 (2005).
Zhao, X., Dai, W., Zhu, H., Zhang, Y., Cao, L., Ye, Q. et al. Epidermal growth factor (EGF) induces apoptosis in a transfected cell line expressing EGF receptor on its membrane. Cell Biol. Int. 30, 653–658 (2006).
Jin, G., Miao, R., Deng, Y., Hu, Z., Zhou, Y., Tan, Y. et al. Variant genotypes and haplotypes of the epidermal growth factor gene promoter are associated with a decreased risk of gastric cancer in a high-risk Chinese population. Cancer Sci. 98, 864–868 (2007).
Kang, S., Kim, J. W., Park, N. H., Song, Y. S., Park, S. Y. Kang, S. B. et al. Epidermal growth factor 61 A/G polymorphism and uterine cervical cancer. Int. J. Gynecol. Cancer 17, 492–496 (2007).
Randerson-Moor, J. A., Gaut, R., Turner, F., Whitaker, L., Barrett, J. H., Silva Idos, S. et al. The relationship between the epidermal growth factor (EGF) 5′UTR variant A61G and melanoma/nevus susceptibility. J. Invest. Dermatol. 123, 755–759 (2004).
James, M. R., Hayward, N. K., Dumenil, T., Montgomery, G. W., Martin, N. G. & Duffy, D. L. Epidermal growth factor gene (EGF) polymorphism and risk of melanocytic neoplasia. J. Invest. Dermatol. 123, 760–762 (2004).
Acknowledgements
This study was supported by the Foundation of Medical Key Department of Jiangsu Province–Department of Urology of Jiangsu Province Hospital (BK2008473).
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Zhu, J., Meng, X., Yan, F. et al. A functional epidermal growth factor (EGF) polymorphism, EGF serum levels and renal cell carcinoma risk in a Chinese population. J Hum Genet 55, 236–240 (2010). https://doi.org/10.1038/jhg.2010.12
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2010.12
Keywords
This article is cited by
-
Decreased macrophage inflammatory protein (MIP)‐1α and MIP‐1β increase the risk of developing nasopharyngeal carcinoma
Cancer Communications (2018)
-
A functional EGF+61 polymorphism is associated with severity of obstructive sleep apnea
Sleep and Breathing (2015)
-
Functional single-nucleotide polymorphism of epidermal growth factor is associated with the development of Barrett's esophagus and esophageal adenocarcinoma
Journal of Human Genetics (2012)
