
Abstract
An oscillometric device is recommended for blood pressure (BP) measurement in atrial fibrillation (AF), but there is still controversy concerning its accuracy. Therefore, evaluation of BP values in AF patients remains a challenge. This study included 251 patients with AF and 154 participants with sinus rhythm (SR). Pulse rate (PR) and BP were measured using an oscillometric device three times. The differences between the highest and lowest PR and the systolic and diastolic BP (SBP and DBP) were calculated as ΔPR, ΔSBP and ΔDBP, respectively. AF patients were stratified with respect to ΔPR in 0–5, 6–10, 11–15 and >15 subgroups. The AF group had a greater ΔPR (12.1±8.6 vs. 4.10±3.21 b.p.m., P<0.001), ΔSBP and ΔDBP than the SR group at similar SBP and DBP. A positive correlation existed between ΔPR and ΔSBP (r=0.255, P<0.001) in AF patients, but no correlation was found in SR subjects. Meanwhile, the ΔSBP in the 0–5 and 6–10 subgroups (9.58±5.61 and 10.67±6.77 vs. 8.45±5.25 mm Hg, nonsignificant) was similar to the SR group, whereas ΔSBP in the 11–15 and >15 subgroups was significantly greater than the SR group. Regardless of ΔPR, the ΔDBP in the AF group was significantly greater than that of the SR group. The AF patients who exhibited greater variability in their PR also had a greater variability in their SBP readings. The SBP measurement for AF patients is accurate as the measurement for patients with SR if the ΔPR is of 0–10 b.p.m. in AF.
Similar content being viewed by others

Introduction
Hypertension and atrial fibrillation (AF) often coexist, and both are strong risk factors for stroke. In addition, many medications used to treat AF also may induce hypotension that is associated with an increase in all-cause mortality or adverse events.1, 2, 3 Therefore, blood pressure (BP) control is important in AF patients. However, measuring BP in AF patients is difficult and uncertain, even when using the auscultatory method, because there is a high variability of BP that is induced by an irregular ventricular rate and stroke volume.4, 5
Previously, an oscillometric device was not considered suitable for BP measurement in AF patients. However, some studies recently showed that the oscillometric method could detect the systolic BP (SBP) in a sufficiently accurate manner compared with auscultatory sphygmomanometry.6 Pagonas et al.7 suggested that AF did not significantly affect the accuracy of oscillometric measurements compared with intra-arterial BP if three measurements were performed. Therefore, some guidelines recommend the oscillometric BP method in AF patients if repeated measurements were performed.8, 9
Because an oscillometric BP measurement is based on the assumption that the cardiac rhythm is regular, the controversy about its accuracy in AF is ongoing. In clinical practice, a large intraindividual variability between three BP measurements is often observed in patients with AF compared with those with sinus rhythm (SR).10, 11
Currently, the method to evaluate BP values using the oscillometric method in AF patients is a challenge for clinicians. Because the irregularity of the ventricular rate varies in patients with AF, and because the variability of three pulse rate (PR) measurements may reflect the irregularity of the ventricular rate to some extent, we suspect that the variability of three PR readings may be associated with the variability of three BP readings in AF patients. However, the variability of three BP readings in AF patients with lower PR variability may be similar to the BP readings in SR subjects, and these BP readings may be accepted in a clinical setting. The aim of this study was to test the above-mentioned hypothesis and to identify a cutoff point for the PR variability with which the variability of three BP readings was similar to readings in patients with a SR. If this hypothesis is true, doctors and patients may better evaluate the clinical value of the BP reading from an oscillometric device by referencing the PR variability.
Methods
The proposal and consent procedures of this study were approved by the Ethics Committee of the Second Affiliated Hospital of Nanchang University. All patients provided verbal informed consent.
This study included 251 outpatients with permanent AF and 154 outpatients with SR from March to July of 2015. At the time of BP measurements, all subjects received an ECG examination to identify AF or SR. In addition, information about age, sex, body mass index, smoking status, diabetes mellitus, cardiovascular disease and the use of antihypertensive or heart rate (HR)-control treatments was collected.
The exclusion criteria were as follows: acute myocardial infarction, congenital heart disease, acute heart failure, syncope, hemiplegia and pulseless disease. In patients with SR, subjects with arrhythmias were also excluded.
An automatic BP device using an oscillometric method (OMRON BP HEM-7200, Omron Co., Ltd, Dalian, China) was used in this study. The cuff was placed on the middle of right upper arm. After a 10-min rest in a sitting position, the PR and BP were taken at a 1-min interval three times, and the averages were calculated as the final BP and PR values. To evaluate the variability of the PR, ΔSBP and ΔDBP, the difference between the highest and lowest values of three readings for each parameter was calculated. Based on ΔPR, AF patients were stratified into four subgroups: ΔPR 0–5, ΔPR 6–10, ΔPR 11–15 and ΔPR >15.
Statistical analysis
The data were entered using Excel 2007 and analyzed using SPSS19.0 (SPSS Company, Chicago, IL, USA). Continuous variables were expressed as mean±s.d. The χ2 test and two independent sample t-tests were used for the statistical analysis. Linear correlation analysis was performed to examine the correlation of mean ΔBP with ΔPR. A P-value of <0.05 was considered statistically significant.
Results
The baseline characteristics of participants with sinus rhythm and AF are shown in Table 1. The SBP, diastolic BP (DBP), body mass index, the percentage of each gender and smokers, and the prevalence of diabetes mellitus and hypertension were similar between the SR and AF groups. However, 71.1% of AF patients received β-blockers, and this value was only 3.2% in SR subjects. In addition, more AF patients used aspirin and warfarin. The use of other antihypertensive drugs was similar between the AF and SR groups.
The levels of SBP (120.8±20.6 vs. 122.6±11.4 mm Hg, nonsignificant) and DBP (71.3±11.2 vs. 71.7±10.3 mm Hg, nonsignificant) were similar between the AF and SR groups, but ΔSBP (11.45±7.75 vs. 8.45±5.25 mm Hg, P<0.001), ΔDBP (8.48±6.75 vs. 5.27±5.77 mm Hg, P<0.001) and ΔPR (12.1±8.6 vs. 4.10±3.21 b.p.m., P<0.001) were significantly greater in the AF group than the SR group (Figure 1).

Comparison of the blood pressure (BP) and pulse rate (PR) parameters between the atrial fibrillation (AF) and sinus rhythm (SR) groups. DBP, diastolic blood pressure; SBP, systolic blood pressure.
To exclude a possible bias from the greater age in the AF group, we analyzed the data after excluding the AF patients who were more than 70 years old. When the mean age was similar between the two groups, the AF group still had a significantly greater ΔSBP and ΔPR than the SR group (Table 2).
In this study, only 8 (5.2%) patients with SR had a ΔPR >10 b.p.m., but this value was 48.6% in AF patients.
These results indicate that the patients with AF had a greater PR, SBP and DBP variation among three BP measurements.
Furthermore, the ΔSBP of the ΔPR 0–5 or ΔPR 6–10 AF subgroup was similar to that of the SR group (9.58±5.61 and 10.67±6.77 vs. 8.45±5.25 mm Hg, nonsignificant), but the ΔSBP of the ΔPR 11–15 or ΔPR >15 AF subgroup was significantly greater than that of the SR group. The ΔDBPs of the four AF subgroups were significantly greater than that of the SR group (Table 3).
A linear correlation analysis showed a positive correlation between ΔPR and ΔSBP (r=0.255, P<0.001) or ΔDBP (r=0.307, P<0.001) in AF patients. However, in SR patients, no correlation was found between ΔPR and ΔSBP, whereas a positive correlation existed between ΔPR and ΔDBP (r=0.211, P=0.009; Figure 2).

Correlation between ΔPR and ΔBP in the atrial fibrillation (AF) and sinus rhythm (SR) patients. BP, blood pressure; DBP, diastolic blood pressure; PR, pulse rate; SBP, systolic blood pressure.
Discussion
In this study, an index, ΔPR, was used to express the variability of the PR among three BP measurements. It is well known that in patients with sinus rhythm, when the PR is measured using an oscillometric device, it can accurately represent the ventricular rate (HR); thus, the ΔPR in this study is mainly dependent on the HR variation during the period of the three BP measurements. Conversely, the PR measured using an oscillometric device is less than the HR because of the pulse deficit in AF patients. In addition, the variation of the HR in the period of the three BP measurements was large in the AF patients. Therefore, the ΔPR may be a comprehensive result of the irregular HR during BP measurement and during the period in which the three BP measurements were taken.
First, the present study demonstrated that the mean PR was higher in the AF group than in the SR group, and the mean ΔPR was significantly greater in the AF group than in the SR group (12.1±8.6 vs. 4.1±3.2 b.p.m.). In addition, in this study, only 8 patients with SR had a ΔPR >10 b.p.m. (5.2%), but this value was 48.6% for the AF patients. These results indicated a greater PR variation in the three BP measurements in the AF group.
Second, the present study showed that ΔPR was variable in AF patients, with a ΔPR of 0–10 b.p.m. in 51.4% of patients and more than 10 b.p.m. in 48.6% of patients. These results indicate that the irregularity of the ventricular rate was different among the AF patients. In addition, patients with a higher PR had greater ΔPR values. These results may indicate that the rapid HR may induce a greater ΔPR.
Third, the present study showed a positive correlation between ΔPR and ΔSBP in AF patients, whereas no correlation was found between ΔPR and ΔSBP in SR patients. These results imply that the PR variability affects the measurement of SBP using oscillometric devices in AF patients. Because the ΔSBP in the AF patients with a ΔPR of 0–10 b.p.m. was close to the ΔSBP in the SR patients, we suggest that when the ΔPR was 0–10 b.p.m., the SBP measurement in AF patients may be as accurate as in patients with SR. Therefore, the SBP in 51.4% of the AF patients (ΔPR of 0–10 b.p.m.) in this study may be clinically acceptable. If the ΔSBP in the AF patients with a ΔPR of >10 b.p.m., especially if ΔPR was >15 b.p.m., was significantly greater than ΔSBP in the SR patients, the SBP reading in these patients may be not as accurate as in SR patients.
The reason for this result is unclear. We suggest that the basic theory of oscillometric BP measurement is related. Unlike auscultatory BP measurements, oscillometric measurements calculate the BP by measuring a series of small pressure pulses while the cuff pressure is decreased from above the SBP to the DBP. In other words, the determination of the SBP and the DBP is on an envelope curve that is created based on the relationship between the oscillometric pulse amplitude and the cuff pressure. Currently, the algorithm used to calculate the SBP and the DBP is dependent on the envelope curve from the regular heart rhythm. Although most oscillometric BP devices are designed to accommodate some level of HR variation during the BP measurement cycle, significant HR variability can create a situation where the reference BP is difficult to determine. A common example occurs in AF patients. In AF patients, especially those with more irregularity (indicated by a greater ΔPR), the envelope curve may vary far from the patients with SR; thus, the BP measurement may be more inaccurate. When the rhythm of ventricular beats changes more obviously, the BP readings were more variable among the three measurements.12, 13
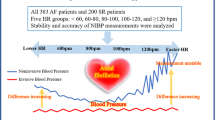
Previously, Giantin et al.14 indicated that the BP values of ambulatory blood pressure monitoring in stable AF patients (HR 60–100 b.p.m.) were similar to those patients with SR, whereas the BP values in very unstable AF (HR over 100 b.p.m.) were not. This study found that AF patients with a HR over 100 b.p.m. measure using ECG often have a greater ΔPR. The finding that a greater ΔPR induces a less accurate SBP measurement in the present study is concomitant with the study of Giantin et al.14
Fourth, our results demonstrate that the greater ΔSBP and ΔPR in the AF group were not dependent on the greater age in the AF group. When the data from the AF patients >70 years of age were excluded, the AF group still had a significantly greater ΔSBP and ΔPR than the SR group when these two groups had similar mean ages.
Finally, our results show that, regardless of ΔPR, ΔDBP in the AF group was significantly greater than in the SR group. Meanwhile, there was a stronger positive correlation between ΔPR and ΔDBP (r=0.307, P<0.001) in AF patients compared with SR patients (r=0.211, P=0.009). These findings mean that DBP determined using the oscillometric method is not accurate as in SR patients. Previously, the study of Pagonas and Westhoff15 also showed a greater DBP bias (between the noninvasive and intra-arterial measurements) in AF patients compared with SR patients (8.6±9.8 vs. −3.9±10.4 mm Hg), whereas the SBP bias was similar. Because a positive correlation existed between ΔPR and ΔDBP but not between ΔPR and ΔSBP in the SR patients, we consider that the DBP measured using the oscillometric device may be easily influenced by the variation in HR.
Clinical implications
Although the mean SBP value of the three measurements measured using the oscillometric device has been suggested by some studies to be clinically acceptable,7, 15, 16 our results showed quite a large variability in SBP measurements in AF patients. The present study provides useful information for doctors to better evaluate the BP when using an oscillometric device: when the ΔPR of three BP measurements is 0–10 b.p.m., the SBP reading may be as accurate as the SBP reading in SR patients, and it is clinically acceptable. However, when the ΔPR is >10 b.p.m., the SBP reading may not be reliable, and more BP measurements are needed. However, the DBP reading is less reliable than the SBP reading if ΔDBP was significantly greater than that of the SR group, regardless of ΔPR.
Limitations
In this study, the BP difference among three oscillometric measurements in SR was used as a reference to confirm our discovery that a greater ΔPR is associated with a less accurate BP measurement in AF patients. Therefore, a study using intra-arterial BP measurement is needed.
In addition, the treatments were quite different between the SR and AF groups. This difference may affect the BP measurement but could not induce the greater ΔSBP and ΔPR in the AF group. To identify this point, more research is needed.
Conclusion
There is a positive relationship between the variations in the pulse rate and the SBP measured using an oscillometric BP device. The AF patients who exhibit a greater variability in their pulse rate will also have a greater variability in their BP readings. The SBP measurement in AF patients may be considered as accurate as the SBP measurement in SR patients if ΔPR is 0–10 b.p.m.
References
Badheka AO, Patel NJ, Grover PM, Shah N, Patel N, Singh V, Deshmukh AJ, Mehta K, Chothani A, Savani GT, Arora S, Rathod A, Marzouka GR, Lafferty J, Mehta JL, Mitrani RD . Optimal blood pressure in patients with atrial fibrillation (from the AFFIRM Trial). Am J Cardiol 2014; 114: 727–736.
Carlsson AC, Wändell P, Sundquist K, Johansson SE, Sundquist J . Effects of prescribed antihypertensives and other cardiovascular drugs on mortality in patients with atrial fibrillation and hypertension: a cohort study from Sweden. Hypertens Res 2014; 37: 553–559.
Jong GP, Chen HY, Li SY, Liou YS . Long-term effect of antihypertensive drugs on the risk of new-onset atrial fibrillation: a longitudinal cohort study. Hypertens Res 2014; 37: 950–953.
Lip GY, Zarifis J, Beevers M, Beevers DG . Ambulatory blood pressure monitoring in atrial fibrillation. Am J Cardiol 1996; 78: 350–353.
Jani B, Bulpitt CJ, Rajkumar C . Blood pressure measurement in patients with rate controlled atrial fibrillation using mercury sphygmomanometer and Omron HEM-750CP deice in the clinic setting. J Hum Hypertens 2006; 20: 543–545.
Stergiou GS, Kollias A, Destounis A, Tzamouranis D . Automated blood pressure measurement in atrial fibrillation: a systematic review and meta-analysis. J Hypertens 2012; 30: 2074–2082.
Pagonas N, Schmidt S, Eysel J, Compton F, Hoffmann C, Seibert F, Hipert J, Tschope C, Zidek W, Westhoff TH . Impact of atrial fibrillation on the accuracy of oscillometric blood pressure monitoring. Hypertension 2013; 62: 579–584.
Kollias A, Stergiou GS . Automated measurement of office, home and ambulatory blood pressure in atrial fibrillation. Clin Exp Pharmacol Physiol 2014; 41: 9–15.
Maselli M, Giantin V, Corrado D, Franchin A, Attanasio F, Pengo V, Tramontano A, De Toni P, Perissinotto E, Manzato E . Reliability of oscillometric blood pressure monitoring in atrial fibrillation patients admitted for electric cardioversion. J Clin Hypertens (Greenwich) 2015; 17: 558–564.
Stergiou GS, Kollias A, Karpettas N . Does atrial fibrillation affect the automated oscillometric blood pressure measurement? Hypertension 2013; 62: e37.
Myers MG, Stergiou GS . Should oscillometric blood pressure monitors be used in patients with atrial fibrillation? J Clin Hypertens (Greenwich) 2015; 17: 565–566.
Alpert B, Quinn D, Gallick D . Oscillometric blood pressure: a review for clinicians. Jo Am Soc Hypertens 2014; 8: 930–938.
Raamat R, Talts J, Jagomägi K, Kivastik J . Accuracy of some algorithms to determine the oscillometric mean arterial pressure: a theoretical study. Blood Press Monit 2013; 18: 50–56.
Giantin V, Perissinotto E, Franchin A, Baccaglini K, Attanasio F, Maselli M, Grosso G, Luisa Corradin M, Tramontano A, Manzato E . Ambulatory blood pressure monitoring in elderly patients with chronic atrial fibrillation: is it absolutely contraindicated or a useful tool in clinical practice and research? Hypertens Res 2013; 36: 889–894.
Pagonas N, Westhoff TH . Response to "Does atrial fibrillation affect the automated oscillometric blood pressure measurement"? Hypertension 2013; 62: e38.
Stergiou GS, Kollias A, Destounis A, Tzamouranis D . Automated blood pressure measurement in atrial fibrillation: a systematic review and meta-analysis. J Hypertens 2013; 31: 215–216.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (81530013). It was also supported by the National Science and Technology Infrastructure Program No. 2013BAI05B10 and the Ministry of Chinese Education Innovation Team Development Plan (IRT1141).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Wang, Xx., Shuai, W., Hong, K. et al. How to evaluate BP measurements using the oscillometric method in atrial fibrillation: the value of pulse rate variation. Hypertens Res 39, 588–592 (2016). https://doi.org/10.1038/hr.2016.31
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2016.31
