
Abstract
Combination therapy with angiotensin II receptor blockers and angiotensin-converting enzyme inhibitors (ACEIs) requires further evaluation in patients with diabetic nephropathy and hypertension. In a post hoc analysis of the Olmesartan Reducing Incidence of Endstage renal disease in diabetic Nephropathy Trial with hypertension, we examined the effects of olmesartan on renal and cardiovascular outcomes in the presence or absence of an ACEI. Among 563 patients randomized to receive either olmesartan (n=280) or placebo (n=283), 73.5% (n=414) received a concomitant ACEI. Compared with placebo, olmesartan significantly reduced proteinuria in both the ACEI-treated and non-ACEI-treated groups. The respective changes in the urinary protein creatinine ratio in the olmesartan-treated and placebo-treated groups were −32.6% and +21.1% without an ACEI (P=0.001) and −17.0% and +2.2% with an ACEI (P=0.028). In the olmesartan group, 115 patients developed primary renal outcomes (41.1%) compared with 129 (45.6%) in the placebo group (hazard ratio (HR): 0.97, P=0.787). The respective HRs in the ACEI-treated and non-ACEI-treated groups were 1.02 (P=0.891) and 0.84 (P=0.450). 40 olmesartan-treated patients (14.3%) and 53 placebo-treated patients (18.7%) developed secondary cardiovascular outcomes (HR: 0.65, P=0.042). The respective HRs in the ACEI-treated and non-ACEI-treated groups were 0.69 (P=0.129) and 0.51 (P=0.129). Olmesartan was well tolerated. Dual blockade treatment caused more hyperkalemia than monotherapy. In patients with diabetic nephropathy and hypertension, olmesartan significantly reduced proteinuria, independent of ACEI treatment and cardiovascular outcome but failed to show additional renal benefit compared with ACEI treatment alone. The cardiovascular benefit of dual treatment requires further evaluation.
Similar content being viewed by others

Introduction
Type 2 diabetes is the leading cause of end-stage renal disease worldwide.1 Control of glycemia2 and blood pressure (BP)3 has been shown to reduce proteinuria and the rate of decline of renal function. Treatment with renin–angiotensin system (RAS) inhibitors including angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs) has been shown to improve clinical outcomes in diabetic patients with hypertension, including reducing the incidence of microalbuminuria in patients with normoalbuminuria,4, 5 the progression to overt proteinuria in patients with microalbuminuria6, 7, 8 and the development of end-stage renal disease in patients with overt nephropathy.9, 10
Theoretically, dual blockade of the RAS by inhibiting ACE activity and blocking the angiotensin II receptor may confer additional organ protection. However, in a small randomized controlled study (n=133), combination treatment with lisinopril and irbesartan did not have additional renoprotective benefits in type 2 diabetes compared with the use of either drug alone administered in optimal high doses.11 In the ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial (ONTARGET), the renal composite outcome was worse in patients treated with a combination therapy of telmisartan and ramipril compared with those treated with either drug alone.12 However, among the 25 620 participants in the ONTARGET, only 2781 (11%) and 1025 (4%) had type 2 diabetes with micro- or macroalbuminuria, respectively. Among the patients with diabetic nephropathy, combination therapy did not have significant deleterious effects.13 A combination of the direct renin inhibitor aliskiren and valsartan did not demonstrate beneficial effects on renal outcome,14 although proteinuria was reduced by dual blockade.15 When used as monotherapy, ACEIs or ARBs have been shown to reduce the incidence of renal events in patients with diabetic nephropathy. However, the combination of these agents has not incrementally improved renal outcomes compared with monotherapy.
In the Olmesartan Reducing Incidence of Endstage renal disease in diabetic Nephropathy Trial (ORIENT), which enrolled type 2 diabetic patients receiving conventional antihypertensive agents including ACEIs, treatment with olmesartan, an ARB, reduced BP, proteinuria and the rate of decline of the serum creatinine reciprocal (1/SCr) compared with placebo. Although treatment with olmesartan did not reduce the primary composite outcome of doubling of serum creatinine (SCr), end-stage renal disease and all-cause death, the adjusted hazard ratio (HR) of the secondary composite cardiovascular outcome was 0.64 (95% confidence interval (CI): 0.43–0.98; P=0.039) in the olmesartan group.16
Given the ongoing debate on the safety and efficacy of dual blockade of the RAS on organ protection, we conducted a post-hoc analysis of the ORIENT16 to examine whether the effects of olmesartan on renal and cardiovascular outcomes were modified by the concomitant use of an ACEI in type 2 diabetic patients with hypertension and overt nephropathy.
Methods
Study design and patients
The ORIENT commenced in 2003 and was approved by the appropriate Institutional Ethics Committees. All patients provided written informed consent. We enrolled type 2 diabetic patients from Japan and Hong Kong with the following inclusion criteria: (1) age between 30 and 70 years; (2) urinary albumin:creatinine ratio (UACR) >300 mg gCr–1 in the first morning urine sample; and (3) SCr concentration of 1.0–2.5 mg dl–1 in females and 1.2–2.5 mg dl–1 in males (normal range <1.0 mg dl–1). The major exclusion criteria included the following: (1) type 1 diabetes; (2) history of myocardial infarction or coronary artery bypass grafting within 3 months before consent; (3) percutaneous coronary intervention, carotid artery or peripheral artery revascularization within 6 months; (4) stroke or transient ischemic attack within 1 year; (5) unstable angina pectoris or heart failure of New York Heart Association functional class III or IV; (6) rapidly progressive renal disease within 3 months before consent; (7) severe orthostatic hypotension; and (8) a serum potassium level ⩽3.5 or ⩾5.5 mEq l–1. In this analysis, we included patients with hypertension defined as a BP ⩾130/80 mm Hg or treatment with any anti-hypertensive agents during the run-in period according to the Japan Society of Hypertension Guidelines (2009).17
Definitions of study outcomes
The efficacy measure was the time to the first event of the primary composite outcome of doubling of SCr, end-stage renal disease (SCr >5 mg dl–1, dialysis, transplantation), and all-cause death. SCr was measured at a central laboratory in Japan (SRL, Tokyo, Japan). The secondary composite outcomes included the following: (1) a composite end point of first occurrence of cardiovascular death, non-fatal stroke except for transient ischemic attacks, non-fatal myocardial infarction, hospitalization for unstable angina, hospitalization for heart failure, revascularization of the coronary, carotid, or peripheral arteries, or lower extremity amputation; (2) change in proteinuria; (3) rate of decline of the estimated glomerular filtration rate (eGFR) using the Japanese equation and the modification of diet in renal disease (MDRD) equation for estimating the GFR in Japanese and Chinese patients, respectively.18, 19
Statistical analysis
The Cox regression model was applied to estimate the HR between treatment groups with the 95% CI for the renal and cardiovascular composite event rates.20 The covariates in the model were (1) UACR and SCr at baseline and regions (Japan/Hong Kong) for the renal composite event rate, and (2) baseline UACR, history of cardiovascular disease, and age for the cardiovascular composite event rate. The Kaplan–Meier method was used to estimate the cumulative event rate in each treatment group stratified by the use of an ACEI.21
The linear mixed-effects model was used to compare the trend in the percent change of the urinary protein:creatinine ratio (UPCR) and that of eGFR between the treatment and placebo groups. Serious adverse events and discontinuation of the study drug due to adverse events were summarized. All statistical tests were two sided with 0.05 set as the significance level. Statistical analyses were performed using the Statistical Analysis System version 9.2 (SAS Institute, Cary, NC, USA).
Results
Patients
Among the 566 type 2 diabetic patients with overt nephropathy randomized in the ORIENT, 563 patients (363 Japanese and 200 Chinese) had hypertension. Of these, 280 received olmesartan and 283 received placebo in addition to conventional antihypertensive therapy (Table 1). Of the 563 patients with hypertension, 414 (73.1%) were treated with ACEIs that were continued at the same dosage throughout the study period of 3.2 (0.6) years (mean (s.d.)). The ratio of patients receiving olmesartan was similar in the ACEI-treated (205/414) and non-ACEI-treated groups (75/149), at 50%.
Blood pressure
In the olmesartan group, the mean BP fell from 141.9/77.8 mm Hg at baseline to 137.6/75.1 mm Hg at week 12 and 131.9/72.2 mm Hg at week 144. The respective values were 140.9/77.2, 140.4/76.6 and 136.6/73.6 mm Hg in the placebo group (Figure 1a). There was a greater reduction in time-averaged systolic and diastolic BP (SBP and DBP) in the olmesartan group compared with the placebo group (SBP, 2.8 mm Hg; DBP, 1.6 mm Hg, P<0.01). The daily dose of olmesartan ranged from 10 to 40 mg, with 49.5%, 60.8% and 63.9% of patients receiving 40 mg at weeks 12, 48 and 144, respectively. In the non-ACEI-treated group, olmesartan treatment reduced BP significantly compared with placebo (SBP, 6.4 mm Hg; DBP, 4.0 mm Hg, P<0.001, Figure 1b), but this phenomenon was not observed in the ACEI-treated group (SBP, 1.0 mm Hg (P=0.417); DBP, 0.7 mm Hg (P=0.323), Figure 1c).

Change in blood pressure in type 2 diabetic patients with overt nephropathy and hypertension during treatment with olmesartan or placebo (a) all patients; (b) patients not treated with an ACEI and (c) patients treated with an ACEI). ACEI, angiotensin-converting enzyme inhibitor; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Renal outcome
In the placebo group, compared with a median baseline UPCR of 2.05 g gCr–1, the percentage changes were +11.6% at week 12, +6.7% at week 48 and −3.1% at week 144. The respective changes in the olmesartan group, with a median baseline UPCR of 2.19 g gCr–1, were −19.7%, −20.4% and −25.0%. Olmesartan significantly reduced the UPCR by −22.2%, whereas placebo increased it by +7.3% (P=0.002, Figure 2a). In both the ACEI-treated and non-ACEI-treated groups, treatment with olmesartan reduced the UPCR significantly compared with placebo. The changes in the UPCR in the olmesartan group and the placebo group were −32.6% and +21.1% without an ACEI (P=0.001, Figure 2b) and −17.0% and +2.2% with an ACEI (P=0.028, Figure 2c), respectively.

Changes in proteinuria expressed as percentage change in the urinary protein to creatinine ratio from baseline during treatment with olmesartan or placebo in type 2 diabetic patients with overt nephropathy and hypertension ((a) all patients; (b) patients not treated with an angiotensin-converting enzyme inhibitor (ACEI) and (c) patients treated with an ACEI).
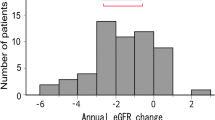
In the olmesartan group, the median change in eGFR was −4.640 (interquartile range: −9.316 to −1.913) ml min–1 per 1.73 m2 per year, which was slower compared with the placebo group (−5.804 (interquartile range: −9.208 to −2.781) ml min–1 per 1.73 m2 per year; P=0.039, Figure 3a). In the non-ACEI-treated group, olmesartan monotherapy significantly slowed the rate of decline of eGFR compared with placebo (−4.497 vs. −7.120 ml min–1 per 1.73 m2 per year; P=0.027, Figure 3b). In the ACEI-treated group, the respective changes were −4.788 and −5.547 ml min–1 per 1.73 m2 per year (P=0.202, Figure 3c).

Distribution of changes in the estimated glomerular filtration rate (eGFR) decline according to 2 ml min–1 per 1.73 m2 per year intervals in type 2 diabetic patients with overt nephropathy and hypertension ((a) all patients; (b) patients not treated with an angiotensin-converting enzyme inhibitor (ACEI) and (c) patients treated with an ACEI).
The renal composite outcome occurred in 115 patients in the olmesartan group (41.1%) and 129 patients in the placebo group (45.6%). The HR for renal outcome in the olmesartan-treated patients was 0.97 (P=0.787, Figure 4a) in the entire cohort, 0.84 (P=0.450, Figure 4b) in the non-ACEI-treated group, and 1.02 (P=0.891, Figure 4c) in the ACEI-treated group.

Kaplan–Meier analysis of the time to the primary composite renal end point in type 2 diabetic patients with overt nephropathy and hypertension ((a) all patients; (b) patients not treated with an angiotensin-converting enzyme inhibitor (ACEI) and (c) patients treated with an ACEI). HR, hazard ratio.
Cardiovascular outcome
The composite cardiovascular outcome occurred in 40 olmesartan-treated patients (14.3%) and 53 placebo-treated patients (18.7%) with HR of 0.65 (P=0.042, Figure 5a). The effects of olmesartan on cardiovascular outcome were similar in the non-ACEI-treated group with HR of 0.52 (P=0.129, Figure 5b) and the ACEI-treated group with HR of 0.69 (P=0.129, Figure 5c; Table 2).

Kaplan–Meier analysis of the time to the secondary composite cardiovascular end point in type 2 diabetic patients with overt nephropathy and hypertension ((a) all patients; (b) patients not treated with an angiotensin-converting enzyme inhibitor (ACEI) and (c) patients treated with an ACEI). HR, hazard ratio.
Safety
Serious adverse events occurred in 145 olmesartan-treated patients (51.8%) and 169 placebo-treated patients (59.7%). In total, 73 (26.1%) olmesartan-treated patients and 64 (22.6%) placebo-treated patients were discontinued from treatment before study completion due to adverse events. The discontinuation rate due to hyperkalemia was higher in the olmesartan group compared with the placebo group (26 (9.3%) vs. 15 (5.3%)). The respective rates were 11.7% vs. 7.2% in the ACEI-treated patients and 2.7% vs. 0% in the non-ACEI-treated patients (Table 3). None of the patients required acute dialysis in the first 6 months of the study, and only one patient (0.4%) in each group was discontinued due to acute renal failure during the study period.
Discussion
The primary objective of this post-hoc analysis was to evaluate the benefit–risk ratio for the use of olmesartan, indicated for the treatment of hypertension, on the prevention of renal and cardiovascular outcomes when used in combination with an ACEI. To this end, treatment with olmesartan reduced SBP in patients not treated with ACEI but had little effect on BP in patients receiving an ACEI. However, regardless of treatment with an ACEI, olmesartan treatment reduced proteinuria, albeit with neutral effects on renal outcome. In agreement with our primary analysis, treatment with olmesartan reduced cardiovascular outcomes, showing similar trends in patients with or without ACEI treatment.
Renal outcomes
The beneficial effects of olmesartan on reducing proteinuria, regardless of concomitant treatment with an ACEI, were in agreement with previous studies.4, 5, 6, 7, 8, 9, 10, 22, 23 In the ORIENT, olmesartan significantly slowed the rate of decline of eGFR compared with placebo, and there was a numerical risk reduction of 16% for renal outcome in the non-ACEI-treated group, which was similar to that reported in the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) study.9 These findings support the renoprotective effects of olmesartan monotherapy in type 2 diabetic patients with hypertension and overt nephropathy. In the ACEI-treated group, treatment with olmesartan did not confer an additional renoprotective effect, with HR of 1.02. In this regard, it has been suggested that the beneficial effects of RAS blockade on renal outcome might be most evident when administered early rather than during an advanced stage of diabetic nephropathy.24
In a subanalysis of the ONTARGET12 that examined the effects of a combination therapy of ramipril and telmisartan on cardiovascular outcomes in high-risk patients, dual therapy increased the risk of renal outcome by 9% compared with ramipril alone. Despite attenuating the rate of increase in the UACR, dual therapy was associated with a more rapid decline in renal function. These findings differed from the results of the ORIENT, where a reduction in proteinuria was not accompanied by a decline in renal function. Of note, only 37.5% of participants in the ONTARGET had diabetes, and of those, 700 had overt proteinuria.25 Although some patients in the entire cohort exhibited rapid deterioration of renal function during treatment with combination therapy, diabetic patients with overt nephropathy demonstrated a nonsignificant 8% risk reduction of renal outcome in favor of combination therapy compared with telmisartan alone.13
Apart from the controversies caused by the ONTARGET, the debate on the risk–benefit ratio of dual blockade of the RAS was recently fuelled by the lack of benefits on renal outcome observed using a combination treatment of the direct renin inhibitor aliskiren and valsartan,14 despite greater reduction in proteinuria compared with monotherapy.15 Against this background, the potential adverse effects of dual blockade of the RAS using various combinations of ACEIs, ARBs or renin inhibitors, notably hyperkalemia, hypotension and renal dysfunction, remain a subject of major concern.
Owing to their multiple risk factors and pre-existing complications, patients in the ORIENT had frequent hospitalizations and high rates of treatment discontinuation, with similar rates between the olmesartan and placebo groups. The discontinuation rate due to hyperkalemia was higher in the olmesartan group than in the placebo group (9.3% vs. 5.3%). However, none of the study patients required acute dialysis in the first 6 months of the study, and only one patient (0.4%) in each group developed acute renal failure during the study period. This low rate of adverse renal effects might be because of the gradual titration of the olmesartan dose from 10 to 20 to 40 mg at 4-week intervals to ensure the safety and tolerability of dual therapy for RAS blockade.
Cardiovascular outcome
In the Irbesartan Diabetic Nephropathy Trial and the RENAAL study, which enrolled type 2 diabetic patients with hypertension and overt nephropathy, treatment with an ARB reduced renal but not cardiovascular outcomes, except for heart failure.9, 10 In the RENAAL-Asia subanalysis, 34% of participants experienced cardiovascular events26 compared with 16% in the ORIENT. In the latter study, patients had better control of blood glucose and lipids compared with those enrolled in the RENAAL study, most likely due to overall improvement in care over time. In this post-hoc analysis, despite near optimal metabolic and BP control, patients treated with olmesartan had a 35% risk reduction of cardiovascular outcome (P=0.042), with similar trends in the ACEI-treated (HR=0.69, P=0.129) and non-ACEI-treated groups (HR=0.52, P=0.129; Figures 2a–c). In a randomized controlled trial of patients with stable angina pectoris, treatment with olmesartan reduced the atheroma volume detected by intravascular ultrasound.27 Taken together, our results suggest that in addition to reducing BP, olmesartan may improve cardiovascular outcome independent of treatment with an ACEI.
Conclusion
In this post-hoc analysis of type 2 diabetic patients with hypertension and overt nephropathy, the majority of whom were optimally treated with an ACEI, olmesartan reduced BP and proteinuria. Including olmesartan did not have an additional benefit on renal outcome. Despite its neutral effects on renal outcome in the presence of an ACEI, treatment with olmesartan reduced the occurrence of cardiovascular events with similar trends in ACEI-treated and non-ACEI-treated patients. Despite the controversies surrounding combined treatment with ACEIs and ARBs, our results suggest that further studies are required to evaluate the cardiovascular effects of olmesartan in patients treated with or without an ACEI.
References
Excerpts From the United States Renal Data System 2008. Annual Data Report: international comparison. Am J Kidney Dis 2009; 53 (Suppl 1): S297–S308.
Bilous R . Microvascular disease: what does the UKPDS tell us about diabetic nephropathy? Diabet Med 2008; 25 (Suppl 2): 25–29.
Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, Tuttle K, Douglas J, Hsueh W, Sowers J . Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis 2000; 36: 646–661.
Ruggenenti P, Fassi A, Ilieva AP, Bruno S, Iliev IP, Brusegan V, Rubis N, Gherardi G, Arnoldi F, Ganeva M, Ene-Iordache B, Gaspari F, Perna A, Bossi A, Trevisan R, Dodesini AR, Remuzzi G . Preventing microalbuminuria in type 2 diabetes. N Engl J Med 2004; 351: 1941–1951.
Haller H, Ito S, Izzo JL Jr, Januszewicz A, Katayama S, Menne J, Mimran A, Rabelink TJ, Ritz E, Ruilope LM, Rump LC, Viberti G, ROADMAP Trial Investigators. Olmesartan for the delay or prevention of microalbuminuria in type 2 diabetes. N Engl J Med 2011; 364: 907–917.
Parving H-H, Lehnert H, Brochner-Mortensen J, Gomis R, Andersen S, Arner P . The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 2001; 345: 870–878.
Makino H, Haneda M, Babazono T, Moriya T, Ito S, Iwamoto Y, Kawamori R, Takeuchi M, Katayama S, INNOVATION Study Group. Prevention of transition from incipient to overt nephropathy with telmisartan in patients with type 2 diabetes. Diabetes Care 2007; 30: 1577–1578.
Uzu T, Sawaguchi M, Maegawa H, Kashiwagi A . Reduction of microalbuminuria in patients with type 2 diabetes: the Shiga Microalbuminuria Reduction Trial (SMART). Diabetes Care 2007; 30: 1581–1583.
Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S, RENAAL Study Investigators. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001; 345: 861–869.
Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I, Collaborative Study Group. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 2001; 345: 851–860.
Fernandez Juarez G, Luño J, Barrio V, de Vinuesa SG, Praga M, Goicoechea M, Cachofeiro V, Nieto J, Fernández Vega F, Tato A, Gutierrez E . Effect of dual blockade of the renin-angiotensin system on the progression of type 2 diabetic nephropathy: a randomized trial. Am J Kidney Dis 2013; 61: 211–218.
Mann JF, Schmieder RE, McQueen M, Dyal L, Schumacher H, Pogue J, Wang X, Maggioni A, Budaj A, Chaithiraphan S, Dickstein K, Keltai M, Metsärinne K, Oto A, Parkhomenko A, Piegas LS, Svendsen TL, Teo KK, Yusuf S, ONTARGET investigators. Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trial. Lancet 2008; 372: 547–553.
Mann JF, Anderson C, Gao P, Gerstein HC, Boehm M, Rydén L, Sleight P, Teo KK, Yusuf S . Dual inhibition of the renin-angiotensin system in high-risk diabetes and risk for stroke and other outcomes: results of the ONTARGET trial. J Hypertens 2013; 31: 414–421.
Parving HH, Brenner BM, McMurray JJ, de Zeeuw D, Haffner SM, Solomon SD, Chaturvedi N, Persson F, Desai AS, Nicolaides M, Richard A, Xiang Z, Brunel P, Pfeffer MA . Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med 2012; 367: 2204–2213.
Parving HH, Persson F, Lewis JB, Lewis EJ, Hollenberg NK . Aliskiren combined with losartan in type 2 diabetes and nephropathy. N Engl J Med 2008; 358: 2433–2446.
Imai E, Chan JC, Ito S, Yamasaki T, Kobayashi F, Haneda M, Makino H . Effects of olmesartan on renal and cardiovascular outcomes in type 2 diabetes with overt nephropathy: a multicentre, randomised, placebo-controlled study. Diabetologia 2011; 54: 2978–2986.
Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mitsuyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshima H, Umemura S, Ishimitsu T, Rakugi H, on behalf of The Japanese Society of Hypertension Committee. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res 2009; 32: 3–107.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A . Revised equations for estimating glomerular filtration rate (GFR) from serum creatinine in Japan. Am J Kidney Dis 2009; 53: 982–992.
Stevens LA, Coresh J, Greene T, Levey AS . Assessing kidney function—measured and estimated glomerular filtration rate. N Engl J Med 2006; 354: 2473–2483.
Cox DR . Regression models and life-tables. J R Stat Soc [B] 1972; 34: 187–220.
Kaplan EL, Meier P . Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53: 457–481.
Viberti G, Wheeldon NM . Microalbuminuria reduction with valsartan in patients with type 2 diabetes mellitus: a blood pressure-independent effect. Circulation 2002; 106: 672–678.
Mogensen CE, Neldam S, Tikkanen I, Oren S, Viskoper R, Watts RW, Cooper ME . Randomised controlled trial of dual blockade of renin-angiotensin system in patients with hypertension, microalbuminuria, and non-insulin dependent diabetes: the candesartan and lisinopril microalbuminuria (CALM) study. BMJ 2000; 321: 1440–1444.
Heerspink HJ, de Zeeuw D . The kidney in type 2 diabetes therapy. Rev Diabet Stud 2011; 8: 392–402.
Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, Schumacher H, Dagenais G, Sleight P, Anderson C, ONTARGET Investigators. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med 2008; 358: 1547–1559.
Chan JC, Wat NM, So WY, Lam KS, Chua CT, Wong KS, Morad Z, Dickson TZ, Hille D, Zhang Z, Cooper ME, Shahinfar S, Brenner BM, Kurokawa K, Asian RENAAL Study Investigators. Renin angiotensin aldosterone system blockade and renal disease in patients with type 2 diabetes. An Asian perspective from the RENAAL Study. Diabetes Care 2004; 27: 874–879.
Hirohata A, Yamamoto K, Miyoshi T, Hatanaka K, Hirohata S, Yamawaki H, Komatsubara I, Murakami M, Hirose E, Sato S, Ohkawa K, Ishizawa M, Yamaji H, Kawamura H, Kusachi S, Murakami T, Hina K, Ohe T. . Impact of olmesartan on progression of coronary atherosclerosis a serial volumetric intravascular ultrasound analysis from the OLIVUS (impact of OLmesarten on progression of coronary atherosclerosis: evaluation by intravascular ultrasound) trial. J Am Coll Cardiol 2010; 55: 976–982.
Acknowledgements
The ORIENT study was supported by a research grant from Daiichi Sankyo.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
EI has received consulting and lecture fees and grant support from Daiichi-Sankyo, Kyowa-Hakko-Kirin, MSD, Kaken, Chugai, Takeda, Shionogi, Dainippon-Sumitomo, Astellas and Pfizer. MH has received a research grant from Daiichi-Sankyo. TY, FK and AH are employees of Daiichi-Sankyo. SI has received consultancy fees, lecture fees and research grants from Daiichi-Sankyo, Novartis, Astellas, MSD and Pfizer. JCNC has received consultancy and lecture fees from Daiichi-Sankyo, MSD, Astra Zeneca, Bristol Myers Squibb, GSK, Pfizer and Bayer. Her institution has received grant support from these companies. HM has received consultancy fees, lecture fees and research grants from Daiichi-Sankyo, Astellas, MSD, Kyowa-Hakko-Kirin, Takeda, Chugai, Novartis, Boehringer Ingelheim, Dainippon-Sumitomo and Kowa.
Appendix
Appendix
Steering Committee: H Makino, S Ito, M Haneda, E Imai, JCN Chan.
Independent Data Monitoring Committee: S Katayama, T Hashimoto, H Origasa.
Renal/Cardiovascular Endpoints Adjudication Committee: T Moriya, T Babazono, K Shikata, H Daida, M Takayama, N Tanahashi, K Kitagawa.
Person in Charge of Randomization and Blinding: C Hamada.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Imai, E., Haneda, M., Yamasaki, T. et al. Effects of dual blockade of the renin–angiotensin system on renal and cardiovascular outcomes in type 2 diabetes with overt nephropathy and hypertension in the ORIENT: a post-hoc analysis (ORIENT–Hypertension). Hypertens Res 36, 1051–1059 (2013). https://doi.org/10.1038/hr.2013.86
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2013.86
Keywords
This article is cited by
-
Efficacy and Safety of Dual Blockade of the Renin–Angiotensin–Aldosterone System in Diabetic Kidney Disease: A Meta-Analysis
American Journal of Cardiovascular Drugs (2019)
-
Combination antihypertensive therapy in clinical practice. The analysis of 1254 consecutive patients with uncontrolled hypertension
Journal of Human Hypertension (2016)
-
The necessity and effectiveness of mineralocorticoid receptor antagonist in the treatment of diabetic nephropathy
Hypertension Research (2015)
-
Causal Measures of the Treatment Effect Captured by Candidate Surrogate Endpoints
Journal of Agricultural, Biological, and Environmental Statistics (2015)
-
Dual Renin-Angiotensin-Aldosterone Blockade: Promises and Pitfalls
Current Hypertension Reports (2015)
