
Abstract
Studies have shown that the average drinking water consumption ranges between 0.075 and 3 L/day for adults with both national and regional differences. For exposure assessment of drinking water hazards, country-specific drinking water consumption data including sources of the consumed water may therefore be warranted. To estimate the amount and source of drinking water consumed among adults in Sweden, we collected self-reported estimates using both traditional methods (telephone interviews, web questionnaire) and a novel method (Short Message Service, SMS questionnaires) in a population from an average sized Swedish municipality. Monthly SMS questionnaires were sent out during one year to obtain longitudinal information as well. SMS showed to be a promising tool for collecting self-reported consumption, as most citizens could participate and the method showed high response rate. Data collected via the SMS questionnaire shows an average consumption of cold tap water of 4.9 glasses/24 h (one glass=200 ml), while the average estimates of cold tap water collected by the traditional methods range from 4.5 to 7.0 glasses/24 h. For statistical distributions, the mean daily consumption of cold tap water for the population was best fitted to a gamma distribution. About 70% of the cold tap water is consumed at home. Based on the results from the SMS study, we suggest using 1 l/day for the average adult population and 2.5 l/day for high consumers for risk assessment of cold tap water consumption. As 46% of the tap water consumed is heated, we suggest using 1.85 l/day for total tap water consumption.
Similar content being viewed by others

INTRODUCTION
In the industrialized world, drinking water is generally associated with low health concern. Large drinking water related outbreaks1, 2, 3 and findings of harmful substances4 in drinking water during recent years have increased the awareness of the vulnerability of the drinking water supply and that consumers may be at risk. To evaluate the need for risk reducing measures to sustain good quality tap water, models for risk assessment have been developed, e.g. quantitative microbial risk assessment (QMRA)5. These models demand accurate consumption data to make realistic risk assessments. As examples of reference values for drinking water consumption, World Health Organization (WHO) has adopted 2 L as a standard quantity of daily consumption of drinking water for adults,6 while European Food Safety Authority (EFSA) recently suggested using 2 L for females and 2.5 L for males for total daily water consumption from beverages and food.7 A reference value may be sufficient for risk assessment in general, but international studies have shown that the average drinking water consumption for adults range between 0.075 L/day and 3 L/day for adults,8, 9, 10, 11 showing both national and regional differences.9, 11, 12, 13, 14 Using reference values for risk assessments may overestimate exposure to certain hazards where only a specific water source (e.g. raw water source used for drinking water production) may be relevant or only unheated water poses a risk, like microbial hazards or volatile chemicals. Country-specific drinking water consumption data,11 as well as information on sources of the consumed water and information on the total consumption of cold and heated tap water, may therefore be warranted.
Collecting information on consumption is highly affected by the method used, timing of the study and the population under study.12, 13, 14, 15, 16 Most water consumption data are based on single measurements while repeated individual data take into account intra-individual day-to-day variation, reducing the risk of systematic and random errors, as consumption may vary between days of the week or seasons.13, 15, 16, 17, 18 Repeated individual estimates are also highly useful when statistical distributions are preferred, for example in risk assessment models.11 Lack in motivation and drop-out is common when collecting repeated measurements, but may be overcome by rewarding the participants.19, 20 Paper questionnaires and telephone interviews are commonly used for prospective cohort studies, but the use of telephone interviews has lately been compromised as a collecting method due to decreases in landline subscribers and the unwillingness to answer unknown phone calls.20 The near-ubiquitous use of mobile telephones, give rise to new ways of collecting data through Short Message Services (SMS) or mobile app surveys. SMS surveys have previously been used for data collection in medical research and have been shown to give as high data quality as telephone interviews, but to a lower cost and with a higher response rate.21, 22, 23
The aims of this paper are to i) present new data on statistical distributions and consumption patterns of self-reported cold tap water consumption as well as data on the use of different water sources among adults for self-reported cold tap water consumption that can be used for health risk assessment and ii) present new data for self-reported drinking water consumption patterns from different water sources among adults in Sweden, as well as iii) to compare self-reported cold tap water consumption, collected using traditional methods for collecting single estimates (point estimates from nationally representative telephone interviews and web questionnaires) and a novel method (SMS) for collecting repeated individual estimates.
METHODS
Study Population
The main part of the self-reported consumption was collected from the adult population between the age of 18 and 80 years living in Ale, a municipality in the south-western part of Sweden. This municipality was chosen as the demographical distribution resembles that of Sweden as a whole.24 At the time of the study, the municipality had ~28 000 inhabitants, an average sized municipality by Swedish standards, and two thirds of the inhabitants were living in urban areas. The rural population received their tap water from private wells (drilled or dug wells), and the urban population from either of two municipal water treatment plants. Prior to the study, information on the study and the upcoming recruitment to the cohort were advertised in the local newspaper, on the homepage of the National Food Agency and the homepage of the municipality of Ale. To evaluate if the self-reported water consumption in the local study in Ale were representative, nationwide consumption data were collected in parallel to two of the telephone interview surveys conducted in Ale (representative selection of nationwide participants in the age 18 to 80 years). Oral informed consent was obtained from all participants and the regional ethical review board (Uppsala, Sweden) approved the study. Swedish language was exclusively used in all parts of the study; participation was thus limited to citizens mastering Swedish.
Initial telephone interviews and recruitment to SMS survey
In early 2012, computer assisted telephone interviews were carried out in Ale (TelAle1) and nationwide (TelSwe1) by professional interviewers (Figure 1 and Table 1). The national consumer register (PAR, including 87% of the Swedish population older than 16 years) was used for obtaining a representative selection of respondents in the adult population based on age and sex (landline telephone numbers). Respondents residing on average less than five days a week in Ale or having chronic/recurring gastrointestinal illness were excluded at an early stage of the interviews. Respondents were asked about their consumption of cold drinking water from the tap at home and away (in glasses, one glass equalling 200 ml), and bottled water during the past 24 h (recall), as well as other background information for categorizing the participants into representative panels (age, sex, household information). They were further informed to include water used for dilution of juices and water from tap-connected water dispensers etc., but to exclude bottled water, water from the hot water tap (>50 °C according to building regulations), and heated or boiled water. To validate that 200 ml is a “standard serving”; an interactive national web questionnaire was conducted with 116 respondents (data not shown). The results showed that a glass of water on average contained 225 ml and when participants were asked to estimate of a fixed volume (200 ml), they were on average off by 12% (average 176 ml). The respondents in TelAle1 were given the opportunity to continue their participation in the subsequent one-year SMS survey (12mSMS). The aim was to complete 4 000 interviews in TelAle1 and 1 000 national representative interviews in TelSwe1.

Schematic view of the data collection 2012–2013. Participants were recruited to the one-year SMS study (12mSMS) by telephone interviews in the municipality of Ale (TelAle1). Additional telephone interview (TelAle2), a seven-day SMS study (7dSMS) as well as a web questionnaire was conducted for either a representative selection of participants or all participants in 12mSMS. Two nationwide telephone interview surveys (TelSwe1, TelSwe2) were conducted in parallel with the telephone interviews in Ale.
Twelve-month SMS survey (12mSMS)
Sixty-seven per cent of the respondents in TelAle1 were interested in participating in 12mSMS (Figure 1, Table 1) and were thus invited to join the study. Participants received instruction and information letters prior to and during 12mSMS. Participants were categorized into two sub-panels, as identical as possible with respect to the distribution of sex, age, water source and daily water consumption (as reported at recruitment, one glass equalling 200 ml), and each of the two sub-panels received monthly questionnaires either around the turn of or in the middle of each month, from March 2012 to February 2013. SMS questionnaires were sent out according to a pre-set schedule, ensuring an even distribution between days of the week over the entire year. Questions were always sent at 10 AM and 24 h prior to the SMS questionnaire, a pre-reminder SMS was sent out, reminding the participants to keep record of their consumption during the next 24 h. In the SMS questionnaires, participants were asked to report the amount of cold tap water (in glasses) that they had consumed in the past 24 h. Participants were informed not to answer if they had been away from home for a continuous period of at least seven days during the last 28 days. As a reimbursement and an encouragement to continue participation in the survey, participants received a lottery scratch card (value approx. €1) each month they completed an SMS questionnaire.
Additional telephone interviews
Close to the end of 12mSMS, self-reported habitual average daily consumption (recall) and 24 h consumption (recall) of drinking water (in glasses) were collected from participants via telephone interviews (TelAle2) (Figure 1 and Table 1). The aim of this second telephone interview was to collect additional information on different water consumption sources (i.e. cold tap water home and away, bottle etc. that were not collected in the 12mSMS) and to assess the influence on reporting by prior participation in 12mSMS. The selection of participants in the TelAle2 was a subset from 12mSMS, based on age, sex and average self-reported water consumption (equal numbers of participants were selected from each quartile of average consumption of all the participants in 12mSMS). Nationwide interviews were conducted simultaneously with a new selection of participants (TelSwe2), in order to confirm the results from the previous nationwide telephone interviews (TelSwe1). During TelAle2, the participants were also asked if they would like to participate in a one-week daily SMS survey (7dSMS). We aimed at completing 1000 interviews in both TelAle2 and TelSwe2.
Additional one-week daily SMS survey (7dSMS)
Three-quarters of the respondents in TelAle2 were interested in participating in 7dSMS (Figure 1, Table 1). The aim of 7dSMS was to obtain information on the cold tap water consumption pattern on different days of the week during a one week period, to confirm results from 12mSMS. The selection of participants receiving an SMS invitation to 7dSMS was based on age, sex and average self-reported water consumption, with an equal number of participants selected from each consumer group (quartiles of average consumption of all participants in 12mSMS). Of those that had confirmed their interest during TelAle2 (75%), 53% were sent an SMS invitation and 74% of these agreed to participate in the 7dSMS during one week in March 2013. The participants received their SMS questionnaires during all the seven days at 10 AM and were asked to report their consumption during the past 24 h as in 12mSMS, but no 24 h pre-reminder was sent out due to the distribution of questionnaires every 24 h.
Web questionnaire on consumption of beverages in general
All participants in 12mSMS were invited to join a final web questionnaire (Web) (Figure 1 and Table 1). Data on the frequency of consumption and the daily consumption of tap water, heated and unheated, as well as other beverages were collected (recall) to be able to estimate the amount of tap water consumed in relation to total fluid intake/other beverages. Information on water used for cooking was not collected. In Web, the participants were asked about their drinking water consumption in decilitres during the last 24 h. Information on physical activity, health status, educational level, socio-economic factors and other confounding factors were collected as well.
Statistical Analyses
In the analyses of the cold tap water consumption in the 12mSMS, the participants were assigned into consumer quartiles according to their mean daily self-reported consumption from the twelve SMS questionnaires. The Kruskal-Wallis test was used to assess differences in the average water consumption between groups in 12mSMS. Spearman’s rank test (rho) was used to assess the correlation between self-reported consumption data from the all data sets (single and average reported consumption). Random-effect generalized least squares regression was used for estimating the intra-individual correlation of the estimates reported in in 12mSMS. This analysis does not permit zero samples, accordingly non-consumers received an average of 0.0001 glasses.
Average cold (unheated) water consumption exceeding 20 glasses/24h (4 l/24h), single self-reported estimates exceeding 30 glasses/24 h (6 l/24 h), (excluding 0.2% of the single consumption estimates of 12mSMS) and total beverage consumption exceeding 10 l/24 h in Web were considered unlikely and therefore excluded (high estimates were reported at random). Participants that were retrospectively found not to fulfil the criteria of residence within the study area were excluded from the analyses (0.1% of the original participants). Only participants completing at least two of the 12 SMS questionnaires were included, excluding 12% (either non-respondents or those who answered only one SMS questionnaire; Table 1). Statistical analyses were performed using Stata 12.1 (StataCorp, Texas, USA) and R version 3.2.3 (R Core Team [2015], R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Participation, Response Rate and Drop-Out
The response rate during the telephone interviews in Ale and nationwide were 38–56% of the total number of persons contacted (Table 1). The participants were evenly distributed among the age groups <40, 40–54 and >54 years, and sex in all studies conducted (Table 2). Out of the 67% that showed an interest in participating in 12mSMS, 88% completed at least two SMS questionnaires (included in the statistical analyses) and 73% of all participants answered at least ten SMS questionnaires.
Consumption Patterns
In telephone interviews, the average daily consumption of 6.4 and 7.0 glasses/24 h in Ale (TelAle1 and TelAle2, respectively) did not differ significantly from the reported consumption nationwide (TelSwe1: 6.1 glasses/24 h, P=0.6; TelSwe2: 6.9 glasses/24 h, P=0.6), indicating that the results from the study population in Ale were nationally representative.
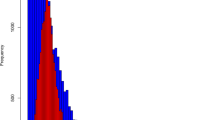
The average self-reported individual consumption in 12mSMS were not normally distributed, instead best fitting a gamma distribution (shape=3.938; rate=0.791: in glasses equalling 200 ml) (Figure 2 and 3). The average self-reported cold tap water consumption for each participant (individual averages) was 4.9 glasses/24 h (median 4.6, 90th percentile 8.3 and 99th percentile 12.7 glasses/24 h, respectively; Figure 4). Non-consumers of cold tap water constituted 0.2% of all participants. For all single self-reported estimates (point estimates, not individual averages) in 12mSMS, the mean daily consumption was 5 glasses/24 h (90th percentile 9 and 99th percentile 15 glasses/24 h, respectively; Figure 5).

Theoretical densities of the mean daily consumption of cold tap water in the one-year SMS study (12mSMS). Figure shows Weibull, gamma and lognormal distributions, and their parameter values, fitted to the data.

Q-Q-plot for the distribution of the mean daily consumption of cold tap water and the theoretical distribution in the one-year SMS study (12mSMS). Figure shows Weibull, gamma and lognormal distributions fitted to the data.

Distribution of the average individual number of self-reported glasses (200 ml) of cold tap water consumed daily during in the one-year SMS study (12mSMS) for all participants (n=2 345).

Distribution of all single self-reported glasses (200 ml) cold tap water consumed daily (n=23 929) in the one-year SMS study (12mSMS) for all participants.
Women had a significantly higher daily mean consumption than men in 12mSMS (5.4 and 4.5 glasses/24 h respectively, P<0.001), while there was no statistically significant difference between the three age groups (P=0.07) (Table 3). The average self-reported consumption was slightly lower for participants receiving water from private wells compared to municipal water during the entire year, although the difference was not statistically significant (P=0.3) (Figure 6). Educational level (P=0.08), travel abroad (P=0.1) or time spent at home (P=0.98) did not have any apparent effect on the consumption. In contrast, participants with physically demanding working conditions (P=0.005), regular exercise (P<0.001) and lower perceived health status (P=0.02) had significantly higher average self-reported consumption (data not shown).

Average self-reported daily consumption of cold tap water (24 h) during the course of the one-year SMS study (12mSMS; n=23 929). Consumption is reported in number of glasses (1 glass=200 ml).
There was a significant difference between single self-reported consumption made on different days of the week (P<0.001) in 12mSMS, with the highest self-reported consumption observed for Monday to Thursday (average 5.1 glasses/24 h, data not shown) that was significantly different from the lowest observed self-reported consumption for Saturday to Sunday (average 4.4 glasses/24 h, data not shown). In 7dSMS there was, however, no significant difference between days of the week, but similar trends as in 12mSMS could be observed, strengthening the results from 12mSMS. Difference in consumption between seasons was not possible to assess due to the design of the study.
About 40% of the participants made a consumption estimate that was within the same consumer quartile after the first SMS questionnaire as their average consumption during the entire study period (Figure 7). After seven self-reported consumption estimates during different days of the week, 80% had reached their final consumer quartile. In addition, the intra-individual correlation was fairly high (rho=0.6) for the individual consumption estimates in the entire 12mSMS.

Number of single self-reported consumption estimates (consumption during 24 h) of cold tap water consumption needed for participants to reach their final consumer group (quartiles of average consumption of all participants) in the one-year SMS study (12mSMS).
Sources of Drinking Water
In Web, single self-reported consumption of heated drinking water and other beverages were collected. The results show that 78% of the total non-alcoholic beverage consumption is tap water of which 42% is consumed cold, while 36% is heated drinking water (tea, coffee, etc.). As much as 9% of the respondents reported that they occasionally consumed water directly from the hot water tap.
In TelAle1, TelAle2 and 7dSMS, self-reported cold tap water consumption at home and away from home were collected separately. The results showed that consumption of cold tap water at home constituted 65–73% of the total cold tap water consumption per day (Table 4). Similar results were obtained in the two nationwide interviews, in which on average 66% (TelSwe1) and 75% (TelSwe2) of the cold tap water was consumed at home.
Four of the surveys made in Ale contained questions concerning bottled water (Table 4). At least 84% of the responding participants in all the surveys reported to be non-consumers of bottled water (24 h). The average consumption among those who did consume bottled water ranged between 2.2 and 6.3 glasses/24 h, results similar to the nationwide interviews.
Comparison of Different Data Collection Methods
The average self-reported consumption of cold tap water reported by the study population in Ale, ranged between 4.5 glasses/24h and 7.0 glasses/24 h, with the lowest reported average in Web and the highest in TelAle2 (Table 4). In comparison to the average individual consumption in 12mSMS, the first telephone interview, TelAle1, showed the lowest correlation (Table 4).
DISCUSSION
In this fairly large study on individual self-reported water consumption from various sources we evaluated different sampling techniques and obtained new statistical distributions and consumption estimates for drinking water consumption for the Swedish adult population using SMS questionnaires. To our knowledge, SMS has not previously been used for collecting repeated consumption measurements.
Consumption of Drinking Water
The mean daily consumption estimate (in glasses equalling 200 ml) from our study fits a gamma distribution with the parameter values 3.938 (shape) and 0.791 (rate). For statistical modelling of exposure of hazards via cold tap water in regions that have similar consumption patterns as in Sweden, we therefore suggest fitting drinking water consumption data to a gamma distribution. Previous studies have suggested using lognormal or Poisson distribution for drinking water consumption.11, 14 Although the average consumption data fits a lognormal distribution fairly well, the gamma distribution is best fitted to the average consumption in 12mSMS presented in this paper.
The median mean daily consumption of cold tap water in 12mSMS was 1 L/day. For risk assessment, besides using the median, we suggest using the 99th percentile of the average consumption (2.5 L/day) as well, to represent average high-consumers. If risk assessment is being made only on cold tap water consumed at home, we suggest using a factor of 0.7, since five of the surveys in our study showed that 65–75% (on average about 70%) of the total cold tap water is consumed at home. For total consumption of drinking water (heated or unheated), we suggest using a factor of 1.85 to the cold water consumption, as this study showed that on average 46% of the tap water was consumed heated (e.g. tea and coffee). This more or less supports the notion of WHO to use 2 litres as a standard quantity of total daily consumption of drinking water.6 Data on drinking water used in cooking was not collected in this study and is therefore not included in the recommendations for risk assessment presented in this paper. We also like to point out that 9% of the participants consume warm tap water, which may be of relevance for risk assessment of some chemicals. Even though there are significant differences within the population, e.g. between sexes, we only recommend to consider these differences in cases where chronic exposure is assessed, since the difference between subpopulations are not large enough to be considered relevant for acute exposure.
Previous data on drinking water consumption patterns in Sweden14, 25, 26 reported the average drinking water consumption to range between 483 ml heated and unheated water/day26 to 860 ml unheated water/day,14 which is considerably lower than the results in the present study. Potential explanations include changes in consumption trends over time and differences due to data collection methods. Previous Swedish drinking water consumption data were either collected as part of a 7-day diet diary;25 a 4-day web-based diet diary;26 as part of an outbreak investigation in which information on water consumption was collected retrospectively for a period of one month;27 or as part of a questionnaire in which the daily average consumption of tap water was investigated.28 Data collection method-related differences in the self-reported consumption were also observed in the present study, although all data collection was performed within the same study population during a one-year period.
The self-reported consumption presented in this paper show that Swedes have a fairly average drinking water consumption compared to results reported in international studies.8, 9, 10, 11 While international studies show higher drinking water consumption among men compared to women,9 the present results indicate a higher consumption of cold tap water among women than men—in line with previous Swedish studies, indicating a potential country-specific phenomenon. In this study we did not collect data on pregnancy and lactation among women although this may have been relevant for the consumption.
In an international comparison, our study demonstrates an unusually low proportion of consumers of bottled water, which also might indicate a country-specific phenomenon.14 The reason for choosing bottled water may be cultural, but may also be due to consumers' notion on taste, risk perception of tap water and trust in public water utilities.29 In Sweden consumers have a high trust towards their drinking water and consume it regularly,30 and therefore Swedes may prefer tap water instead of bottled water. In contrast to a previous study in Sweden14 and in previous international studies,12, 13 we did not see any significant difference in the average consumption between rural (having private wells) and urban areas (municipal water source), although the participants in the rural areas had slightly lower average consumption compared to the urban areas during the entire 12mSMS.
Data Collection Methods and Study Limitation
The results presented in this paper show that using single self-reported consumption estimates (point estimates) in 12mSMS give a similar result as the individual average consumption during repeated estimates, although there are differences in the high percentiles. This is true for both 24 h recall consumption as well as self-reported habitual daily consumption. The first self-reported consumption in 12mSMS showed that about 40% of the participants estimated their consumption within the same consumer quartiles as their final average consumption. After seven consumption estimates in 12mSMS, almost 80% of the participants had reached their final consumer group, indicating that up to seven estimates might be required to obtain fairly accurate average individual consumption of the study population. The self-reported consumption in 12mSMS also showed a high intra-individual correlation, meaning that most participants in the study reported a similar consumption over the year. In previous studies, reported drinking water consumption from the first and the second day of diaries has shown to be higher than the average of repeated consumption estimates,31 indicating an adjustment or learning period, alternatively changes in consumption and/or reporting patterns. As the consumption during TelAle1 and the first single self-reported consumption estimates during 12mSMS is around 20% higher compared to the average during 12mSMS, such an adjustment period may exist in our study as well. In spite of the mean cold tap water consumption in TelAle2 (after participating in 12mSMS for eight months) being higher than the corresponding mean cold water consumption in TelAle1 (prior to 12mSMS), the single consumption estimates from TelAle2 displayed a better correlation with the average consumption in 12mSMS, strengthening the theory of an adjustment period.
Respondents in this study were informed in all study parts that 200 ml is a “standard serving” of tap water. International studies have assumed a glass of water to be 150 to 250 ml.11, 32, 33 In our validation of a “standard serving”, 225 ml was shown to be an average serving for tap water among Swedes, but the same participants were off by 12% when estimating a fixed volume. As participants in the cohort were informed to estimate their intake in a fixed volume in all study parts, we were confident to use 200 ml when recalculating glasses into volume. Although using a “standard serving” affects the validity in the study, we consider this to be the most accurate measure for the study design.
Participation in 12mSMS required a mobile phone and the knowledge on how to send SMS. Most participants completed the questionnaires without problems, but there were rare problems with sending and receiving SMS due to technical problems or participants simply not being familiar with how to answer SMS. Problems were solved in most cases, but in some cases participants decided to leave the study. Twenty-five individuals that confirmed their participation in the study, but did not answer any SMS questionnaires, were interviewed about their reason for drop-out (data not shown). The most common reason was either that they never received any SMS questionnaires or could not answer an SMS due to technical problems or did not know how to answer an SMS. Other reasons were lack of time, forgetting to answer or due to the cost of answering the SMS. For future studies we therefore suggest that respondents at an early stage confirm their participation via SMS, confirm that the correct mobile telephone number is used and that the participants are indeed familiar with using SMS. This was successful in 7dSMS, with only a 2% drop-out after the participants had confirmed their participation via SMS.
The main aim of 12mSMS was to collect information on gastrointestinal illness (GI) that may be associated with tap water consumption and the design of the study as well as the time period when the study was conducted, may therefore have affected the response rate. Due to the large outbreak of waterborne cryptosporidiosis in the Swedish city of Östersund in 2012, 750 km away from the study area,1 drinking water related gastroenteritis was discussed frequently in Sweden, something that may have increased the general response rate. The reward of a scratch card for every completed SMS questionnaire may also have increased the participation rate, especially over time. The response rate decreased slightly during vacation periods, and this may be explained by the fact that the participants were advised not to answer the SMS questionnaire if they had been away from home during a continuous period of 7 days, within the last 28 day period (the reason for this was related to reporting of GI, as we did not want participants to report travellers’ diarrhoea). For future SMS questionnaire studies, it might therefore be preferable to allow participants to indicate reason for non-response, instead of leaving the questionnaires unanswered. Still, 73% of all that showed an interest in participating in 12mSMS during TelAle1completed at least ten SMS questionnaires, and therefore we may conclude that the response rate in the 12mSMS study was high.
CONCLUSIONS
For statistical modelling of exposure of hazards via cold tap water in regions that have similar consumption patterns as in Sweden, we suggest fitting consumption data to a gamma distribution. For risk assessment of cold tap water consumption for the adult population in Sweden, we suggest using 1 L/day for the average population and 2.5 L/day for high consumers. If risk assessment is being made exclusively on cold tap water consumed at home, we suggest using a factor of 0.7 and for the total consumption of tap water (heated or unheated) we suggest using a factor of 1.85 to the cold water consumption.
Using SMS is a promising data collection tool, with a high response rate, it is user-friendly and a method most people can use. If accurate drinking water consumption data are required on the individual level, we recommend using at least seven single consumption estimates via SMS. To collect consumption data only during one week of the year, will give a fairly accurate average consumption for drinking water, but we highly suggest making the data collection during several months if there is reason to believe that seasonal variation is high and may affect the average consumption.
References
Widerström M, Schönning C, Lilja M, Lebbad M, Ljung T, Allestam G et al. Large Outbreak of Cryptosporidium hominis Infection Transmitted through the Public Water Supply, Sweden. Emerg Infect Dis. 2014; 20: 581–589.
Laine J, Huovinen E, Virtanen MJ, Snellman M, Lumio J, Ruutu P et al. An extensive gastroenteritis outbreak after drinking-water contamination by sewage effluent, Finland. Epidemiol infect 2011; 139: 1105–1113.
Jakopanec I, Borgen K, Vold L, Lund H, Forseth T, Hannula R et al. A large waterborne outbreak of campylobacteriosis in Norway: the need to focus on distribution system safety. BMC Infect Dis 2008; 8: 128.
Lieberman A . Recovery efforts in Flint slowly begin to take form. Lancet 2016; 387: 1499–1500.
Haas CN, Rose JB, Gerba CP . Quantitative Microbial Risk Assessment. Wiley. 1999.
WHO Nutrients in Drinking Water 2005.
EFSA Panel on Dietetic Products NaAN. Scientific Opinion on Dietary Reference Values for water. Opinion of the Scientific Committee/Scientific Panel 2010.
Watanabe C, Kawata A, Sudo N, Sekiyama M, Inaoka T, Bae M et al. Water intake in an Asian population living in arsenic-contaminated area. Toxicol Appl Pharmacol. 2004; 198: 272–282.
Ozen AE, Bibiloni MD, Pons A, Tur JA . Fluid intake from beverages across age groups: a systematic review. J Hum Nutr Diet. 2015; 28: 417–442.
Ribas-Barba L, Serra-Majem L, Salvador G, Castell C, Cabezas C, Salleras L et al. Trends in dietary habits and food consumption in Catalonia, Spain (1992-2003). Public Health Nutr. 2007; 10: 1340–1353.
Mons MN, van der Wielen JM, Blokker EJ, Sinclair MI, Hulshof KF, Dangendorf F et al. Estimation of the consumption of cold tap water for microbiological risk assessment: an overview of studies and statistical analysis of data. J Water Health. 2007; 5 (Suppl 1): 151–170.
Hynds PD, Misstear BD, Gill LW . Investigation of water consumption patterns among Irish adults for waterborne quantitative microbial risk assessment (QMRA). J Water Health. 2012; 10: 453–464.
Barraj L, Scrafford C, Lantz J, Daniels C, Mihlan G . Within-day drinking water consumption patterns: results from a drinking water consumption survey. J Expo Sci Env Epid 2009; 19: 382–395.
Westrell T, Andersson Y, Stenström TA . Drinking water consumption patterns in Sweden. J Water Health. 2006; 4: 511–522.
Malisova O, Bountziouka V, Panagiotakos D, Zampelas A, Kapsokefalou M . Evaluation of seasonality on total water intake, water loss and water balance in the general population in Greece. J Hum Nutr Diet. 2013; 26 (Suppl 1): 90–96.
Gofti-Laroche L, Potelon JL, Da Silva E, Zmirou D . Description of drinking water intake in French communities (E.MI.R.A. study). Rev Epidemiol Sante Publique. 2001; 49: 411–422.
Bhargava A, Forthofer R, McPherson S, Nichaman M . Estimating the variations and autocorrelations in dietary intakes on weekdays and weekends. Stat Med. 1994; 13: 113–126.
Baranowski T . 24-Hour Recall and Diet Record Methods. In: Willett W edr. Nutritional Epidemiology. Third Editioned. Oxford University Press: USA. 2013.
Payment P, Siemiatycki J, Richardson L, Renaud G, Franco E, Prevost M . A prospective epidemiological study of gastrointestinal health effects due to the consumption of drinking water. Int J Environ Heal R. 1997; 7: 5–31.
O'Toole J, Sinclair M, Leder K . Maximising response rates in household telephone surveys. BMC Med Res Methodol 2008; 8: 71.
Johansen B, Wedderkopp N . Comparison between data obtained through real-time data capture by SMS and a retrospective telephone interview. Chiropr Osteopat 2010; 18: 10.
Kew S . Text messaging: an innovative method of data collection in medical research. BMC Res Notes 2010; 3: 342.
Kongsted A, Leboeuf-Yde C . The Nordic back pain subpopulation program—individual patterns of low back pain established by means of text messaging: a longitudinal pilot study. Chiropr Osteopat 2009; 17: 11.
SCB. Statistics Sweden: Population statistics, 2012-2013. 2015.
Becker W, Person M . Food Habits and Nitritional Intake of the Population Methods and Result analysis. In: Dietary Habits and Nutrient Intake in Sweden 1997-1998. National Food Agency: Uppsala, Sweden. 2002.
Amcoff E, Edberg A, Barbieri HE, Lindroos AK, Nälsén C, Pearson M et al. The Food and Nutrient Intake Among Adults in Sweden. National Food Agency: Uppsala, Sweden. 2012.
Carrique-Mas J, Andersson Y, Petersen B, Hedlund KO, Sjögren N, Giesecke J . A norwalk-like virus waterborne community outbreak in a Swedish village during peak holiday season. Epidemiol Infect. 2003; 131: 737–744.
Anonymous. [Environmental health report] Miljöhälsorapport. The National Board of Health and Welfare, Institute of Environmental Medicine, Stockholm County Council 2001.
Doria MF . Bottled water versus tap water: understanding consumers' preferences. J Water Health. 2006; 4: 271–276.
SKL. [Criticism on engeneering 2013 - Report from customer surveys in technical management]. Stockholm, Sweden 2013.
Levallois P, Guevin N, Gingras S, Levesque B, Weber JP, Letarte R . New patterns of drinking-water consumption: results of a pilot study. Sci Total Environ. 1998; 209: 233–241.
Robertson B, Forbes A, Sinclair M, Black J, Veitch M, Pilotto L et al. How well does a telephone questionnaire measure drinking water intake? Aust Nz J Publ Heal 2000; 24: 619–622.
Maskiell KE, Heyworth JS, McCaul KA . Validation of a water consumption questionnaire for a study of the adverse health outcomes associated with disinfection by-products. Int J Environ Heal R. 2006; 16: 145–153.
Acknowledgements
The study was financed by the Swedish Civil Contingencies Agency and the EU programme Interreg IV A Öresund-Kattegatt-Skagerak.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Säve-Söderbergh, M., Toljander, J., Mattisson, I. et al. Drinking water consumption patterns among adults—SMS as a novel tool for collection of repeated self-reported water consumption. J Expo Sci Environ Epidemiol 28, 131–139 (2018). https://doi.org/10.1038/jes.2017.8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jes.2017.8
Keywords
This article is cited by
-
Predicting factors of public awareness and perception about the quality, safety of drinking water, and pollution incidents
Environmental Monitoring and Assessment (2022)
-
Association between magnesium in drinking water and atrial fibrillation incidence: a nationwide population-based cohort study, 2002–2015
Environmental Health (2021)
