
Abstract
The β2-adrenergic receptor (β2AR) is a transmembrane protein expressed by airway smooth muscle cells. In vitro studies have shown that polymorphisms at amino acid positions 16 and 27 alter receptor function. The aim of this study was to examine the associations between the β 2AR polymorphisms and risks of asthma, chronic obstructive pulmonary disease (COPD) and respiratory symptoms in a sample of adults. Participants were part of a cross-sectional population-based study of risk factors for respiratory disease. A total of 1,090 Caucasian participants completed a detailed respiratory questionnaire, spirometry, methacholine challenge and measurement of gas transfer. Genotyping for β 2AR polymorphisms at positions 16 and 27 was performed using the tetra-primer amplification refractory mutation system–polymerase chain reaction (ARMS–PCR) method. Haplotype frequencies for the two polymorphisms were estimated using the E-M algorithm. We found the Arg16 homozygotes had an increased risk of COPD (OR 5.13; 95% CI 1.40,18.8), asthma (2.44; 1.12,5.31) and symptoms of wheeze (1.84; 1.02,3.35). The Gln27 homozygotes had an increased risk of asthma (2.08; 1.05,4.13) and bronchial hyperreactivity (BHR) (1.92; 1.07,3.46). The Arg16/Gln27 haplotype was associated with asthma (1.63; 1.12,2.38) and COPD (2.91; 1.42,5.94). The Arg16/Gln27 β2AR haplotype is important in COPD, asthma and BHR, and may be associated with more severe respiratory symptoms in middle-aged and older adults.
Similar content being viewed by others

Introduction
Beta2 (β2)-agonists are one of the most important classes of drugs used in the treatment of asthma and chronic obstructive pulmonary disease (COPD). Their action is mediated by the β2-adrenergic receptor (β2AR), a transmembrane protein expressed by airway smooth muscle cells. When stimulated, β2AR results in cAMP-mediated muscular relaxation that is important to the regulation of airway tone, and therefore airway reactivity and lung function (Turner et al. 2004).
Several polymorphisms within β 2AR have been described (Reihsaus et al. 1993). In particular, the amino acid substitutions at positions 16, arginine → glycine (Arg → Gly) and 27, glutamine → glutamate (Glu → Gln) have been shown to alter the receptor function in vitro (Green et al. 1994, 1995). Initial in vivo studies of transfected cell lines and primary cultures of human-airway smooth muscle cells found the Gly16 form of the receptor becomes more down-regulated and desensitised after exposure to β2-agonist than the Arg16 form (Green et al. 1994, 1995). However, more recent in vivo work in humans has shown the Arg16Gln27 haplotype is the form of the receptor that is associated with agonist-promoted desensitization (Dishy et al. 2001). Genetic studies of these polymorphisms have found them to be associated with asthma severity (Turki et al. 1995; Weir et al. 1998), bronchial hyperreactivity (BHR) (Hall et al. 1995; Ramsay et al. 1999), bronchodilator (BD) response (D’Amato et al. 1998; Lima et al. 1999; Martinez et al. 1997; Ulbrecht et al. 2000) and lung function (Summerhill et al. 2000).
Few studies have investigated β 2AR polymorphisms in COPD and related phenotypes. One study in Chinese patients found a decreased prevalence of the Arg16 allele in the COPD cases, and subjects with the Gln27 allele had lower FEV1 percent predicted (Ho et al. 2001). In contrast a study of Egyptian COPD patients found a decreased prevalence of the Gln27 allele in the COPD patients compared to controls (Hegab et al. 2004). Furthermore, the Lung Health Study (LHS) of current smokers found a protective effect of heterozygosity at position 27 against rapid decline in lung function (Joos et al. 2003).
Most genetic studies have investigated these polymorphisms in isolation. However, work by Drysdale et al. (2000) has shown that the haplotype containing Arg16/Gln27 was associated with a reduced response to β2-agonist in vivo (Drysdale et al. 2000), highlighting the importance of examining haplotypes. A few studies have investigated β 2AR haplotypes and risk of asthma, COPD or related phenotypes with conflicting results. Two studies have found that the Gly16/Gln27 haplotype was protective against BHR (Litonjua et al. 2004; Ulbrecht et al. 2000). Conversely, an Italian study found the Gly16/Gln27 haplotype to be associated with an increased risk of BHR (D’Amato et al. 1998). Furthermore, the LHS found no association between any β 2AR haplotypes and bronchodilator response or non-specific BHR, or rate of decline in lung function (Joos et al. 2003). BHR is a known risk factor for chronic respiratory symptoms (Xu et al. 1997) and mortality from COPD (Hospers et al. 2000), so given these conflicting results it is clear that further study of the β 2AR gene in asthma, COPD and related phenotypes is warranted.
We recruited 1,232 randomly selected middle-aged and older adults from the general community in Melbourne, Australia. We examined their lung function and bronchial responsiveness, and genotyped them for the β 2AR16 and β 2AR27 polymorphisms. The aim of this study was to further examine the associations between the β 2AR polymorphisms and haplotypes, and risk of asthma, COPD and related phenotypes.
Methods
Participants
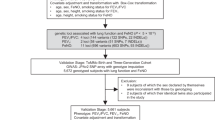
Recruitment and pulmonary-function testing were described in detail elsewhere (Matheson et al. 2005). Briefly, 1,232 subjects (595 females, 637 males) were randomly recruited to be part of a two-stage cross-sectional epidemiological study to investigate risk factors for asthma and COPD in adults aged between 45 and 69 years. From this general Caucasian population, sample cases of respiratory conditions and controls were selected (described in more detail below). The study was approved by the Ethics Committees at Monash University and The Alfred Hospital, Melbourne, Australia. All participants gave written informed consent.
Lung function testing
Spirometry and diffusing capacity (DLco) was performed according to the American Thoracic Society (ATS) criteria. Predicted values for FEV1, FVC and FEF25–75 were calculated from age, height and gender using equations by Gore et al. (1995), and for DLco using the equations by Quanjer et al. (1983). Methacholine (MCh) (USP Methapharm Inc., Brantford, ON, Canada) was delivered by a Mefar 3B dosimeter (Mefar, Bovezzi, Italy) until FEV1fell by 20% from the initial value or up to a cumulative dose of 2 mg (PD20). BHR was defined as a PD20 FEV1 < 2 mg MCh (Toelle et al. 1992). Reasons which caused subjects not to complete the MCh challenge included poor-quality spirometry (n=5), being on medication for heart disease including beta-blockers, epilepsy (n=92) or an initial FEV1 less than 70% predicted or 1.5 l (n=46). For those subjects with an initial FEV1 less than 70% predicted or 1.5 l, spirometry was repeated 10 min after the administration of a bronchodilator [200 μg (2 puffs) of salbutamol via a spacer]. Significant bronchodilator reversibility was defined as an increase in FEV1 of at least 12% and 200 mL (Pellegrino et al. 2005).
Definitions
Wheeze was defined as a positive response to: “Have you had wheezing or whistling in your chest at any time in the last 12 months?”. Nocturnal chest tightness was defined as a positive response to: “Have you been woken by chest tightness at any time in the last 12 months?”. Dyspnoea was defined as a positive response to: “Are you troubled by shortness of breath when hurrying on level ground or walking up a slight hill?”. Current asthma was defined as wheeze during the last 12 months, together with BHR to methacholine (Toelle et al. 1992) or significant bronchodilator reversibility (where BHR could not be done). Mild airflow obstruction was defined as FEV1/FVC ratio less than 70% (Pauwels et al. 2001). Chronic obstructive bronchitis was defined as a positive response to: “Have you brought up phlegm on most days for as much as 3 months of a year for at least 2 successive years?” and mild airflow obstruction. Symptomatic emphysema was defined as mild airflow obstruction, a DLco < 80% predicted and dyspnoea. COPD was defined as either chronic obstructive bronchitis or symptomatic emphysema. Pack years were calculated as the average number of cigarettes smoked per day divided by 20 and multiplied by the number of years smoked.
Genotyping
From the 1,232 participants in the study, blood and consent to extract DNA were available for 1,138 participants (92.4%). DNA was successfully extracted from 1,102 subjects (96.8%) using standard phenol chloroform techniques. All analyses were performed blind with respect to diagnosis and patient characteristics. β 2AR genotype was determined using the tetra-primer ARMS–PCR method described by Ye et al. (2001). Primers were designed using the computer program created by the authors of the method. Approximately 50 ng of DNA was amplified in a 20-μl reaction mix. This mix contained 1 × reaction buffer, 2.5 mM MgCl2, 250 μM of dNTP (GeneAmp, Applied Biosystems, CA, USA), one unit of AmpliTaq Gold DNA polymerase (Applied Biosystems) and 0.5 μM of each primer. The outer primers were diluted to 1:10 of the concentration of the inner primers to enhance specificity. The PCR cycling conditions for the β 2AR16 polymorphism were 95°C for 10 min, followed by 35 cycles of 94°C for 1 min, 67°C for 1 min and 72°C for 1 min, and then a final extension for 10 min at 72°C. For β 2AR27 the conditions were identical, with the exception of an annealing temperature of 85°C. The PCR products were resolved by electrophoresis on a 3% agarose gel stained with ethidium bromide. A random sample of 10% of the total sample was genotyped using the restriction fragment length polymorphism (RFLP) method described by Martinez et al. (1997) to validate the genotyping protocol.
Statistical analysis
The statistical analysis was performed using the statistical package STATA (version 6; STATA Corporation, TX, USA). The haplotype analysis was performed using the haplo.stats package for R (Version 2.0.0; The R Foundation for Statistical Computing). These procedures assume Hardy–Weinberg equilibrium (HWE). HWE was calculated by a χ2 goodness of fit test.
Multiple regression analysis was used to examine the association between genotype and continuous outcomes. For binary outcomes logistic regression was used, and cases were subjects that reported the symptom or met the criteria for the disease of interest. Controls were subjects who did not report any symptoms and did not have any of the outcomes investigated. The same control group was used for all analyses. Covariates included in the models were age, gender, smoking status (current, past or never smoker), and pack years. Modification of the effect of genotype by smoking was assessed by including an interaction term (genotype*ever smoking) in the models. All subjects in the analysis presented were of Caucasian descent.
Haplotype frequencies were estimated using the E-M algorithm for genetic markers measured on unrelated subjects with unknown phase. The β 2AR16 and β 2AR27 SNPs were used in the haplotype analysis. Those traits significant in the genotype analysis, for either single nucleotide polymorphism (SNP), were further explored using haplotype analysis using haplo.score. The haplo.glm function was used to compute the regression of a trait on haplotypes, and to adjust for covariates (Hawley and Kidd 1995). For binary traits, this procedure fitted logistic regression models which provided odds ratios (ORs) and 95% confidence intervals (95% CIs). For continuous traits, linear regression models were fitted giving differences of means between groups and 95% CIs. For all analyses the significance level was set at P<0.05.
Results
Subject characteristics
The clinical characteristics of the subgroups are presented in Table 1. The control group was significantly younger than all other clinical subgroups. There was a significantly greater proportion of males in the control group than in the groups with asthma, BHR, dyspnoea or nocturnal chest tightness. The prevalence of current and past smokers was significantly greater in all the clinical subgroups compared to the controls. Wheeze was the most frequently reported symptom, followed by dyspnoea when walking on level ground or up a slight hill (dyspnoea grade 2), and then nocturnal chest tightness (Table 1). Subjects with COPD had the worst lung-function parameters, but all clinical subgroups had worse lung function than the controls.
Genotype and haplotype frequencies
Genotyping was successfully completed for 1,090 subjects (98.9% of available samples) for the β2AR16 and β2AR27 polymorphisms. For β 2AR16, the prevalence of the Arg16 homozygotes was 13.1% (n=143), for Arg16/Gly16 heterozygotes 46.2% (n=504) and for Gly16 homozygotes 40.6% (n=443). For β 2AR27, the prevalence of the Gln27 homozygotes was 32.0% (n=349), for Gln27/Glu27 heterozygotes 47.6% (n=519) and for Glu27 homozygotes 20.4% (n=222). In the controls, both polymorphisms were in HWE (β2AR16 P=0.45; β2AR27 P=0.85). There was strong linkage disequilibrium between the two polymorphisms According to D´ measures, there appeared to be strong LD between the two SNPs (D´ 0.996; 95% CI 0.97, 1.0 P<0.0001); however, r2 measures (0.447) suggest that LD is more moderate. The haplotype frequencies were estimated using the E-M algorithm. As found by other investigators, the Arg16 segregated more commonly with Gln27 and Gly16 with Glu27. The Gly16/Glu27 haplotype (0.44) was the most common, with Arg16/Gln27 (0.36) the next most frequent, Gly16/Gln27 at 0.197 and the Arg16/Glu27 haplotype very rare in our population (0.00057).
Respiratory symptoms, current asthma and single β2AR polymorphisms
The associations between individual polymorphisms and risk of current asthma and respiratory symptoms are reported in Tables 2 and 3. A significantly increased risk of wheeze, asthma and COPD was found for individuals with the Arg16/Arg16 genotype.
For the β2AR27 polymorphism we found a higher prevalence of BHR and asthma. There was also a marginally increased risk of the respiratory symptoms of nocturnal chest tightness and dyspnoea in individuals homozygous for the Gln27 genotype. Also a marginally lower FEF25–75 % predicted in individuals homozygous for the Gln27 genotype was found (regression coefficient −5.54; 95% CI −11.6, 0.48, P=0.07). There was no evidence of an interaction between either polymorphism and ever smoking for any of the outcomes investigated.
Haplotype analysis
In order to investigate the combined effect of the two SNPs, haplotype analysis was also performed. The results of the haplotype analyses are presented in Table 4. The Arg16/Gln27 haplotype was associated with an increased risk of asthma and COPD. A marginal association between the Arg16/Gln27 haplotype and symptoms of wheeze, and dyspnoea, and BHR was found. The Arg16/Gln27 haplotype was also associated with a lower FEF25–75 % predicted, but this did not quite reach statistical significance (regression coefficient −2.95; 95% CI −6.12, 0.22, P=0.07).
Discussion
The Arg16/Gln27 haplotype was associated with current asthma, BHR and COPD in this sample of middle-aged and older adults. Our study is one of the largest of older adults from the general population, and one of the first to investigate β2AR haplotypes in this age group.
For the SNPs individually, the association with asthma was strongest in the Arg16/Gly16 heterozygotes. Our results are consistent with a Chinese study that reported an association between the Arg16 allele and asthma in cigarette smokers (Wang et al. 2001). However, a study of childhood asthma found an association with the Glu27 allele (Hopes et al. 1998), and another study found nocturnal asthma to be associated with the Gly16 allele (Turki et al. 1995). Furthermore, many other studies have reported no association with asthma at all (Dewar et al. 1998; Martinez et al. 1997; Ramsay et al. 1999; Reihsaus et al. 1993; Summerhill et al. 2000; Turner et al. 2004). Only one study has looked at β2AR haplotypes and risk of asthma, which found the Gly16/Gln27 haplotype was more prevalent in moderate asthmatics than in mild asthmatics (Weir et al. 1998). This is different to our reported association with Arg16/Gln27, which may be because our subjects had milder asthma. Unlike Weir et al. (1998), we were able to resolve β2AR haplotypes for subjects heterozygous at both polymorphisms, because we used the E-M algorithm to infer phase in all subjects.
An increased risk of COPD was associated with Arg16 homozygous genotype, and COPD and FEF25–75 were associated with possession of the Arg16/Gln27 haplotype. The measurement of FEF25–75 is a feature of small airways disease, which has been shown to progress to COPD (Hogg 2004). These results are in contrast to two previous studies, one from Taiwan that found the Arg16 allele to be less prevalent in COPD cases (Ho et al. 2001) and the other from Egypt that found the Gln27 allele to be less prevalent in COPD cases (Hegab et al. 2004). The LHS found a protective effect of the Glu27/Gln27 genotype on rapid decline in lung function, but no association with any of the β2AR haplotypes (Joos et al. 2003). Further studies of β2AR haplotypes in COPD are needed to confirm our association in other populations.
We found a significant association between respiratory symptoms of wheeze and dyspnoea with the Arg16 genotype and the Arg16/Gln27 haplotype. These associations suggest that the Arg16/Gln27 haplotype may be associated with more severe respiratory symptoms. A previous Australian study also reported an association between wheeze with a cold and the Arg16 allele (Ramsay et al. 1999). As mentioned previously, however, Weir et al. (1998) found a higher prevalence of the Gly16/Gln27 haplotype in subjects with moderate to severe asthma. The difference from our results may be because our community-based subjects had milder asthma.
Studied in vitro, polymorphisms at positions 16 and 27 have been shown to alter expression of the β2AR protein. The Gly16 form experiences enhanced degradation of the receptor during agonist exposure compared to the Arg16 form, as does the Gln27 form compared with the Glu27 form (Liggett 1997). Drysdale et al. (2000) investigated multiple SNPs in β 2AR and found the haplotype combination of Arg16/Gln27 was associated with a reduced response to β2-agonist (Drysdale et al. 2000). They also found that the β 2AR mRNA and protein levels of this haplotype were significantly reduced compared to other haplotypes. In vivo work with humans has also shown Arg16 subjects have more rapid decline in FEF50 during exercise than Gly16 subjects (Snyder et al. 2006). These results support our association with the Arg16/Gln27 haplotype, and suggest subjects with this haplotype experience more respiratory symptoms due to their reduced response to endogenous catecholamines and β2-agonists.
Furthermore, in vivo studies of the β 2AR polymorphisms and response to β2-agonist therapy have been conducted, and there is accumulating evidence that the Arg16 allele is associated with worse response to β2-agonist (Israel et al. 2000, 2004; Lee et al. 2004; Martinez et al. 1997). Conversely, a study by Tan et al. (1997) found significantly greater bronchodilator desensitisation in Gly16 homozygotes. However, some studies have not found any evidence of an effect of the β 2AR polymorphisms on response to β2-agonist therapy (Hancox et al. 1998; Lipworth et al. 1999). These discrepancies are most likely due to the small sample sizes in most studies, and highlight the need for larger studies to determine more accurately the effect of these polymorphisms on bronchodilator response.
We found that Gln27 homozygotes and individuals with the Arg16/Gln27 haplotype had a higher prevalence of BHR. This is consistent with previous studies that have found individuals with the Glu27 allele to be less responsive to histamine (Ramsay et al. 1999) and methacholine (Hall et al. 1995) than those with the Gln27 allele. Furthermore, an American study that used haplotype estimation also found the Arg16/Gln27 haplotype was positively associated with BHR (Litonjua et al. 2004). However, our results are contrary to those of two other haplotype studies of BHR. One study observed an increased frequency of the Gly16/Gln27 haplotype among BHR-positive subjects, but only studied males, and found a higher overall frequency of the Gly16/Gln27 haplotype in their population than we did in ours (D’Amato et al. 1998). The second study found the Gly16/Gln27/Thr164 haplotype to be underrepresented in the BHR cases compared to the controls, resulting in a protective effect of this haplotype (Ulbrecht et al. 2000). Despite the inconsistencies, there is still mounting evidence to suggest that the β 2AR haplotype influences BHR.
One potential limitation of our study is that we did not determine haplotype directly, but instead inferred phase using the E-M algorithm. There have been some concerns regarding the accuracy of this method; however, recent studies have demonstrated that estimated haplotype frequencies accurately reflect the true frequencies for common polymorphisms (Tishkoff et al. 2000). In line with other studies of Caucasian populations, we have found the Arg16/Glu27 haplotype to be extremely rare. In three previous haplotype studies the Arg16/Glu27 was not found at all, or—if using the E-M algorithm to infer phase—present at extremely low frequencies (D’Amato et al. 1998; Joos et al. 2003; Litonjua et al. 2004; Ulbrecht et al. 2000). The prevalence of the other haplotypes in our study was very similar to those reported in other Caucasian populations (Litonjua et al. 2004; Ulbrecht et al. 2000).
Association studies are susceptible to bias as a result of population stratification caused by ethnic variation within the sample. We have attempted to minimise this bias by analysing only those subjects of Caucasian descent. Due to the number of analyses conducted with many different outcomes, it might be argued that adjustment for multiple comparisons is necessary. However, for both SNPs there was an a priori hypothesis of an individual association with the outcomes studied. This assumption was based on the important role of this gene in modulating response to endogenous and exogenous catecholamines. The associations were consistent across both individual SNPs and the haplotype analysis, which suggests a genuine association. Therefore, the P values for the statistical tests completed are presented as they were performed.
In conclusion, we have shown the Arg16/Gln27 haplotype is associated with COPD, asthma and BHR in middle-aged and older adults. We have provided the first evidence that β 2AR haplotype may be important in COPD. We have provided further evidence that haplotype analysis is important when assessing multiple polymorphisms with functional effects on the receptor. Our results would suggest that β 2AR genotype may be an important modulating factor in risk of COPD, asthma and related phenotypes. This study provides good evidence that further randomised clinical trials of β2-agonist response in specific haplotype groups are needed to fully elucidate the importance of β 2AR haplotypes in modulating response to therapy. In the future, genetic screening for β 2AR genotype may be worthwhile in patients prescribed β2-agonists, to predict those who will most benefit from this type of therapy. This may be particularly relevant to individuals with COPD, and further work is needed to determine what effect β 2AR has on COPD bronchodilator responsiveness.
Abbreviations
- ATS:
-
American Thoracic Society
- β2 :
-
Beta2
- β2AR:
-
β2-Adrenergic receptor
- BHR:
-
Bronchial hyperreactivity
- COPD:
-
Chronic obstructive pulmonary disease
- DLco:
-
Diffusing capacity
- LHS:
-
Lung health study
- MCh:
-
Methacholine
- Ors:
-
Odds ratios
- PCR:
-
Polymerase chain reaction
- RFLP:
-
Restriction fragment length polymorphism
- SNP:
-
Single nucleotide polymorphism
- Tetra-primer ARMS:
-
Tetra-primer amplification refractory mutation system
- 95% Cis:
-
95% Confidence intervals
References
D’Amato M, Vitiani LR, Petrelli G, Ferrigno L, di Pietro A, Trezza R, Matricardi PM (1998) Association of persistent bronchial hyperresponsiveness with beta2-adrenoceptor (ADRB2) haplotypes. A population study. Am J Respir Crit Care Med 158:1968–1973
Dewar JC, Wheatley AP, Venn A, Morrison JF, Britton J, Hall IP (1998) Beta2-adrenoceptor polymorphisms are in linkage disequilibrium, but are not associated with asthma in an adult population. Clin Exp Allergy 28:442–448
Dishy V, Sofowora GG, Xie H, Kim RB, Byrne DW, Stein CM, Wood AJJ (2001) The effect of common polymorphisms of the (beta)(2))-adrenergic receptor on agonist-mediated vascular desensitization. N Engl J Med 345:1030–1035
Drysdale CM, McGraw DW, Stack CB, Stephens JC, Judson RS, Nandabalan K, Arnold K, Ruano G, Liggett SB (2000) Complex promoter and coding region beta 2-adrenergic receptor haplotypes alter receptor expression and predict in vivo responsiveness. Proc Natl Acad Sci USA 97:10483–10488
Gore CJ, Crockett AJ, Pederson DG, Booth ML, Bauman A, Owen N (1995) Spirometric standards for healthy adult lifetime nonsmokers in Australia. Eur Respir J 8:773–782
Green SA, Turki J, Innis M, Liggett SB (1994) Amino-terminal polymorphisms of the human beta-2-adrenergic receptor impart distinct agonist-promoted regulatory properties. Biochemistry 33:9414–9419
Green SA, Turki J, Bejarano P, Hall IP, Liggett SB (1995) Influence of beta-2-adrenergic receptor genotypes on signal trabsduction in human airway smooth muscle cells. Am J Respir Cell Mol Biol 13:25–33
Hall IP, Wheatley A, Wilding P, Liggett SB (1995) Association of Glu 27 beta 2-adrenoceptor polymorphism with lower airway reactivity in asthmatic subjects. Lancet 345:1213–1214
Hancox RJ, Sears MR, Taylor DR (1998) Polymorphism of the beta2-adrenoceptor and the response to long-term beta2-agonist therapy in asthma. Eur Respir J 11:589–593
Hawley ME, Kidd KK (1995) HAPLO: a program using the EM algorithm to estimate the frequencies of multi-site haplotypes. J Hered 86:409–411
Hegab AE, Sakamoto T, Saitoh W, Massoud HH, Massoud HM, Hassanein KM, Sekizawa K (2004) Polymorphisms of IL4, IL13, and ADRB2 genes in COPD. Chest 126:1832–1839
Ho LI, Harn HJ, Chen CJ, Tsai NM (2001) Polymorphism of the beta(2)-adrenoceptor in COPD in Chinese subjects. Chest 120:1493–1499
Hogg JC (2004) Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet 364:709–721
Hopes E, McDougall C, Christie G, Dewar J, Wheatley A, Hall IP, Helms PJ (1998) Association of glutamine 27 polymorphism of beta 2 adrenoceptor with reported childhood asthma: population based study. BMJ 316:664
Hospers JJ, Postma DS, Rijcken B, Weiss ST, Schouten JP (2000) Histamine airway hyper-responsiveness and mortality from chronic obstructive pulmonary disease: a cohort study. Lancet 356:1313–1317
Israel E, Drazen JM, Liggett SB, Boushey HA, Cherniack RM, Chinchilli VM, Cooper DM, Fahy JV, Fish JE, Ford JG, Kraft M, Kunselman S, Lazarus SC, Lemanske RF, Martin RJ, McLean DE, Peters SP, Silverman EK, Sorkness CA, Szefler SJ, Weiss ST, Yandava CN (2000) The effect of polymorphisms of the beta(2)-adrenergic receptor on the response to regular use of albuterol in asthma. Am J Respir Crit Care Med 162:75–80
Israel E, Chinchilli VM, Ford JG, Boushey HA, Cherniack R, Craig TJ, Deykin A, Fagan JK, Fahy JV, Fish J, Kraft M, Kunselman SJ, Lazarus SC, Lemanske RFJ, Liggett SB, Martin RJ, Mitra N, Peters SP, Silverman EK, Sorkness CA, Szefler SJ, Wechsler ME, Weiss ST, Drazen JM, National Heart L, Blood Institute’s Asthma Clinical Research Network (2004) Use of regularly scheduled albuterol treatment in asthma: genotype-stratified, randomised, placebo-controlled cross-over trial. Lancet 364:1505–1512
Joos L, Weir TD, Connett JE, Anthonisen NR, Woods R, Pare PD, Sandford AJ (2003) Polymorphisms in the beta2 adrenergic receptor and bronchodilator response, bronchial hyperresponsiveness, and rate of decline in lung function in smokers. Thorax 58:703–707
Lee DK, Currie GP, Hall IP, Lima JJ, Lipworth BJ (2004) The arginine-16 beta2-adrenoceptor polymorphism predisposes to bronchoprotective subsensitivity in patients treated with formoterol and salmeterol. Br J Clin Pharmacol 57:68–75
Liggett SB (1997) Polymorphisms of the beta2-adrenergic receptor and asthma. Am J Respir Crit Care Med 156:S156–S162
Lima JJ, Thomason DB, Mohamed MH, Eberle LV, Self TH, Johnson JA (1999) Impact of genetic polymorphisms of the beta2-adrenergic receptor on albuterol bronchodilator pharmacodynamics. Clin Pharmacol Ther 65:519–525
Lipworth BJ, Hall IP, Aziz I, Tan KS, Wheatley A (1999) Beta2-adrenoceptor polymorphism and bronchoprotective sensitivity with regular short- and long-acting beta2-agonist therapy. Clin Sci (Lond) 96:253–259
Litonjua AA, Silverman EK, Tantisira KG, Sparrow D, Sylvia JS, Weiss ST (2004) Beta 2-adrenergic receptor polymorphisms and haplotypes are associated with airways hyperresponsiveness among nonsmoking men. Chest 126:66–74
Martinez FD, Graves PE, Baldini M, Solomon S, Erickson R (1997) Association between genetic polymorphisms of the beta2-adrenoceptor and response to albuterol in children with and without a history of wheezing. J Clin Invest 100:3184–3188
Matheson MC, Benke G, Raven J, Sim MR, Kromhout H, Vermeulen R, Johns DP, Walters EH, Abramson MJ (2005) Biological dust exposure in the workplace is a risk factor for chronic obstructive pulmonary disease. Thorax 60:645–651
Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS, Committee GS (2001) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO global initiative for chronic obstructive lung disease (GOLD) workshop summary. Am J Respir Crit Care Med 163:1256–1276
Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J (2005) Interpretative strategies for lung function tests. Eur Respir J 26(5):948–968
Quanjer PH, Dalhuijsen A, van Zomeren BC (1983) Summary equations of reference values. Bull Eur Physiopathol Respir 19:45–51
Ramsay CE, Hayden CM, Tiller KJ, Burton PR, Goldblatt J, Lesouef PN (1999) Polymorphisms in the beta2-adrenoreceptor gene are associated with decreased airway responsiveness. Clin Exp Allergy 29:1195–1203
Reihsaus E, Innis M, MacIntyre N, Liggett SB (1993) Mutations in the gene encoding for the beta-2-adrenergic receptor in normal and asthmatic subjects. Am J Respir Cell Mol Biol 8:334–339
Snyder EM, Beck KC, Dietz NM, Joyner MJ, Turner ST, Johnson BD (2006) Influence of beta2-adrenergic receptor genotype on airway function during exercise in healthy adults. Chest 129:762–770
Summerhill E, Leavitt SA, Gidley H, Parry R, Solway J, Ober C (2000) Beta(2)-adrenergic receptor Arg16/Arg16 genotype is associated with reduced lung function, but not with asthma, in the Hutterites. Am J Respir Crit Care Med 162:599–602
Tan S, Hall IP, Dewar J, Dow E, Lipworth B (1997) Association between beta 2-adrenoceptor polymorphism and susceptibility to bronchodilator desensitisation in moderately severe stable asthmatics. Lancet 350:995–999
Tishkoff SA, Pakstis AJ, Ruano G, Kidd KK (2000) The accuracy of statistical methods for estimation of haplotype frequencies: an example from the CD4 locus. Am J Hum Genet 67:518–522
Toelle BG, Peat JK, Salome CM, Mellis GM, Woolcock AJ (1992) Towards a definition of asthma for epidemiology. Am Rev Respir Dis 146:633–637
Turki J, Pak J, Green SA, Martin RJ, Liggett SB (1995) Genetic polymorphisms of the beta-2-adrenergic receptor in nocturnal and nonnocturnal asthma. J Clin Invest 95:1635–1641
Turner SW, Khoo SK, Laing IA, Palmer LJ, Gibson NA, Rye P, Landau LI, Goldblatt J, Le Souef PN (2004) Beta adrenoceptor Arg16Gly polymorphism, airway responsiveness, lung function and asthma in infants and children. Clin Exp Allergy 34:1043–1048
Ulbrecht M, Hergeth MT, Wjst M, Heinrich J, Bickeboller H, Wichmann HE, Weiss EH (2000) Association of beta(2)-adrenoreceptor variants with bronchial hyperresponsiveness. Am J Respir Crit Care Med 161:469–474
Wang Z, Chen C, Niu T, Wu D, Yang J, Wang B, Fang Z, Yandava CN, Drazen JM, Weiss ST, Xu X (2001) Association of asthma with beta(2)-adrenergic receptor gene polymorphism and cigarette smoking. Am J Respir Crit Care Med 163:1404–1409
Weir TD, Mallek N, Sandford AJ, Bai TR, Awadh N, Fitzgerald JM, Cockcroft D, James A, Liggett SB, Pare PD (1998) Beta-2-adrenergic receptor haplotypes in mild, moderate and fatal/near fatal asthma. Am J Respir Crit Care Med 158:787–791
Xu X, Rijcken B, Schouten JP, Weiss ST (1997) Airways responsiveness and development and remission of chronic respiratory symptoms in adults. Lancet 350:1431–1434
Ye S, Dhillon S, Ke X, Collins AR, Day IN (2001) An efficient procedure for genotyping single nucleotide polymorphisms. Nucleic Acids Res 29:E88–E88
Acknowledgments
We wish to thank Cathryn Wharton, Judi Wicking and Billy Skoric for assistance with data collection, and Nicholas Harrap and Nadia Harun for assistance with DNA extraction. Financial support for this study was provided by The National Health and Medical Research Council, Monash University, LEW Carty Research Fund, Windermere Foundation, Victorian Tuberculosis and Lung Association and the Rebecca L. Cooper Medical Research Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Matheson, M.C., Ellis, J.A., Raven, J. et al. β2-adrenergic receptor polymorphisms are associated with asthma and COPD in adults. J Hum Genet 51, 943 (2006). https://doi.org/10.1007/s10038-006-0043-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10038-006-0043-z
Keywords
This article is cited by
-
Association of β2-adrenergic receptor gene polymorphisms (rs1042713, rs1042714, rs1042711) with asthma risk: a systematic review and updated meta-analysis
BMC Pulmonary Medicine (2019)
-
Asthma: Gln27Glu and Arg16Gly polymorphisms of the beta2-adrenergic receptor gene as risk factors
Allergy, Asthma & Clinical Immunology (2014)
-
Glucocorticoid receptor gene polymorphisms and potential association to chronic obstructive pulmonary disease susceptibility and severity
European Journal of Medical Research (2009)
