
Abstract
Research on asbestos exposure in Libby, MT, has focused on occupational exposure in vermiculite mining and processing, but less attention has been paid to asbestos-related mortality among community members without vermiculite mining occupational history. Our study reports on asbestos-related mortality in Libby over 33 years (1979–2011) while controlling for occupational exposure. We calculated sex-specific 33-year standardized mortality ratios (SMRs) for Libby residents who died from 1979 to 2011 with an asbestos-related cause of death. Decedent address at time of death was geocoded to confirm inclusion in the Libby County Division. We controlled for past W.R. Grace employment by including and then removing them from the SMR analysis. Six hundred and ninety-four decedents were identified as having at least one asbestos-related cause of death and residing in our study area boundary. Statistically significant (P<0.05) 33-year SMRs, both before and after controlling for W.R. Grace employment, were found for: male and female non-malignant respiratory diseases, female COPD, and asbestosis for both sexes combined. Eighty-five men and two women were matched to employment records. We observed elevated asbestos-related mortality rates among males and females. SMR results for asbestosis were high for both sexes, even after controlling for past W.R. Grace employment. These results suggest that the general population may be experiencing asbestos-related effects, not just former vermiculite workers. Additional research is needed to determine whether SMRs remain elevated after controlling for secondary exposure, such as living with vermiculite workers.
Similar content being viewed by others

INTRODUCTION
Asbestos-contaminated vermiculite was mined and processed in Libby, Montana, from the 1920s through 1990.1 Vermiculite ore in Libby is contaminated up to 26% with amphibole asbestos. Libby amphibole is mostly comprised of the unregulated amphiboles, winchite (84%) and richterite (11%), and regulated asbestiform fibers, tremolite (6%).2 The only chemical difference in these amphiboles is their iron content and their mineralogical difference is minimal and may have no biological significance.3
The highest occupational and environmental exposures to asbestos-contaminated vermiculite likely occurred from the 1950s to the 1970s.4 During this time, there were both peak production volumes and a lack of engineering controls. W.R. Grace, the company that owned the mine, measured environmental asbestos in Libby at levels ranging between 1.0 and 1.5 fibers/ml air in 1975.5 The mine closed in 1990. The site was added to the US Environmental Protection Agency’s National Priorities List (NPL) in 2002 and remains a Final NPL site today.
Although much of the past research has focused on occupational exposures, Libby vermiculite has been associated with adverse health effects among both workers and community members with no mining or vermiculite processing involvement.6 Studies have also been performed on occupational cohorts at sites that received Libby vermiculite around the country, where workers may have also encountered higher than average levels of asbestos exposure through various stages of processing.7, 8
In 2002, the Agency for Toxic Substances and Disease Registry (ATSDR) published a report on asbestos-related mortality in Libby looking at community residents from 1979 to 1998 in six overlapping geographic boundaries.9 This period was selected to reflect the period of time when exposures were at their peak (1950s–1970s) and a minimal induction/latency period (20–30 years) had occurred. Even with the minimal induction/latency period, the authors found that malignant respiratory deaths were 20–40 times higher and non-malignant respiratory deaths, especially asbestosis, were at least 40 times higher than expected.9
There are two objectives for the current study. First, the authors update mortality surveillance since the 2002 ATSDR Health Consultation by adding 13 years of data (1999 to 2011). Specifically, standardized mortality ratios (SMRs) for asbestos-related mortality in Libby, Montana, from 1979 to 2011 were calculated using mortality data from the United States for comparison. Second, we controlled for community exposures in non-workers by removing past W.R. Grace employees from the SMR analysis.
METHODS
Decedent Selection Criteria
To assess asbestos-related mortality among Libby residents, we retrieved death certificate data from the Montana Department of Public Health and Human Services (MDPHHS). Decedent selection criteria included:
-
1
All decedents in the 2002 ATSDR report
-
a
Libby was listed as City of Residence on decedent’s death certificate;
-
b
Death occurred between 1979 and 1998; and
-
c
The underlying cause of death matched one of the specified causes of death (see section Asbestos-Related Causes of Death).
-
a
-
2
Decedents who died between 1999 and 2011
-
a
Libby was listed as City of Residence on decedent’s death certificate;
-
b
The underlying cause of death matched one of the specified causes of death included in the study.
-
a
For Libby residents whose deaths occurred outside of Montana, MDPHHS was unable to provide full records on those decedents. Therefore, death certificates were requested from the health department in the state in which the decedent died and residential address as reported on the complete death certificate record was used in the same way as the records provided by MDPHHS.
Asbestos-Related Causes of Death
Cause of death is coded on the death certificates using the ninth and tenth International Classification of Diseases (ICD-9 and ICD-10). Given that a change occurred in 1999 in how deaths were coded, we refer to asbestos-related mortality by category and subcategories. The categories selected are based on previously published research:9, 10, 11, 12
-
1
Malignant neoplasms of the digestive organs or peritoneum
-
a
Esophagus, stomach, small intestine, colon, or rectum
-
b
Pancreas
-
c
Other ill-defined digestive organs;
-
a
-
2
Malignant neoplasms of respiratory or intrathoracic organs, excluding nasal cavities and accessory sinuses
-
a
Trachea, bronchus, or lung;
-
a
-
3
Malignant neoplasm of the ovary;
-
4
Non-malignant respiratory diseases, excluding upper respiratory tract infections
-
a
Chronic obstructive pulmonary disease (COPD) or allied conditions
-
b
Asbestosis
-
c
Other diseases of the respiratory system.
-
a
We also examined mesothelioma deaths. The ICD-9 system did not include a code specific for mesothelioma; therefore, we do not report SMRs for mesothelioma prior to 1999. Actual mesothelioma deaths that occurred between 1999 and 2011 were identified using the ICD-10 code C45. Table 1 lists the ICD-9 and ICD-10 codes that were used to retrieve the category-specific deaths mentioned above.
The translation of the above-mentioned ICD-9 to the appropriate ICD-10 codes was made using the World Health Organization (WHO) International Classification of Diseases Translator13 and the NIOSH-recommended ICD-9 and -10 codes for asbestos-related mortality.14 Discrepancies in our final list after comparing the WHO translation and the NIOSH list of codes were reviewed and deemed appropriate by staff clinicians with expertise in asbestos-related mortality and disease classification. US comparison mortality data were retrieved from the Centers for Disease Control and Prevention, National Center for Health Statistics Compressed Mortality File.15
Georeferencing of Decedents
In order to calculate the most accurate SMRs, we were limited by the available census data for the rural area around Libby. Detailed census data were available as early as 1980 by the County Division level within Lincoln County, and the Libby County Division was selected as our study area boundary for inclusion of decedents (Figure 1).

Map of geographic boundary (Libby County Division, 1980) used to assess mortality rates in Lincoln County, Montana.
The decedent’s last place of residence as listed on their death certificate was geocoded before analyzing SMRs to confirm inclusion in the Libby County Division. Using the Libby County Division allowed us to exclude other cities in Lincoln County that were unlikely to have been impacted by asbestos exposure. The use of the county division offered a more focused method for analyzing mortality in Libby, because many residents identify their place of residence as Libby even though they live well outside city limits.
Decedents’ residential addresses were geocoded using two different geocoders: ESRI's North American Address Locator and Centrus Desktop 5.0 (Group 1 Software, A Pitney-Bowes Company, Lanham, MD, USA). For addresses where the locations returned from the two geocoders differed or where they were matched to the ZIP code level, additional sources were consulted to find a location. The supplementary sources included Google Maps and tax parcel data from Lincoln County, MT.
For decedents whose address was listed as a P.O. Box or Rural Route number, the local postmaster was contacted to provide a physical street address. For 66 decedents, the last place of residence was recorded as the Libby Care Center, a local elder care facility that houses residents from Libby and the surrounding communities. To identify whether decedents from the Care Center lived in Libby before their admission to the center, we researched admission records for the individual’s address prior to their admission. The decedent’s prior address was then geocoded. Decedents who were not Libby residents prior to moving into the Libby Care Center were excluded from the study. There were 10 decedents from the Libby Care Center for whom no previous address could be found; for these cases, the Libby Care Center was geocoded as their residential address.
Baseline Population Estimates
The population data in the study are from the US Census Bureau's decennial census of 1980, 1990, 2000, and 2010. The census data for the Libby County Division were obtained from two different sources. Census data for 1980, 1990, and 2000 were obtained from the Minnesota Population Center's National Historical Geographic Information System: Version 2.0. Minneapolis, MN: University of Minnesota 2011. The National Historical Geographic Information website (https://www.nhgis.org/) was used to query and download the data. Census data for 2010 were obtained from the spatial data repository maintained in ATSDR's GIS program.
The 1980 boundaries we used were the Census County Divisions. In 1990, the boundaries changed very slightly when the area was divided into three census tracts. The tract boundaries remained unchanged for the subsequent censuses (2000, 2010). The slight change in the census boundaries has no effect on our study, because the boundary differences occur in unpopulated areas.
Population data were not available at the Lincoln County Division level for non-census years. For those years, we applied non-linear interpolation, using Lincoln County data to derive Libby Division postcensal estimates by year, sex, and age group, and then adjusted these to create Libby Division intercensal estimates. Specifically, we used Lincoln County intercensal estimates to create year-to-year inflation factors, and then applied these to Division census counts to create Division postcensal estimates. We then used the Das Gupta method16 to produce intercensal estimates that reconciled the postcensal estimates with census counts. This method of interpolation used county data to create initial estimates, then updated them to account for Census counts. The resulting estimates mirror the year-to-year changes observed for the county and are consistent with the County Division census counts prior to and after the estimate years.
Demographics
The following demographic data were retrieved from decedents’ death certificates: sex, age, and race (White vs Non-White). Because death certificates do not contain consistent information on risk factors or confounders like occupational history, family medical history, or smoking, these factors were not controlled for in the analysis. To investigate occupational history associated with potential asbestos exposure, we compared our decedent population with ATSDR’s list of former W.R. Grace employees, using Social Security number or first name, last name, and date-of-birth combined.17
Standardized Mortality Ratios
To quantitatively assess asbestos-related mortality in Libby, the number of observed cases for each cause of death was converted to ratios. An SMR represents the ratio, with a null value of 1, of the number of observed deaths to the expected number of deaths for a referent population standardized to eliminate effects due to age differences. The population of the United States was used as a reference population in calculating the expected mortality rates for SMRs. The comparison population was limited to the White population to better reflect the racial make-up of the Libby decedents (Table 2). Sex-specific 33-year (1979–2011) SMRs and corresponding 95% confidence intervals (CIs) were generated for each cause-of-death category and subcategory using the decedent’s underlying cause of death. SMRs for each category and subcategory were also calculated excluding decedents who matched our list of former W.R. Grace employees. SMRs and corresponding CIs for mesothelioma deaths were only calculated for 1999–2011.
RESULTS
Georeferencing
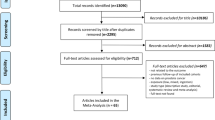
We obtained 767 original death certificate records from MDPHHS. Sixteen records were excluded because they lacked address information. Fifteen records were excluded because they had addresses in cities other than Libby after address history research. Of the remaining 736 records, 695 (94.4%) were matched to specific coordinates using the street address and 41 records were matched to a ZIP code centroid. Those matched on zip code centroid were excluded from the analysis because of the locational uncertainty. One record that was geocoded down to the street level fell outside of our study boundary. Six hundred and ninety-four decedents were successfully geocoded to an address inside our study area boundary and used in the study.
Demographics
There were more male decedents than female (58.6% male vs 41.4% female). The majority of decedents were age 65 or older at the time of death (Table 2). The study population was primarily White (98.7%). Eighty-seven decedents, 85 men and 2 women, were matched to the W.R. Grace employee list.
Asbestos-Related Underlying Cause Mortality Statistics
There were 152 Libby decedents (80 males, 72 females) with malignant neoplasm of the digestive organs as their underlying cause of death. The 33-year SMR was statistically significantly decreased for both sexes combined and for males only before and after controlling for past W.R. Grace employment. The majority of cases (103, 67.8%) were attributed to the subgroup malignant neoplasm of esophagus, stomach, small intestine, colon, and rectum, and the SMR was statistically significantly decreased in this subcategory for males only after excluding past W.R. Grace employees. The SMR for the subcategory malignant neoplasm of the pancreas was significantly decreased for males before and after controlling for past W. R. Grace employment (Supplementary Tables).
There were 232 decedents (152 males, 80 females) with a malignant neoplasm of the respiratory and intrathoracic organs listed as their underlying cause of death. The 33-year SMR was not statistically elevated (SMR=1.03, CI=0.90–1.03). Results remained insignificant when controlling for former W.R. Grace employment (SMR=0.91, CI=0.79–1.04). The subcategory “malignant neoplasm of trachea, bronchus, or lung” contained all but 5 of the 232 decedents (97.8%) and SMRs were statistically insignificant in this subgroup.
There were 19 decedents with a malignant neoplasm of the ovary listed as their underlying cause of death. No statistically significant results were found for rates of malignant neoplasm of the ovary. The number of cases did not change after controlling for past W.R. Grace employment.
There were 286 cases (171 males, 115 females) with a non-malignant respiratory disease listed as their underlying cause of death. Before controlling for past employment, SMRs were statistically significantly elevated for both sexes combined (SMR=1.45, CI=1.28–1.63), and separately for males (SMR=1.51, CI=1.30–1.76) and females (SMR=1.36, CI=1.12–1.63) (Figure 2). After excluding workers, SMRs were statistically significant for both sexes combined (SMR=1.21, CI=1.06–1.37) and for females (SMR=1.35, CI=1.11–1.62) but not for males (SMR=1.11, CI=0.92–1.32). The majority (187, 65.4%) of non-malignant respiratory cases identified were people with COPD listed as their underlying cause of death (99 males, 88 females). COPD SMRs were statistically significant for both sexes combined before controlling for past employment and for females before and after excluding W.R. Grace workers from the analysis (Table 3). Male SMRs were not significantly elevated.

Thirty-three-year SMRs and 95% confidence intervals for non-malignant respiratory disease using US data for comparison.
The most highly elevated SMRs in the “non-malignant respiratory diseases” category were observed among persons with asbestosis listed as their underlying cause of death (59 cases, 45 males and 14 females). When compared with the US population, statistically significant results were found for both sexes combined and for males and females separately, before and after controlling for past employment (Table 4). When W.R. Grace workers were excluded from the analysis, the SMR estimates decreased but remained statistically significant.
Because there was no unique code for mesothelioma before 1999, we looked at SMRs for the ICD-10 period only, 1999–2011. There were five cases (4 male and 1 female) of mesothelioma from 1999 to 2011 (Table 5). SMRs for both sexes combined, males, and females were elevated but not statistically significant before controlling for past employment. All male mesothelioma cases were matched to W.R. Grace employee records, and therefore might have had occupational asbestos exposure. The single female case was not matched to employee records.
DISCUSSION
Interpretation of Results
This study concurs with the findings of ATSDR’s 2002 Health Consultation and shows an increase in potential asbestos-related mortality in the following 13 years, especially for the female population. In 2002, there were no statistically significant SMRs presented for females, except for asbestosis rates in their three largest areas using the US population as comparison.9 In our study, female asbestosis was significantly elevated, as was asbestosis in males. Similarly, we found significantly elevated rates for female COPD and general non-malignant respiratory diseases. Although this study cannot draw conclusions about the exposure pathway, the increase in potential asbestos-related mortality for females, of whom only two were matched to our list of former W.R. Grace workers, suggests that women may have experienced non-occupational asbestos-related exposure.
Further research on individual cases would help identify possible secondary exposure, such as from sharing a home with a former worker. Non-occupational exposures can occur through household contact with employees, ambient levels of asbestos in the environment released from processing of contaminated vermiculite ore, or a variety of other routes.
Although we are not able to accurately calculate SMRs for mesothelioma before 1999 using death certificate data, there were nevertheless known cases during that time period. In the 2002 Health Consultation,9 investigators reported on three mesothelioma cases that were found by a manual search of Libby death certificates coded with the ICD-9 199 code for malignant neoplasm without specification of site. On these records, the cause of death was listed as “mesothelioma” and not “pleural mesothelioma” or “peritoneal mesothelioma.” Without specific information on the death certificate regarding the anatomical location of the mesothelioma, classifying these deaths as ICD-9 199 is appropriate. We were unable to perform the same manual search on national reference populations and could not calculate SMRs for 1979–2011 or 1979–1998 using these mesothelioma cases. The Health Consultation also reported on referent causes of death (breast cancer, prostate cancer, and cerebrovascular disease) to check for temporal changes in mortality reporting and recording for the time period 1979–1998. The authors of the 2002 report found that the SMRs for all of the referent underlying causes were close to one, supporting the validity of their analysis (ATSDR 2002). Therefore, referent causes were not further investigated in this new analysis.
Past studies have investigated the risks associated with exposure to Libby vermiculite and the development of asbestos-related lung and pleural diseases in occupational cohorts and in the general Libby community. One medical testing program examined associations in live subjects between self-reported exposure and pleural or interstitial abnormalities among 7307 persons who had lived, worked, or played in Libby for at least six months prior to 31 December 1990. The results of that study showed that the prevalence of pleural abnormalities increased with an increasing number of exposure pathways, from a prevalence of 6.7% pleural abnormalities in those reporting no apparent exposure in their interviews, up to a prevalence of 34.6% for those who reported 12 pathways. The factors most strongly associated with pleural abnormalities were former W.R. Grace employment, age, sharing a home with a W.R. Grace worker, and being male.6 Another study looked at occupational respiratory disease mortality through 2001 among former Libby vermiculite miners, millers, and processors comparing 1672 workers to the White men in the United States population. The author of that study found elevated SMRs for asbestosis (SMR=165.8, 95% CI: 103.9–251.1), lung cancer (SMR=1.7, 95% CI: 1.4–2.1), cancer of the pleura (SMR=23.3, 95% CI: 6.3–59.5), and mesothelioma (SMR=15.1, 95% CI: 1.8–54.4) among their study cohort.18 The findings on the health status of living Libby residents support our findings, as do the elevated SMRs in the worker cohort mortality study by Sullivan, but neither study examined the community mortality experience for the broader Libby community.
Other studies have been performed on cohorts outside of Libby investigating the health effects of occupational and non-occupational exposure to Libby vermiculite at processing plants around the United States.7 One particular non-occupational study, the Northeast Minneapolis Community Vermiculite Investigation, found an association between the prevalence of pleural abnormalities and estimates of environmental exposure to asbestos fibers attributed to processing Libby vermiculite, suggesting that non-occupational community exposure to asbestos fibers from the processing of Libby vermiculite produced measurable effects.19
The results of our study also raise some questions about the effects of sex on susceptibility to non-malignant respiratory disease. The non-worker asbestosis results were much higher for females than males, even though they both represent non-occupational community exposure. The expected rates for males are 27 times higher than females (0.55 and 0.02, respectively), so that may be driving some of the gender difference in the magnitude of the SMRs. In addition, there has also been research on the difference of susceptibility to fiber-induced health effects based on sex, although the majority has focused on mesothelioma and there is no published data available on the possible role of gender in the development of asbestos-related non-malignant disorders.20 The non-worker female COPD SMRs were also elevated while non-worker male COPD SMRs were not. This is a new finding since the 2002 Health Consultation by ATSDR, which did not report on any sex-specific SMR elevations for COPD. Some factors related to sex outside of occupational history that may influence COPD risks or outcomes are phenotypic differences in the expression of COPD or sex differences in comorbidities.21
Limitations
The main limitations of this study are: the possible effects of exposure misclassification, potential diagnostic bias, a lack of information on smoking history, and general issues with death certificates as a data source in assessing trends in mortality. Residential address verification was performed on select decedents: those from the Libby Care Center or who had a P.O. Box on their death certificate. Given the large number of decedents who met these criteria, address verification was necessary to determine whether these decedents were actually Libby residents and where they resided within Libby. Although this eliminated some bias, the same level of address verification could not be performed on all decedents. In addition, we were unable to conduct a full residential history on each decedent. Therefore, it is possible that one’s last place of residence may not accurately provide a real representation of past exposure. We are unable to account for the effects of population migration, but according to the US Census, the Lincoln county population increased by 2169 or 12% between 1990 and 2010. This population growth still does not diminish the effect of out-migration. Because we only use address at time of death, our group of decedents includes some people who did not live in Libby for the requisite latency period, and it does not include former residents who moved out of Libby for jobs, retirement, or medical treatment. Thus, the SMRs are likely an underestimate of the true effect of exposure as a resident of Libby, given that the baseline population increased over time. It is possible that, if new residents arrive with little or no asbestos exposure and longer term residents with greater exposure depart, these circumstances could cause an underestimate of the disease–exposure relationship. However, even with this effect, we still found significantly elevated SMRs.
Awareness of asbestos contamination of Libby vermiculite and the health effects attributed to asbestos exposure has greatly increased in recent decades. As a result, it is possible that medical certifiers in Libby are more likely to report asbestos-related mortality as a cause of death on a decedent’s death certificate than examiners in other parts of the country, resulting in a diagnostic bias. Conversely, improved medical care in the last 10 years, owing to increased funding and access to care, as well as patient and provider education, may have slowed mortality since the previous study.
Although death certificates contain important information, they are known to include inaccuracies and do not contain consistent information on risk factors or confounders like occupational history, family medical history, or smoking.22 In order to be consistent about case definition and comparison case ascertainment, we did not pursue any additional information to validate specific causes of death as they were reported on the death certificates obtained from MDPHHS. Asbestos exposure and smoking have both been associated with outcomes such as lung cancer, non-malignant respiratory diseases, and cardiovascular diseases. Adult smoking prevalence in Montana in 2010 was reported at 18.8% (19.7% for male, 17.9% for females) compared with a rate of 17.3% nationwide (18.5% for males, 15.8% for females), according to the CDC’s Behavioral Risk Factor Surveillance System.23 There were also coding issues that resulted from the change in how deaths were coded before and after 1999. For the first 20 years, causes of death were classified with ICD-9 codes and the most recent 13 years used ICD-10 codes. Although much attention was paid to the “translation” of the pertinent causes of death, there are bound to be complications with this process.
CONCLUSIONS
Elevated asbestos-related mortality rates were observed among males and females for non-malignant respiratory diseases. Results for asbestosis were particularly high for both sexes, even after controlling for W.R. Grace employment history. These results suggest asbestos-related effects may be experienced by others in the general population besides former vermiculite workers. Additional research on decedents may help determine whether SMRs remain elevated after controlling for secondary exposure to asbestos-contaminated dust brought home on a vermiculite worker’s clothes. Future case studies may provide information on whether decedents had other occupational asbestos exposure not related to vermiculite mining (e.g., military history, logging related work, or auto repair).
References
Bandli BR, Gunter ME . A review of scientific literature examining the mining history, geology, mineralogy, and amphibole asbestos health effects of the Rainy Creek Igneous Complex, Libby, Montana, USA. Inhal Toxicol 2006; 18: 949–962.
Meeker GPAMB Meeker GPAMB Brownfield IK Meeker GPAMB Lowers HA Meeker GPAMB Sutley SJ Meeker GPAMB Hoefen TM Meeker GPAMB Vance JS . The composition and morphology of amphiboles from the Rainy Creek Complex Near Libby, Montana. Am Mineral 2003; 88: 1955–1969.
McDonald JC, Harris J, Armstrong B . Mortality in a cohort of vermiculite miners exposed to fibrous amphibole in Libby, MT. Occu Environ Med 2004; 61: 363–366.
McDonald JC, McDonald AD, Armstrong B, Sebastien P . Cohort study of mortality of vermiculite miners exposed to tremolite. Br J Ind Med 1986; 43: 436–444.
Whitehouse AC, Black CB, Heppe MS, Ruckdeschel J, Levin SM . Environmental exposure to Libby asbestos and mesotheliomas. Am J Ind Med 2008; 51: 877–880.
Peipins LA, Lewin M, Campolucci S, Lybarger JA, Miller A, Middleton D et al. Radiographic abnormalities and exposure to asbestos-contaminated vermiculite in the community of Libby, Montana, USA. Environ Health Perspect 2003; 111: 1753–1759.
Horton K, Kapil V, Larson T, Murarov O, Melnikova N, Anderson BA . Review of the Federal Government's health activities in response to asbestos-contaminated ore found in Libby, Montana. Inhal Toxicol 2006; 18: 925–940.
Antao VC, Larson TC, Horton DK . Libby vermiculite exposure and risk of developing asbestos-related lung and pleural diseases. Curr Opin Pulm Med 2012; 18: 161–167.
ATSDR Mortality in Libby, Montana 1979-1998 Libby Asbestos Site, Libby, Lincoln County, Montana 2002. Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA.
Cooke W . Fibrosis of the lungs due to the inhalation of asbestos dust. Br Med J 1924; 2: 147.
Selikoff IJ, Hammond EC, Seidman H . Mortality experience of insulation workers in the United States and Canada, 1943-1976. Ann NY Acad Sci 1979; 330: 91–116.
Straif K, Benbrahim-Tallaa L, Baan R, Grosse Y, Secretan B, El Ghissassi F et al. A review of human carcinogens? Part C: metals, arsenic, dusts, and fibres. Lancet Oncol 2009; 10: 453–454.
World Health Organization. Translator ICD9 to ICD10, 1996.
National Institute of Occupational Safety and Health. Life Table Analysis System Table. 04/18/2008 ed 2008.
CDC Wonder compressed mortality file. CDC WONDER On-line Database 2014. National Center for Health Statistics.
U.S. Census Bureau. Methodology. http://www.census.gov/popest/methodology/intercensal_nat_meth.pdf (accessed on 24 October 2014).
Larson T, Antao V, Bove F . Vermiculite worker mortality: estimated effects of occupational exposure to Libby amphibole. J Occup Environ Med 2010; 52: 555–560.
Sullivan P . Vermiculite, respiratory disease, and asbestos exposure in Libby, Montana: update of a cohort mortality study. Environ Health Perspect 2007; 115: 579–585.
Alexander BH, Raleigh KK, Johnson J, Mandel JH, Adgate JL, Ramachandran G et al. Radiographic evidence of nonoccupational asbestos exposure from processing Libby vermiculite in Minneapolis, Minnesota. Environ Health Perspect 2012; 120: 44–49.
Below JE, Cox NJ, Fukagawa NK, Hirvonen A, Testa JR . Factors that impact susceptibility to fiber-induced health effects. J Toxicol Environ Health B Crit Rev 2011; 14: 246–266.
Aryal S, Diaz-Guzman E, Mannino DM . Influence of sex on chronic obstructive pulmonary disease risk and treatment outcomes. Int J Chron Obstruct Pulmon Dis 2014; 9: 1145–1154.
Selikoff IJ . Use of death certificates in epidemiological studies, including occupational hazards: discordance with clinical and autopsy findings. Am J Ind Med 1992; 22: 469–480.
Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System. 2012.
Acknowledgements
Bruce Schwartz and staff at Vital Statistics MDPHHS for assistance with case ascertainment; Dan Middleton, Vinicius Antao, Theodore Larson from ATSDR for their assistance with asbestos-related diseases and cause of mortality coding; Staff at the Libby Care Center and Bruce Moog, Postmaster in Libby, MT for their assistance with address verification.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Journal of Exposure Science and Environmental Epidemiology website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Naik, S., Lewin, M., Young, R. et al. Mortality from asbestos-associated disease in Libby, Montana 1979–2011. J Expo Sci Environ Epidemiol 27, 207–213 (2017). https://doi.org/10.1038/jes.2016.18
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jes.2016.18
