
Abstract
‘Cardiometabolic memory’ has been proposed based on clinical evidence to explain how, even after the cessation of a clinical trial, the superiority of one treatment over the outcome persists. To understand the cardiometabolic memory phenomenon, we performed a systematic review of randomized controlled trials (RCTs) using PubMed in August 2016. The search terms ‘randomized controlled trial’, ‘post-trial follow-up’ and ‘diabetes, hypertension or dyslipidemia’ were used, and articles published after the year 2000 were searched. We judged the memory phenomenon to be positive when the cardiovascular outcome at the end of the post-trial follow-up period in the intervention group was significantly superior even though the favorable control of a risk factor (blood glucose, blood pressure or lipid level) during the trial period was lost after the cessation of the intervention. Among 907 articles retrieved in the initial screening, 21 articles were judged as describing a positive memory phenomenon. Eight, six and seven of the articles concerned diabetes, hypertension and dyslipidemia, respectively. Transient intensive glucose lowering rather easily induced memory for the suppression of diabetic microangiopathies, while memory for the suppression of macroangiopathies tended to be first evident in the post-trial follow-up period. Transient intensive blood pressure lowering was generally effective in the formation of memory for the suppression of cardiovascular events and had an especially strong impact on risk reduction of chronic heart failure. Transient intensive LDL cholesterol lowering clearly had a long-term beneficial effect on risk reduction of cardiovascular events. Our systematic review revealed the clinical relevance of cardiometabolic memory.
Similar content being viewed by others


Introduction
In several randomized controlled clinical trials, the ‘cardiometabolic memory phenomenon’ or ‘legacy effect’ has been proposed based on clinical evidence to show that even after the cessation of the clinical trial, the superiority of one treatment over the outcome persists. This effect has now been highlighted for its medical significance.
The 10-year post-trial follow-up of the UKPDS (United Kingdom Prospective Diabetes Study) revealed that intensive glucose control in type 2 diabetic patients resulted in relative reduction of cardiovascular risks even though the difference in glycemic control was lost between the intensive and standard glucose control groups soon after the trial ended.1 For blood pressure control, the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation)-ON showed a beneficial post-trial ‘memory phenomenon’ in type 2 diabetes.2 The significant difference in blood pressure between the groups receiving active antihypertensive medication and placebo (ΔBPs 5.6/ΔBPd 2.2 mm Hg, P<0.001) that was observed during the randomized ADVANCE trial3 disappeared 6 months after the end of the randomized period (137/74 mm Hg in the active treatment group vs. 136/74 mm Hg in the placebo group). However, the reductions in the risk of death from cardiovascular causes (hazard ratio, 0.82; P=0.03), which were observed in the active treatment group during the randomized period, were still significant at the end of the post-trial follow-up (hazard ratio, 0.88; P=0.04). For lipid management, the result of the 20-year follow-up of the WOSCOPS (West of Scotland Coronary Prevention Study), which showed a legacy benefit of statin treatment, has been published.4 Recently, several articles reporting the results of post-trial follow-up of randomized controlled trials (RCTs) have been published. However, the frequency or clinical relevance of the ‘memory phenomenon’ is not clear.
To more systematically understand the entity of the cardiometabolic memory phenomenon in clinical settings, we performed a systematic review of RCTs that investigated the post-trial effects of the transient intervention for the control of cardiovascular risk factors.
Search strategy for our systematic review
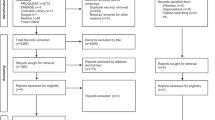
We performed a comprehensive literature search using PubMed in August 2016. For the initial screening, the search terms ‘randomized controlled trial’, ‘post-trial follow-up’, and ‘diabetes, hypertension or dyslipidemia’ were used, and articles published after the year 2000 were searched. For the second screening, titles and abstracts of the retrieved articles were examined by the authors to select RCTs satisfying the following inclusion criteria: (1) written in English, (2) more than 100 participants, (3) longer than 1-year post-trial follow-up period and (4) appropriately focused on the post-trial memory phenomenon of the intervention. Finally, full-text screening of the relevant articles was performed to extract information on patient backgrounds, number of participants, intervention details, control status of the risk factors and cardiovascular outcomes at the end of both the trial period and follow-up period. When plural articles were retrieved for one clinical trial, the articles that were thought to be redundant were omitted.
We judged the memory phenomenon of the transient intervention as positive when the cardiovascular outcome at the end of the post-trial follow- up period in the intervention group was significantly superior even though the favorable control of a risk factor during the trial period was lost after the cessation of the intervention. These risk factors included blood glucose, blood pressure or serum lipid (low-density lipoprotein (LDL)-cholesterol or triglyceride) levels. In contrast, we defined the memory phenomenon as negative when the cardiovascular outcome at the end of the post-trial follow-up period in the intervention group was equivalent to that of the control group. In these cases, the beneficial effects of the transient intervention were not maintained in the follow-up period after the favorable control of a risk factor during the trial period was lost.
In some studies, when a significant suppression of cardiovascular outcomes was observed in the intensive treatment group, a significant reduction in risk factors at the end of the post-trial follow-up period was also detected. In these cases, we described the prolonged effects of the transient intervention as ‘carry-over effects.’ In these situations, the favorable cardiovascular outcomes observed at the end of the follow-up period were considered to be derived from carry-over effects rather than from the memory phenomenon.
Overall findings of our systematic review
In the initial screening, 907 articles were retrieved. A total of 479, 274 and 154 articles were on clinical trials for diabetes, hypertension and dyslipidemia, respectively. In the second screening, 35 articles fulfilled the above-mentioned inclusion criteria, and 15, 10 and 10 articles were on diabetes, hypertension and dyslipidemia, respectively.
After the full-text screening, 21 articles were judged as describing a positive memory phenomenon, as shown in Table 1. Of these, eight,1, 5, 6, 7, 8, 9, 10, 11 six2, 12, 13, 14, 15, 16 and seven4, 17, 18, 19, 20, 21, 22 articles were about diabetes, hypertension and dyslipidemia, respectively. As shown in Table 2, only three articles5, 23, 24 were judged as describing a negative memory phenomenon. In the ACCORDION (Action to Control Cardiovascular Risk in Diabetes Follow-On)-Eye study,5 the memory effect for both glucose and lipid (triglyceride) control was examined. The former was judged as positive and the latter as negative. As shown in Table 3, five articles25, 26, 27, 28, 29 were judged as demonstrating carry-over effects of the transient intervention.
Representatives of cardiometabolic memory-positive trials
The results of our systematic review showed that 21 articles reported a cardiometabolic memory phenomenon in the RCTs on diabetes, hypertension, or dyslipidemia. This systematic review included many RCTs whose observation period was more than 10 years. Therefore, it is suggested that cardiometabolic memory lasts for a long time. Because the clustering of hyperglycemia, hypertension, and dyslipidemia is strongly associated with atherosclerosis,30 cardiometabolic memory produced in the metabolic syndrome had a substantial effect on the clinical course and prognosis of non-communicable diseases.
One of the most representative reports that revealed the memory phenomenon was the long-term follow-up of the DCCT (Diabetes Control and Complications Trial).11 This study showed that intensive therapy for type 1 diabetes for a mean of 6.5 years reduced the risk of any cardiovascular disease by 42 percent (P=0.02) during the 17 years of the post-trial follow-up period.11 In this article, this prolonged effect of early intervention was referred to as ‘metabolic memory.’ Since then, this term has been used widely. Similarly, the term ‘legacy effect’ has been used frequently, as the publication of an article reporting the results from a 10-year post-trial follow-up of the UKPDS.1
Regarding cardiometabolic memory, controversies between blood pressure and blood glucose control have been reported. In the 10-year post-trial follow-up of UKPDS, a legacy effect was shown for blood glucose (UKPDS 80),1 but not blood pressure control (UKPDS 81).23 In contrast, in the ADVANCE-ON study, a beneficial post-trial memory was shown for blood pressure control, but not for blood glucose control.2
Treatment with statins for hypercholesterolemia also demonstrated the existence of a cardiometabolic ‘memory phenomenon.’ The 20-year follow-up of the WOSCOPS revealed that 5-year treatment with pravastatin reduced cardiovascular events over a 20-year period.4 Another statin, simvastatin, was also shown to have a ‘memory phenomenon’ in the 4S (Scandinavian Simvastatin Survival Study),21 namely, a post-trial benefit for lowered coronary mortality.
Occurrence of hypertension and the memory phenomenon
Both cardiovascular risk and the occurrence of hypertension were suggested as targets for the ‘memory phenomenon.’ Prehypertension, which is reported to be associated with abdominal obesity and elevated serum levels of high-sensitivity C-reactive protein,31 is a high risk status for the development of hypertension. The TROPHY (Trial of Preventing Hypertension) study demonstrated that 2-year transient renin-angiotensin system (RAS) inhibition by candesartan in the stage of prehypertension reduced the risk of transition from prehypertension to hypertension, and this beneficial effect was sustained even after the medication was stopped.13 The STAR CAST (Short Treatment with Angiotensin Receptor Candesartan Surveyed by Telemedicine) study we conducted previously demonstrated that 1-year treatment of stage 1 essential hypertension with candesartan postponed the reoccurrence of hypertension compared with treatment with a calcium channel blocker.32 These phenomena were originally shown in hypertension-prone animal models;33, 34, 35, 36 therein, we called it ‘angiotensin block memory,’ and we are currently investigating the molecular basis of this ‘memory phenomenon’.37, 38, 39, 40, 41 In contrast, RAS activation in youth was shown to induce hypertension even after a certain interval after discontinuation of RAS activation.42
Clinical features of the memory phenomenon
Our systematic review revealed the following clinical features of the memory phenomenon:
-
1
Each intervention type, that is, glucose lowering, blood pressure lowering, or LDL cholesterol lowering, possessed unique characters of the memory phenomenon to some extent.
-
2
Transient intensive glucose lowering rather easily induced memory for the suppression of diabetic microangiopathies (ACCORDION-Eye,5 ADVANCE-ON,6 DCCT/EDIC (Epidemiology of Diabetes Interventions and Complications),9 and UKPDS 801), while memory for the suppression of macroangiopathies tended to be first evident in the post-trial follow-up period (DCCT/EDIC,7 VADT (Veterans Affairs Diabetes Trial),8 and UKPDS 801).
-
3
Transient intensive blood pressure lowering was generally effective in the formation of memory for the suppression of cardiovascular events (ADVANCE-ON,2 HOPE-TOO (Heart Outcomes Prevention Evaluation-The Ongoing Outcomes)14) and had an especially strong impact on risk reduction of chronic heart failure (CHF) and CHF-related mortality (MDRD (Modification of Diet in Renal Disease),12 TRACE (Trandolapril Cardiac Evaluation)15).
-
4
Transient intensive LDL-lowering clearly had a long-term beneficial effect on risk reduction of cardiovascular events (WOSCOPS,4 ALLHAT-LLT (Lipid-Lowering Trial component of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial),17 ASCOT-LLA (Lipid-lowering Arm of the Anglo-Scandinavian Cardiac Outcomes Trial),18 ALERT (Assessment of Lescol in Renal Transplantation),20 4S,21 LIPID (Long-term Intervention with Pravastatin in Ischemic Disease)22). In some cases, memory for the suppression of macroangiopathies emerged only in the post-trial follow-up period (ASCOT-LLA19 and ALERT20), which was similar to the memory induced by transient intensive glucose control.
-
5
Lifestyle modification aimed at glucose lowering was very effective in the suppression of new onset diabetes even after the termination of the trial (Finish DPS (Diabetes Prevention Study)25 and the China Da Qing Diabetes Prevention Study27), although the ‘carry-over effects’ described above could explain this phenomenon.
Characteristics of cardiometabolic memory-negative trials
There were only a few studies that denied the existence of the memory phenomenon (Table 2). This trend, however, could be explained by the possibility that negative results in clinical trials are likely to be unpublished. We identified three trials that failed to show the memory phenomenon. All three studies were conducted with two-by-two factorial comparisons. This type of study design sometimes yields incidental uneven grouping or potential interactions between two factors. In UKPDS 81,23 transient intensive blood pressure control failed to show beneficial effects on cardiovascular outcomes in the post-trial period, but there was a difference in HbA1c levels; that is, there was a significantly higher blood glucose level in the intensive blood pressure control group. In the ACCORDION-Eye study,5 fenofibrate treatment failed to reduce the progression of retinopathy in the post-trial period despite obvious improvement in the trial period, however, the proportion of females was significantly lower in the intensive treatment group. The Heart Protection Study (HPS) was also designed as a two-by-two factorial including cholesterol-lowering therapy and antioxidant vitamin supplementation.24 There might be a certain difference between the statin treatment and placebo groups, although the detailed profiles were not fully presented in the post-trial study.
Significance of the ‘carry-over effect’
Clinical trials of lifestyle modification often cause carry-over effects and bring favorable cardiovascular outcomes because the changes in lifestyle are usually prolonged even after termination of the trial. We found five articles that demonstrated carry-over effects of the transient intervention, as shown in Table 3. In the TOHP (Trials of Hypertension Prevention),29 it was shown that salt restriction could reduce long-term risks of cardiovascular events. Ohta et al.43 reported that salt intake of school-aged children exceeded the recommended amounts and was positively correlated with that of their parents. Education about salt restriction from childhood in the family is important for the prevention of hypertension and cardiovascular disease.43 In the post-trial follow-up study of the DCCT published in 2000,26 a significant reduction in diabetic retinopathy was observed in the transient intensive treatment group at the end of the post-trial follow-up period. However, the blood glucose level was significantly lower even at the end of the post-trial follow-up period, which was four years after the cessation of the intensive treatment. Although the report stated that the results could be regarded as an example of the memory phenomenon, we judged that the favorable cardiovascular outcome was due to carry-over effects of the transient intervention in this study.
Possible mechanisms of the cardiometabolic memory phenomenon
Regarding the mechanism of the memory phenomenon, a few explanations were mentioned in the articles. Some reports suggested that reduced generation of the glycation end products during the trial period might contribute to the memory phenomenon after the trial (UKPDS 801 and DCCT/EDIC7). Suppression of vascular or cardiac remodeling during the trial period might also cause the memory phenomenon (HOPE-TOO14 and TRACE15).
Limitations
Several possible limitations must be considered in our systematic review. First, the possibility of selection bias cannot be ruled out because we retrieved only articles written in English using a small number of search terms. Second, the possibility of publication bias cannot be excluded because the articles with positive results might be more easily published. It may be difficult to publish studies reporting the loss of beneficial effects after the termination of the intervention, as mentioned earlier. Third, clinical trials with relatively small sample sizes were included in our analysis. Unknown cofounders can be mingled in such cases. Finally, we used data only from RCTs. Patients enrolled in an RCT might not be representative of patients observed in clinical settings. Therefore, our results might not always be applicable to our routine medical care.
Conclusions
In conclusion, our systematic review showed the existence and clinical significance of cardiometabolic memory. To understand and prevent cardiovascular events, the impact of cardiometabolic memory should be highly emphasized as a concept supporting the importance of intensive intervention in hypertension, diabetes, and dyslipidemia.
References
Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA . 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008; 359: 1577–1589.
Zoungas S, Chalmers J, Neal B, Billot L, Li Q, Hirakawa Y, Arima H, Monaghan H, Joshi R, Colagiuri S, Cooper ME, Glasziou P, Grobbee D, Hamet P, Harrap S, Heller S, Lisheng L, Mancia G, Marre M, Matthews DR, Mogensen CE, Perkovic V, Poulter N, Rodgers A, Williams B, MacMahon S, Patel A, Woodward M, ADVANCE-ON Collaborative Group. Follow-up of blood-pressure lowering and glucose control in type 2 diabetes. N Engl J Med 2014; 371: 1392–1406.
Patel A, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, Harrap S, Poulter N, Marre M, Cooper M, Glasziou P, Grobbee DE, Hamet P, Heller S, Liu LS, Mancia G, Mogensen CE, Pan CY, Rodgers A, Williams B . Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 2007; 370: 829–840.
Ford I, Murray H, McCowan C, Packard CJ . Long-term safety and efficacy of lowering low-density lipoprotein cholesterol with statin therapy: 20-year follow-up of West of Scotland Coronary Prevention study. Circulation 2016; 133: 1073–1080.
Action to Control Cardiovascular Risk in Diabetes Follow-On Eye Study Group, the Action to Control Cardiovascular Risk in Diabetes Follow-On Study Group. Persistent effects of intensive glycemic control on retinopathy in type 2 diabetes in the action to control cardiovascular risk in diabetes (ACCORD) follow-on study. Diabetes Care 2016; 39: 1089–1100.
Wong MG, Perkovic V, Chalmers J, Woodward M, Li Q, Cooper ME, Hamet P, Harrap S, Heller S, MacMahon S, Mancia G, Marre M, Matthews D, Neal B, Poulter N, Rodgers A, Williams B, Zoungas S, ADVANCE-ON Collaborative Group. Long-term benefits of intensive glucose control for preventing end-stage kidney disease: ADVANCE-ON. Diabetes Care 2016; 39: 694–700.
Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular outcomes Study Research G. Intensive diabetes treatment and cardiovascular outcomes in type 1 diabetes: The DCCT/EDIC study 30-year follow-up. Diabetes Care 2016; 39: 686–693.
Hayward RA, Reaven PD, Wiitala WL, Bahn GD, Reda DJ, Ge L, McCarren M, Duckworth WC, Emanuele NV, VADT Investigators. Follow-up of glycemic control and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2015; 372: 2197–2206.
Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Research Group Lachin JM, White NH, Hainsworth DP, Sun W, Cleary PA, Nathan DM . Effect of intensive diabetes therapy on the progression of diabetic retinopathy in patients with type 1 diabetes: 18 years of follow-up in the DCCT/EDIC. Diabetes 2015; 64: 631–642.
DCCT/EDIC Research Group de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW Zinman B . Intensive diabetes therapy and glomerular filtration rate in type 1 diabetes. N Engl J Med 2011; 365: 2366–2376.
Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, Raskin P, Zinman B, Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med 2005; 353: 2643–2653.
Ku E, Glidden DV, Johansen KL, Sarnak M, Tighiouart H, Grimes B, Hsu CY . Association between strict blood pressure control during chronic kidney disease and lower mortality after onset of end-stage renal disease. Kidney Int 2015; 87: 1055–1060.
Julius S, Nesbitt SD, Egan BM, Weber MA, Michelson EL, Kaciroti N, Black HR, Grimm RH Jr, Messerli FH, Oparil S, Schork MA, Trial of Preventing Hypertension (TROPHY) Study Investigators. Feasibility of treating prehypertension with an angiotensin-receptor blocker. N Engl J Med 2006; 354: 1685–1697.
Bosch J, Lonn E, Pogue J, Arnold JM, Dagenais GR, Yusuf S, HOPE/HOPE-TOO Study Investigators. Long-term effects of ramipril on cardiovascular events and on diabetes: Results of the hope study extension. Circulation 2005; 112: 1339–1346.
Buch P, Rasmussen S, Abildstrom SZ, Køber L, Carlsen J, Torp-Pedersen C, TRACE investigators. The long-term impact of the angiotensin-converting enzyme inhibitor trandolapril on mortality and hospital admissions in patients with left ventricular dysfunction after a myocardial infarction: Follow-up to 12 years. Eur Heart J 2005; 26: 145–152.
Jong P, Yusuf S, Rousseau MF, Ahn SA, Bangdiwala SI . Effect of enalapril on 12-year survival and life expectancy in patients with left ventricular systolic dysfunction: a follow-up study. Lancet 2003; 361: 1843–1848.
Margolis KL, Davis BR, Baimbridge C, Ciocon JO, Cuyjet AB, Dart RA, Einhorn PT, Ford CE, Gordon D, Hartney TJ, Julian Haywood L, Holtzman J, Mathis DE, Oparil S, Probstfield JL, Simpson LM, Stokes JD, Wiegmann TB, Williamson JD, ALLHAT Collaborative Research Group. Long-term follow-up of moderately hypercholesterolemic hypertensive patients following randomization to pravastatin vs usual care: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT-LLT). J Clin Hypertens (Greenwich) 2013; 15: 542–554.
Sever PS, Chang CL, Gupta AK, Whitehouse A, Poulter NR, ASCOT Investigators. The anglo-scandinavian cardiac outcomes trial: 11-year mortality follow-up of the lipid-lowering arm in the U.K. Eur Heart J 2011; 32: 2525–2532.
Sever PS, Poulter NR, Dahlof B, Wedel H, Beevers G, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes G, Mehlsen J, Nieminen MS, O’Brien ET, Ostergren J, ASCOT Investigators. The Anglo-Scandinavian Cardiac Outcomes Trial lipid lowering arm: extended observations 2 years after trial closure. Eur Heart J 2008; 29: 499–508.
Holdaas H, Fellstrom B, Cole E, Nyberg G, Olsson AG, Pedersen TR, Madsen S, Grönhagen-Riska C, Neumayer HH, Maes B, Ambühl P, Hartmann A, Staffler B, Jardine AG, Assessment of LEscol in Renal Transplantation (ALERT) Study Investigators. Long-term cardiac outcomes in renal transplant recipients receiving fluvastatin: the alert extension study. Am J Transplant 2005; 5: 2929–2936.
Strandberg TE, Pyörälä K, Cook TJ, Wilhelmsen L, Faergeman O, Thorgeirsson G, Pedersen TR, Kjekshus J, 4S Group. Mortality and incidence of cancer during 10-year follow-up of the scandinavian simvastatin survival study (4S). Lancet 2004; 364: 771–777.
LIPID Study Group (Long-term Intervention with Pravastatin in Ischaemic Disease). Long-term effectiveness and safety of pravastatin in 9014 patients with coronary heart disease and average cholesterol concentrations: the lipid trial follow-up. Lancet 2002; 359: 1379–1387.
Holman RR, Paul SK, Bethel MA, Neil HA, Matthews DR . Long-term follow-up after tight control of blood pressure in type 2 diabetes. N Engl J Med 2008; 359: 1565–1576.
Heart Protection Study Collaborative Group, Bulbulia R, Bowman L, Wallendszus K, Parish S, Armitage J, Peto R, Collins R . Effects on 11-year mortality and morbidity of lowering LDL cholesterol with simvastatin for about 5 years in 20,536 high-risk individuals: a randomised controlled trial. Lancet 2011; 378: 2013–2020.
Lindström J, Peltonen M, Eriksson JG, Ilanne-Parikka P, Aunola S, Keinänen-Kiukaanniemi S, Uusitupa M, Tuomilehto J, Finnish Diabetes Prevention Study (DPS). Improved lifestyle and decreased diabetes risk over 13 years: Long-term follow-up of the randomised Finnish diabetes prevention study (DPS). Diabetologia 2013; 56: 284–293.
The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N Engl J Med 2000; 342: 381–389.
Li G, Zhang P, Wang J, Gregg EW, Yang W, Gong Q, Li H, Li H, Jiang Y, An Y, Shuai Y, Zhang B, Zhang J, Thompson TJ, Gerzoff RB, Roglic G, Hu Y, Bennett PH . The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up study. Lancet 2008; 371: 1783–1789.
Jafar TH, Jehan I, Liang F, Barbier S, Islam M, Bux R, Khan AH, Nadkarni N, Poulter N, Chaturvedi N, Ebrahim S . Control of blood pressure and risk attenuation: post trial follow-up of randomized groups. PLoS ONE 2015; 10: e0140550.
Cook NR, Cutler JA, Obarzanek E, Buring JE, Rexrode KM, Kumanyika SK, Appel LJ, Whelton PK . Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). Br Med J 2007; 334: 885–888.
Hirata C, Miyai N, Idoue A, Utsumi M, Hattori S, Iwahara A, Uematsu Y, Shiba M, Arita M . Effect of metabolic syndrome components and their clustering on carotid atherosclerosis in a sample of the general Japanese population. Hypertens Res 2016; 39: 362–366.
Fujii M, Ohnishi H, Saitoh S, Akasaka H, Miura T, Mori M . The combination of abdominal obesity and high-sensitivity C-reactive protein predicts new-onset hypertension in the general Japanese population: the Tanno-Sobetsu study. Hypertens Res 2015; 38: 426–432.
Sasamura H, Nakaya H, Julius S, Tomotsugu N, Sato Y, Takahashi F, Takeuchi M, Murakami M, Ryuzaki M, Itoh H, for the STAR CAST investigators. Feasibility of regression of hypertension using contemporary antihypertensive agents. Am J Hypertens 2013; 26: 1381–1388.
Harrap SB, Van der Merwe WM, Griffin SA, Macpherson F, Lever AF . Brief angiotensin converting enzyme inhibitor treatment in young spontaneously hypertensive rats reduces blood pressure long-term. Hypertension 1990; 16: 603–614.
Wu JN, Berecek KH . Prevention of genetic hypertension by early treatment of spontaneously hypertensive rats with the angiotensin converting enzyme inhibitor captopril. Hypertension 1993; 22: 139–146.
Sasamura H, Hayashi K, Ishiguro K, Nakaya H, Saruta T, Itoh H . Prevention and regression of hypertension: role of renal microvascular protection. Hypertens Res 2009; 32: 658–664.
Sasamura H, Itoh H . ‘Memory’ and ‘legacy’ in hypertension and lifestyle-related diseases. Hypertens Res 2012; 35: 272–273.
Nakaya H, Sasamura H, Hayashi M, Saruta T . Temporary treatment of prepubescent rats with angiotensin inhibitors suppresses the development of hypertensive nephrosclerosis. J Am Soc Nephrol 2001; 12: 659–666.
Nakaya H, Sasamura H, Mifune M, Shimizu-Hirota R, Kuroda M, Hayashi M, Saruta T . Prepubertal treatment with angiotensin receptor blocker causes partial attenuation of hypertension and renal damage in adult Dahl salt-sensitive rats. Nephron 2002; 91: 710–718.
Ishiguro K, Sasamura H, Sakamaki Y, Itoh H, Saruta T . Developmental activity of the renin-angiotensin system during the ‘critical period’ modulates later L-NAME-induced hypertension and renal injury. Hypertens Res 2007; 30: 63–75.
Ishiguro K, Hayashi K, Sasamura H, Sakamaki Y, Itoh H . ‘Pulse’ treatment with high-dose angiotensin blocker reverses renal arteriolar hypertrophy and regresses hypertension. Hypertension 2009; 53: 83–89.
Oguchi H, Sasamura H, Shinoda K, Morita S, Kono H, Nakagawa K, Ishiguro K, Hayashi K, Nakamura M, Azegami T, Oya M, Itoh H . Renal arteriolar injury by salt intake contributes to salt memory for the development of hypertension. Hypertension 2014; 64: 784–791.
Togashi N, Maeda T, Yoshida H, Koyama M, Tanaka M, Furuhashi M, Shimamoto K, Miura T . Angiotensin II receptor activation in youth triggers persistent insulin resistance and hypertension—a legacy effect? Hypertens Res 2012; 35: 334–340.
Ohta Y, Iwayama K, Suzuki H, Sakata S, Hayashi S, Iwashima Y, Takata A, Kawano Y . Salt intake and eating habits of school-aged children. Hypertens Res 2016; 39: 812–817.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Itoh, H., Kurihara, I., Miyashita, K. et al. Clinical significance of ‘cardiometabolic memory’: a systematic review of randomized controlled trials. Hypertens Res 40, 526–534 (2017). https://doi.org/10.1038/hr.2016.192
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2016.192
Keywords
This article is cited by
-
Pre-emptive medicine for hypertension and its prospects
Hypertension Research (2019)
-
Hypertension with diabetes mellitus complications
Hypertension Research (2018)
-
Metabolic syndrome status over 2 years predicts incident chronic kidney disease in mid-life adults: a 10-year prospective cohort study
Scientific Reports (2018)
-
Organ memory: a key principle for understanding the pathophysiology of hypertension and other non-communicable diseases
Hypertension Research (2018)
