
Abstract
Long-chain omega-3 polyunsaturated fatty acids (PUFAs) from fish have been shown to lower blood pressure. However, there is little information about the association with orthostatic hypotension, for which hypertension is a risk factor. We investigated the associations between serum long-chain omega-3 PUFAs and orthostatic hypotension in 1666 middle-aged or older men and women free of cardiovascular disease (CVD), diabetes or hypertension in 1998–2001 in the Kuopio Ischemic Heart Disease Risk Factor Study (KIHD) in eastern Finland. We also investigated the associations with mercury exposure, a major source of which is fish, and which has been associated with higher CVD risk in KIHD. Orthostatic hypotension was defined as decrease in systolic blood pressure of at least 20 mm Hg or diastolic blood pressure of at least 10 mm Hg within 1 min of standing. Orthostatic hypotension was found in 146 participants (8.8%). The mean serum concentrations were 1.67% (s.d. 0.92) for eicosapentaenoic acid, 0.79% (s.d. 0.16) for docosapentaenoic acid (DPA) and 2.78 (s.d. 0.92) for docosahexaenoic acid of all serum fatty acids. The mean pubic hair mercury concentration was 1.5 μg g−1 (s.d. 1.6). We did not find statistically significant associations between the serum long-chain omega-3 PUFAs or pubic hair mercury and risk of orthostatic hypotension, except for DPA. Those in the highest vs. the lowest serum DPA tertile had multivariate-adjusted 41% lower odds for orthostatic hypotension (95% confidence interval 7–63%, P-trend=0.02). Serum long-chain omega-3 PUFAs or mercury exposure were not associated with the risk of orthostatic hypotension, except for the inverse association with DPA.
Similar content being viewed by others


Introduction
Orthostatic hypotension is common in the elderly, occurring in 15–30% among those >65 years of age, and it is associated with higher levels of mortality and morbidity, including cardiovascular disease (CVD), falls and fractures.1, 2 Orthostatic hypotension can occur acutely secondary to, for example, medication use or fluid or blood loss, or it can be a chronic condition as a result of altered blood pressure regulation mechanisms, CVD or autonomic nervous system dysfunction.1, 2, 3 Increase in systolic blood pressure with increasing age is one of the major determinants of orthostatic hypotension development.1, 2
The long-chain omega-3 polyunsaturated fatty acids (PUFAs) from fish, eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), have been associated with lower risk of hypertension in population studies.4, 5, 6, 7, 8, 9 In addition, fish oil supplementation has been shown to lower blood pressure, especially in hypertensive subjects who were not taking hypertension medication.10 The beneficial effects of the long-chain omega-3 PUFAs on blood pressure regulation may be explained by, for example, improved vasodilation and vasoreactivity and arterial compliance.11
Based on the potential benefits of the long-chain omega-3 PUFAs in hypertension prevention, we hypothesized that these fatty acids might also be associated with lower risk of orthostatic hypotension in older people. Currently, there is very little information on the association between the long-chain omega-3 PUFAs and orthostatic hypotension. Therefore, the aim of this study was to investigate the associations between serum long-chain omega-3 PUFA concentrations, an objective biomarker of exposure, and orthostatic hypotension in middle-aged or older men and women in the Kuopio Ischemic Heart Disease Risk Factor Study (KIHD) population in Eastern Finland. Previously, higher serum long-chain omega-3 PUFA concentration was associated with lower blood pressure in this study population.8 We also investigated the association between mercury exposure and risk of orthostatic hypotension, because fish is the major source of methylmercury and mercury exposure has been associated with a higher risk of CVD in the KIHD cohort.9, 12 The previous findings for the association between mercury exposure and hypertension have been mixed,11, 13, 14, 15, 16, 17, 18, 19 but little evidence exists for the association with orthostatic hypotension.
Methods
Study population
The KIHD is an ongoing population-based cohort study designed to investigate risk factors for CVD and other chronic diseases in middle-aged and older men and women in Eastern Finland.20 The study protocol was approved by the Research Ethics committee of the University of Kuopio. All subjects gave their written informed consent. The KIHD complies with the principles of the Declaration of Helsinki.
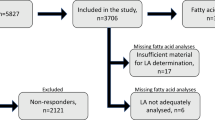
The baseline examinations of the KIHD were conducted between 1984 and 1989 to a random sample of men living in the city of Kuopio and neighboring rural communities. A total of 2682 men aged 42, 48, 54 or 60 years at baseline were recruited into two cohorts. The first cohort consisted of 1166 men (83.3% of those eligible) aged 54 years, enrolled between 1984 and 1986, and the second cohort included 1516 men (82.6%) aged 42, 48, 54 or 60 years, enrolled between 1986 and 1989. During the years 1998–2001, all men from the second cohort were invited to the 11-year re-examinations of the study, and 854 men (85.6%) participated. These examinations were also the baseline for 920 postmenopausal women (78.4% of the 1173 eligible women) from the same area, aged 53–73 years. For the present study, we excluded those with missing data on orthostatic hypotension (n=6) or on serum fatty acids (n=16) or pubic hair mercury (n=86) at the 11-year re-examinations, leaving 1666 participants (837 men and 829 women) for the analyses.
Blood pressure measurements
All blood pressure measurements were performed by specially trained nurses. Resting blood pressure was measured between 0800 and 1000 hours on the first examination day by one nurse with a random-zero mercury sphygmomanometer (Bodenseewerk Perkin-Elmer GmbH, Überlingen, Germany) with cuff-size of 120 × 350 mm2 or 150 × 430 mm2. The measuring protocol included, after a supine rest of 5 min, three measurements in supine position with 5-min intervals, one measurement in standing position 1 min after standing and two measurements in sitting position with 5-min intervals. The mean of all six systolic pressure values was used in the present analyses as the systolic blood pressure and the mean of all six diastolic measurements as diastolic blood pressure. Hypertension was defined as blood pressure >140/90 mm Hg at the follow-up examinations or treatment for hypertension. Orthostatic hypotension was defined as a decrease in systolic blood pressure of at least 20 mm Hg or diastolic blood pressure of at least 10 mm Hg within 1 min of standing.
Serum fatty acids
Serum total fatty acids were determined from frozen samples with a NB-351 capillary column (HNU-Nordion, Helsinki, Finland) by a Hewlett-Packard 5890 Series II gas chromatograph (Hewlett-Packard Company, Avondale, PA, USA, since 1999 Agilent Technologies, USA) with a flame ionization detector. Serum was extracted with chloroform–methanol and fatty acids were methylated with methanol and sulfuric acid prior to gas chromatography. Each analyte had an individual reference standard and the analytes were quantified with an internal standard method using eicosane. Results for fatty acids were obtained in μmol l−1 and in the data analyses proportion of a fatty acid from the total fatty acids was used. The coefficient of variation for repeated measurements of fatty acids ranged from 7% (palmitic acid 16:0) to 16% (lignoceric acid 24:0).
Other measurements
The subjects gave fasting blood samples between 0800 and 1000 hours on the examinations in 1998–2001. They were instructed to abstain from ingesting alcohol for 3 days and from smoking and eating for 12 h prior to giving the sample. Detailed descriptions of the determination of blood glucose, assessment of medical history and medications, family history of diseases, smoking and alcohol consumption have been published.21 Diabetes was defined as self-reported diabetes mellitus or fasting plasma glucose of >6.9 mmol l−1 or 2-h oral glucose tolerance test plasma glucose >11.0 mmol l−1 at the study examinations. Education was assessed in years by using self-administered questionnaire. Physical activity was assessed using the KIHD 12-Month Leisure-Time Physical Activity Questionnaire.22 Body mass index was computed as the ratio of weight in kilograms to the square of height in meters. Dietary intake of foods and nutrients was assessed at the time of blood sampling using 4-day food recording.23 Mercury in pubic hair was determined by flow injection analysis–cold vapor atomic absorption spectrometry and amalgamation, as described.24
Statistical analysis
After confirming that gender did not modify the associations between the serum fatty acids or pubic hair mercury and orthostatic hypotension (P-interactions>0.2), the associations were investigated in the whole study population. The relationships between baseline characteristics and serum EPA+docosapentaenoic acid (DPA)+DHA were explored by means and linear (for continuous variables) or logistic regression (for dichotomous variables). The associations between serum fatty acids and hair mercury with orthostatic hypotension were analyzed with logistic regression. Odds ratios were used to estimate the risk of orthostatic hypotension. The Model 1 was adjusted for age, gender and examination year. The Model 2 included the Model 1 and the history of hypertension in family, leisure-time physical activity, body mass index, alcohol intake, years of education, urinary potassium, urinary sodium, smoking status, history of CVD, type 2 diabetes or cancer, systolic and diastolic blood pressure, number of drugs and drugs associated with orthostatic hypotension (angiotensin-converting enzyme inhibitors, diuretics, antihypertensives, beta-blockers, calcium channel blockers, vasodilators, nitrates, antidepressants, benzodiazepines, antipsychotics and antidepressants).
The cohort mean was used to replace missing values of covariates (<5.2% of values). Few participants reported using fish oil supplements (n<10). Tests of linear trend across tertiles of serum fatty acids or hair mercury were conducted by assigning the median values for each category of exposure variable and treating those as a single continuous variable. Statistical significance of the interactions on a multiplicative scale was assessed by likelihood ratio tests with a cross-product term. All P-values were two-tailed (α=0.05). Data were analyzed with SPSS 21.0 for Windows (IBM, Armonk, NY, USA).
Results
The mean serum concentrations were 1.67% (s.d. 0.92) for EPA, 0.79% (s.d. 0.16) for DPA and 2.78% (s.d. 0.92) for DHA of all serum fatty acids. The mean pubic hair mercury concentration was 1.5 μg g−1 (s.d. 1.6). Table 1 shows the characteristics of the KIHD population at baseline. Those with higher serum EPA+DPA+DHA were more likely to be women, have a higher education with higher income and higher hair mercury content with higher urinary potassium and sodium. They also had higher intake of fish and vegetables (excluding potatoes) and lower intake of dairy and meat and meat products. They were also less likely to smoke.
The number of subjects with orthostatic hypotension was 146 (83 men and 63 women, 8.8% of the study population). We did not find statistically significant associations between the serum long-chain omega-3 PUFA concentrations and risk of orthostatic hypotension, except for DPA (Table 2). Those in the highest vs. the lowest serum DPA tertile had multivariate-adjusted 41% (95% CI 7–63%) lower odds for orthostatic hypotension (P-trend=0.02).
We did not find statistically significant associations between pubic hair mercury content and risk of orthostatic hypotension (Table 2). Pubic hair mercury did not modify the associations between serum long-chain omega-3 PUFAs and orthostatic hypotension either (P-interactions>0.05).
Discussion
The results from this population-based cohort study of middle-aged and older men and women from Eastern Finland suggest that, except for the inverse association with DPA, higher serum concentrations of the long-chain omega-3 PUFAs were not associated with the risk of orthostatic hypotension. No associations were observed with mercury exposure either.
There is little prior information about the impact of the long-chain omega-3 PUFAs on orthostatic hypotension, but these fatty acids have been associated with lower blood pressure in population studies,4, 5, 6, 7, 8, 19 and fish oil supplementation has been shown to lower blood pressure in randomized trials.10 Also in the KIHD cohort, higher total serum long-chain omega-3 PUFA concentration was associated with lower blood pressure and the associations were similar with the individual long-chain omega-3 PUFAs, EPA, DPA and DHA.8 One of the major determinants of development of orthostatic hypotension is increase in systolic blood pressure with ageing.1, 2 Therefore, the long-chain omega-3 PUFAs could also have benefits regarding prevention of orthostatic hypotension. However, in the current analysis we found an inverse association with the risk of orthostatic hypotension only with DPA. DPA can be synthesized endogenously from EPA or obtained from the diet, mainly from seafood.25 Currently, much less is known about the health effects of DPA, when compared with the other long-chain omega-3 PUFAs, EPA and DHA.26 However, in studies that have investigated all three long-chain omega-3 PUFAs, DPA appears to have similar inverse associations with the risk of CVD as EPA and DHA.9, 27, 28, 29, 30, 31, 32 Because so far few studies have evaluated the impact of DPA on blood pressure regulation with mixed findings,8, 17, 33 and even less is known about the impact of EPA, DPA or DHA on the risk of orthostatic hypotension, the results from our study should be interpreted cautiously.
We have previously shown that high hair mercury concentration attenuated the benefits of the long-chain omega-3 PUFAs on the risk of CVD in men in this study population.9, 12 However, high hair mercury content was not associated with blood pressure, and it did not modify the inverse associations between the serum long-chain omega-3 PUFAs and blood pressure.8 Our findings indicate that moderate, long-term mercury exposure is not associated with orthostatic hypotension either. This suggest little effect of mercury on blood pressure regulation, concordant with the findings from other study populations.19
The main strength of this study is the use of established biomarkers of exposure, the circulating fatty acid concentrations and hair mercury, to investigate the associations with orthostatic hypotension. These biomarkers do not depend on study participants’ recall ability, which ensures objectivity of the exposure variables and minimizes the chance of bias through misclassification and recall bias. The serum long-chain omega-3 PUFA concentration is an indicator of exposure during few previous weeks,34 while the hair mercury indicates long-term exposure.35 The additional strengths of this study include extensive examinations on potential confounders and population-based recruitment.
In conclusion, our findings suggest that the long-chain omega-3 PUFAs or mercury exposure have little impact on the risk of orthostatic hypotension in ageing men and women. The role of DPA in blood pressure regulation warrants further studies.
References
Gupta V, Lipsitz LA . Orthostatic hypotension in the elderly: diagnosis and treatment. Am J Med 2007; 120: 841–847.
Feldstein C, Weder AB . Orthostatic hypotension: a common, serious and underrecognized problem in hospitalized patients. J Am Soc Hypertens 2012; 6: 27–39.
Lu DY, Sung SH, Yu WC, Cheng HM, Chuang SY, Chen CH . Wave reflections, arterial stiffness, heart rate variability and orthostatic hypotension. Hypertens Res 2014; 37: 1056–1061.
Pauletto P, Puato M, Caroli MG, Casiglia E, Munhambo AE, Cazzolato G, Bittolo Bon G, Angeli MT, Galli C, Pessina AC . Blood pressure and atherogenic lipoprotein profiles of fish-diet and vegetarian villagers in Tanzania: the Lugalawa study. Lancet 1996; 348: 784–788.
Dallongeville J, Yarnell J, Ducimetiere P, Arveiler D, Ferrieres J, Montaye M, Luc G, Evans A, Bingham A, Hass B, Ruidavets JB, Amouyel P . Fish consumption is associated with lower heart rates. Circulation 2003; 108: 820–825.
Mozaffarian D, Gottdiener JS, Siscovick DS . Intake of tuna or other broiled or baked fish versus fried fish and cardiac structure, function, and hemodynamics. Am J Cardiol 2006; 97: 216–222.
Ueshima H, Stamler J, Elliott P, Chan Q, Brown IJ, Carnethon MR, Daviglus ML, He K, Moag-Stahlberg A, Rodriguez BL, Steffen LM, Van Horn L, Yarnell J, Zhou B,, INTERMAP Research Group. Food omega-3 fatty acid intake of individuals (total, linolenic acid, long-chain) and their blood pressure: INTERMAP study. Hypertension 2007; 50: 313–319.
Virtanen JK, Nyantika AN, Kauhanen J, Voutilainen S, Tuomainen TP . Serum long-chain n-3 polyunsaturated fatty acids, methylmercury and blood pressure in an older population. Hypertens Res 2012; 35: 1000–1004.
Virtanen JK, Voutilainen S, Rissanen TH, Mursu J, Tuomainen TP, Korhonen MJ, Valkonen VP, Seppänen K, Laukkanen JA, Salonen JT . Mercury, fish oils, and risk of acute coronary events and cardiovascular disease, coronary heart disease, and all-cause mortality in men in eastern Finland. Arterioscler Thromb Vasc Biol 2005; 25: 228–233.
Miller PE, Van Elswyk M, Alexander DD . Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid and blood pressure: a meta-analysis of randomized controlled trials. Am J Hypertens 2014; 27: 885–896.
Pedersen EB, Jorgensen ME, Pedersen MB, Siggaard C, Sorensen TB, Mulvad G, Hansen JC, Asmund G, Skjoldborg H . Relationship between mercury in blood and 24-h ambulatory blood pressure in Greenlanders and Danes. Am J Hypertens 2005; 18: 612–618.
Virtanen JK, Laukkanen JA, Mursu J, Voutilainen S, Tuomainen TP . Serum long-chain n-3 polyunsaturated fatty acids, mercury, and risk of sudden cardiac death in men: a prospective population-based study. PLoS ONE 2012; 7: e41046.
Fillion M, Mergler D, Sousa Passos CJ, Larribe F, Lemire M, Guimaraes JR . A preliminary study of mercury exposure and blood pressure in the Brazilian Amazon. Environ Health 2006; 5: 29.
Valera B, Dewailly E, Poirier P . Environmental mercury exposure and blood pressure among Nunavik Inuit adults. Hypertension 2009; 54: 981–986.
Choi AL, Weihe P, Budtz-Jorgensen E, Jorgensen PJ, Salonen JT, Tuomainen TP, Murata K, Nielsen HP, Petersen MS, Askham J, Grandjean P . Methylmercury exposure and adverse cardiovascular effects in Faroese whaling men. Environ Health Perspect 2009; 117: 367–372.
Vupputuri S, Longnecker MP, Daniels JL, Guo X, Sandler DP . Blood mercury level and blood pressure among US women: results from the National Health and Nutrition Examination Survey 1999-2000. Environ Res 2005; 97: 195–200.
Nyantika AN, Tuomainen TP, Kauhanen J, Voutilainen S, Virtanen JK . Serum long-chain omega-3 polyunsaturated fatty acids and future blood pressure in an ageing population. J Nutr Health Aging 2014; 19: 498–503.
Mozaffarian D, Shi P, Morris JS, Grandjean P, Siscovick DS, Spiegelman D, Willett WC, Rimm EB, Curhan GC, Forman JP . Mercury exposure and risk of hypertension in US men and women in 2 prospective cohorts. Hypertension 2012; 60: 645–652.
Xun P, Hou N, Daviglus M, Liu K, Morris JS, Shikany JM, Sidney S, Jacobs DR, He K . Fish oil, selenium and mercury in relation to incidence of hypertension: a 20-year follow-up study. J Intern Med 2011; 270: 175–186.
Salonen JT . Is there a continuing need for longitudinal epidemiologic research? The Kuopio Ischaemic Heart Disease Risk Factor Study. Ann Clin Res 1988; 20: 46–50.
Salonen JT, Nyyssonen K, Korpela H, Tuomilehto J, Seppanen R, Salonen R . High stored iron levels are associated with excess risk of myocardial infarction in eastern Finnish men. Circulation 1992; 86: 803–811.
Lakka TA, Venalainen JM, Rauramaa R, Salonen R, Tuomilehto J, Salonen JT . Relation of leisure-time physical activity and cardiorespiratory fitness to the risk of acute myocardial infarction. N Engl J Med 1994; 330: 1549–1554.
Voutilainen S, Rissanen TH, Virtanen J, Lakka TA, Salonen JT . Low dietary folate intake is associated with an excess incidence of acute coronary events: The Kuopio Ischemic Heart Disease Risk Factor Study. Circulation 2001; 103: 2674–2680.
Salonen JT, Seppänen K, Nyyssönen K, Korpela H, Kauhanen J, Kantola M, Tuomilehto J, Esterbauer H, Tatzber F, Salonen R . Intake of mercury from fish, lipid peroxidation, and the risk of myocardial infarction and coronary, cardiovascular, and any death in eastern Finnish men. Circulation 1995; 91: 645–655.
Byelashov OA, Sinclair AJ, Kaur G . Dietary sources, current intakes, and nutritional role of omega-3 docosapentaenoic acid. Lipid Technology 2015; 27: 79–82.
Mozaffarian D, Wu JH . (n-3) fatty acids and cardiovascular health: are effects of EPA and DHA shared or complementary? J Nutr 2012; 142: 614S–625S.
Virtanen JK, Mursu J, Voutilainen S, Tuomainen TP . Serum long-chain n-3 polyunsaturated fatty acids and risk of hospital diagnosis of atrial fibrillation in men. Circulation 2009; 120: 2315–2321.
Lemaitre RN, King IB, Mozaffarian D, Kuller LH, Tracy RP, Siscovick DS . n-3 Polyunsaturated fatty acids, fatal ischemic heart disease, and nonfatal myocardial infarction in older adults: the Cardiovascular Health Study. Am J Clin Nutr 2003; 77: 319–325.
de Oliveira Otto MC, Wu JH, Baylin A, Vaidya D, Rich SS, Tsai MY, Jacobs DR Jr, Mozaffarian D . Circulating and dietary omega-3 and omega-6 polyunsaturated fatty acids and incidence of CVD in the Multi-Ethnic Study of Atherosclerosis. J Am Heart Assoc 2013; 2: e000506.
Mozaffarian D, Lemaitre RN, King IB, Song X, Huang H, Sacks FM, Rimm EB, Wang M, Siscovick DS . Plasma phospholipid long-chain omega-3 fatty acids and total and cause-specific mortality in older adults: a cohort study. Ann Intern Med 2013; 158: 515–525.
Mozaffarian D, Lemaitre RN, King IB, Song X, Spiegelman D, Sacks FM, Rimm EB, Siscovick DS . Circulating long-chain omega-3 fatty acids and incidence of congestive heart failure in older adults: the Cardiovascular Health Study. Ann Intern Med 2011; 155: 160–170.
Wu JH, Marchioli R, Silletta MG, Macchia A, Song X, Siscovick DS, Harris WS, Masson S, Latini R, Albert C, Brown NJ, Lamarra M, Favaloro RR, Mozaffarian D . Plasma phospholipid omega-3 fatty acids and incidence of postoperative atrial fibrillation in the OPERA trial. J Am Heart Assoc 2013; 2: e000397.
O'Sullivan TA, Bremner AP, Beilin LJ, Ambrosini GL, Mori TA, Huang RC, Oddy WH . Polyunsaturated fatty acid intake and blood pressure in adolescents. J Hum Hypertens 2012; 26: 178–187.
Hodson L, Skeaff CM, Fielding BA . Fatty acid composition of adipose tissue and blood in humans and its use as a biomarker of dietary intake. Prog Lipid Res 2008; 47: 348–380.
Roman HA, Walsh TL, Coull BA, Dewailly E, Guallar E, Hattis D, Mariën K, Schwartz J, Stern AH, Virtanen JK, Rice G . Evaluation of the cardiovascular effects of methylmercury exposures: current evidence supports development of a dose-response function for regulatory benefits analysis. Environ Health Perspect 2011; 119: 607–614.
Acknowledgements
The study was supported by funding from the University of Eastern Finland.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Nyantika, A., Tuomainen, TP., Kauhanen, J. et al. Serum long-chain omega-3 polyunsaturated fatty acids and risk of orthostatic hypotension. Hypertens Res 39, 543–547 (2016). https://doi.org/10.1038/hr.2016.19
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2016.19
Keywords
This article is cited by
-
Environmental stress and vestibular inputs modulate cardiovascular responses to orthostasis in hypertensive rats
Hypertension Research (2018)
