
Abstract
Life expectancy (LE) is a measure that describes the health status of a population. The few published studies that have examined the impact of hypertension on LE were predominantly performed in Western populations. The effect of hypertension on LE has not been reported in an Asian population. Thus, we examined the impact of hypertension on LE in the Japanese population, which has the highest LE worldwide. The abridged life table method was applied to calculate the LEs of both normotensive and hypertensive men and women aged 40–85 years. Hypertensive participants were categorized as having either stage 1 or stage 2 hypertension. Age-specific mortality rates across different groups were estimated using the person–year method based on the follow-up data from a representative Japanese population in a national survey (NIPPON DATA80). The proportion of hypertensive patients in the baseline survey was 50.5% for men and 41.4% for women. The LE of 40-year-old men and women was 41.7 years and 48.7 years, respectively, in normotensive participants and 39.5 and 45.8 years, respectively, in hypertensive participants. The LE difference between normotensive and hypertensive participants was 2.2 years for men and 2.9 years for women. LE decreased with increasing stages of hypertension. Similar patterns of LE, with respect to blood pressure (BP) status, were observed in all index ages and for both genders. At the population level, hypertension leads to decreased LE and affects both genders similarly. Our findings highlight the importance of preventing high BP and the consequences of hypertension in Japanese population.
Similar content being viewed by others


Introduction
Studies have shown that hypertension, or high blood pressure (BP), is quite prevalent worldwide1 and is a major risk factor for morbidity and mortality in young, middle-aged and elderly individuals of both genders.2, 3, 4 Moreover, hypertension is also closely linked to the aging process, as the prevalence and the risk of hypertension increase with age.5, 6 A similar influence of age is also found with regard to mortality.7, 8 The measure life expectancy (LE), which is a comprehensive estimate of a given population's health status, provides a useful and direct means to communicate disease burden and can be used as a universal measure of health in a population. This information can be used to prioritize planning and policy making for the detection, treatment and control of various health conditions.
There are few published studies that have investigated the impact of hypertension on LE.9, 10, 11 Although the impact of hypertension on premature death and LE has been estimated in Western populations, the effect of hypertension on LE has not been reported in Asian populations, including the Japanese population. This information will be of importance because it is unclear how hypertension affects LE in the Japanese population, which currently has the highest longevity worldwide. The present study examined the LE of a representative sample of Japanese population in which hypertension status varied. This is the first population-based Japanese study of LE for people with and without hypertension.
Methods
Data source
The present study analyzed data from NIPPON DATA80 (National Integrated Project for Prospective Observation of Non-communicable Disease and its Trends in the Aged), which was collected from a baseline survey performed in 1980. The details of this cohort have been reported elsewhere.3, 12, 13 In brief, 300 areas were selected by stratified random sampling from all over Japan, and a sample of residents aged 30 years or older in these areas was invited to participate. A total of 10 546 residents (4639 men and 5907 women) participated in the survey (response rate: 76.6%). The baseline surveys were carried out at local public health centers. The participants were followed for 24 years, until November 2004.
To identify death events among the cohort, we used national vital statistics. In accordance with Japan's Family Registration Law, all death certificates issued by the medical doctors are to be forwarded to the Ministry of Health, Labor and Welfare via the public health centers in the respective participant's area of residency. We confirmed death in each area by computer matching of vital statistics data using area, sex, date of birth and date of death as key codes. Permission to use the national vital statistics was obtained from the Management and Coordination Agency of the Government of Japan. In the present study, we excluded participants who had missing information at baseline or who were lost to follow-up (n=941). Thus, the final sample consisted of 9605 participants (4228 men and 5377 women). There were no significant differences between the participants who were lost to follow-up and those who were included in the current study in terms of several risk factors. Approval for this study was obtained from the Institutional Review Board of Shiga University of Medical Science (no. 12-18 2000).
BP measurement and categories
Baseline BP was measured by trained observers using a standard mercury sphygmomanometer on the right arm of seated participants after at least 5 min of rest. Hypertension was defined as systolic BP⩾140 mm Hg and/or diastolic BP⩾90 mm Hg and/or taking antihypertensive medication. Participants with BP<140 mm Hg and diastolic BP<90 mm Hg were defined as normotensive. We further categorized the hypertensive participants, without regard to the use of antihypertensive medication, according to the classification by the JNC-714 as follows: stage 1 hypertension, systolic BP 140–159 mm Hg and/or diastolic BP 90–99 mm Hg, or stage 2 hypertension, systolic BP⩾160 mm Hg and/or diastolic BP⩾100 mm Hg. We decided not to consider treatment of hypertension in the categorization of our analyses because we wanted to evaluate the effect of increased BP levels, which can also arise in hypertensive patients under treatment. When the systolic and diastolic pressures fell into different categories, the higher category was selected for the purposes of classification.
Statistical analysis
Age-specific mortality rates for the cohort participants were calculated using the person–year method,15 and age was considered in the timescale with synchronization with the follow-up. The age bands used in this calculation were defined in 5-year increments. The age categories began at age 40–44 years, and the highest age category was set at age 85 years and over. The abridged life table method was used to calculate life expectancies using age-specific mortality rates. The fraction of the last age interval of life13, 16 was used to construct an abridged life table. Those fractions were calculated from a complete life table for the year 1990 in Japan.13 Each LE was calculated from age 40 to age 85 in 5-year intervals. We also calculated 95% confidence intervals for LE in each age group. All of the statistical analyses were performed using SAS release 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
Table 1 shows the basic characteristics of the participants with different hypertension statuses in the baseline survey. The proportion of hypertensive participants in the baseline survey was 50.5% for men and 41.4% for women. In men, 13.5% of the participants had stage 1 hypertension and 36.2% of the participants had stage 2 hypertension. In women, the respective proportions were 15.0% and 25.1%. Hypertensive patients were generally older and had higher mean plasma glucose and higher total blood cholesterol levels. This difference was observed in both men and women.
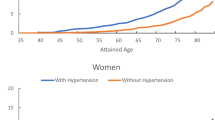
The overall LE of the 40-year-old participants, regardless of BP status, was 40.4 years for men and 47.0 years for women. These LE values were higher than the LEs in the complete life table for Japan from 1990. In that table, LE was 37.5 years for men and 42.9 years for women.17 The observed differences were consistent across all age groups in both genders. Table 2 shows the LE among the participants with different BP statuses from age 40 to 85 years and over. LEs in 40-year-old men and women were 41.7 years and 48.7 years, respectively, in normotensive participants and 39.5 years and 45.8 years, respectively, in hypertensive participants. Thus, the LEs of 40-year-old normotensive participants were greater than those of hypertensive participants. Similar patterns of LE with respect to BP status were observed in all the age groups. The LEs in men with stage 1 hypertension were greater than those of men with stage 2 hypertension. Similar results were observed in women. The longer LE for participants with stage 1 hypertension in comparison with participants with stage 2 hypertension was observed across all age indices for both genders.
Discussion
In this study, LE was estimated for Japanese men and women with and without diagnosed hypertension. The results attribute a significant loss of LE to hypertension. To the best of our knowledge, this is the first study to report the effect of the presence or absence of hypertension on LE in a Japanese population. We observed that the LE of hypertensive men and women was 2–3 years shorter than the LE of normotensive men and women, especially in the middle-aged categories. Increases in hypertension stage also inversely affected LE.
Similar to our observation, Loukine et al.11 recently reported a 2–3 years difference in LE associated with hypertension in a Canadian population. They estimated the LE in 40-year-old men and women to be 41.9 years and 45.8 years, respectively, in normotensive subjects and 38.8 years and 43.7 years, respectively, in hypertensive subjects. After estimating the effect of hypertension on LE in an eastern Finland population, Kiiskinen et al.10 reported that LE was shortened by 2.7 years in hypertensive men and 2.2 years in hypertensive women. Franco et al.,9 studying the participants in the Framingham Heart Study, reported that the differences in LE between 50-year-old normotensive and hypertensive subjects were 5.1 years in men and 4.9 years in women. They estimated the LE in 50-year-old men and women to be 29.7 years and 34.3 years, respectively, in normotensive subjects and 24.6 years and 29.4 years, respectively, in hypertensive subjects. The effect of hypertension on LE in the Framingham Heart Study was much greater than in our Japanese study, the Canadian study and the Finish study. We also observed that the LE for women is higher than that for men, a direct result of higher mortality among men. A similar pattern was observed for the populations both with and without hypertension. Similar observations were reported for the Canadian population, for both subjects with and without hypertension. We observed that the reduction in LE was larger for men than for women. The estimates from other studies were also consistent: the decrease in LE was greater for men than for women.10, 11 It is important to note that direct comparability with our results was hampered by differences in methodology, data used, reporting year and characteristics of the populations studied. Among the subcategories of hypertension, stage 1 and stage 2, decreases in the LE of 40-year-olds were observed as the hypertension grade increased. This tendency was less pronounced when we measured LE in the older-age groups. This finding might be attributed to the small sample size of the older-age group.
Regarding the effect of hypertension on the LE of the elderly population, we observed that the presence of hypertension was associated with reduced LE. Severe hypertension led to reductions in LE. However, the overall impact of milder hypertension was much more limited. Given the aging of the Japanese population and that of the worldwide population, these LE findings reemphasize the importance of hypertension control, even in the elderly.
Our finding is generalizable to the Japanese population by virtue of the cohort we used for the LE estimation. The NIPPON DATA80 cohort was initially selected by stratified random sampling throughout Japan as part of a national survey. Comparing our results with the complete life table for the same period in Japan,17 the overall LE of 40-year-old participants, regardless of BP status, was 40.4 years for men and 47.0 years for women. These were higher than the LEs from the complete life table in Japan in 1990, which were 37.5 years for men and 42.9 years for women. The LEs that we measured were greater than those from the complete life table. This difference might be attributed to the overall healthier status of our cohort. In the baseline survey, people with health problems, such as residents of long-term care facilities, could not participate in the survey. This exclusion criterion may have caused age-specific mortality rates to be lower than population as a whole, which could have resulted in the LE differences observed in this study. The stable population in the final age interval (age 85 and over) was calculated as the number of survivors 85 years or older divided by their death rate. Although this is an accepted way to analyze the final age interval for LE calculations, it may overestimate LE.13, 18 This overestimation also influences the difference between our results and those from the complete life table.
Possible misclassifications of long-term BP categories might also influence our results. The classification of hypertension status was made using only the information obtained from the baseline survey, with the assumption that individuals' hypertension status did not change during the follow-up period. This assumption would be violated if any normotensive participant became hypertensive with ageing. It is not possible to precisely ascertain how much change in hypertensive status occurred during the 24-year period. The influence of this misclassification might attenuate the LE differences observed among the groups, and misclassification might render our estimates more conservative. It should also be recognized that all of the LE differences observed in this study were not caused by hypertension status alone; in fact, other factors in addition to hypertension also affected the mortality rate. The LE differences among the hypertension categories result from the hypertensive participants' risk factor profile, not from BP alone. Thus, in addition to hypertension, other factors simultaneously influenced the LE in our population, including smoking habits,13 diabetes mellitus19 and dyslipidemia. Alternatively, hypertension is a convenient marker that functions as a surrogate for health risks not controlled for in the analysis.
In conclusion, the LEs of participants with different hypertension statuses were examined using data from a nationwide cohort study in Japan. A gradual decrease in LE was observed when hypertension was present, and the decrease was greater with increasing disease severity in both men and women.
References
Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J . Global burden of hypertension: analysis of worldwide data. Lancet 2005; 365: 217–223.
Gu Q, Burt VL, Paulose-Ram R, Yoon S, Gillum RF . High blood pressure and cardiovascular disease mortality risk among US adults: the third National Health and Nutrition Examination Survey mortality follow-up study. Ann Epidemiol 2008; 18: 302–309.
Lida M, Ueda K, Okayama A, Kodama K, Sawai K, Shibata S, Tanaka S, Keijnkai T, Horibe H, Minowa M, Yanagawa H, Hashimoto T, Nippon Data 80 Research Group. Impact of elevated blood pressure on mortality from all causes, cardiovascular diseases, heart disease and stroke among Japanese: 14 year follow-up of randomly selected population from Japanese--NIPPON DATA80. J Hum Hypertens 2003; 17: 851–857.
Murakami Y, Hozawa A, Okamura T, Ueshima H, The Evidence for Cardiovascular Prevention From Observational Cohorts in Japan Research Group. (EPOCH-JAPAN). Relation of blood pressure and all-cause mortality in 180,000 Japanese participants: pooled analysis of 13 cohort studies. Hypertension 2008; 51: 1483–1491.
Franklin SS, Gustin W, Wong ND, Larson MG, Weber MA, Kannel WB, Levy D . Hemodynamic patterns of age-related changes in blood pressure: the Framingham Heart Study. Circulation 1997; 96: 308–315.
Anderson GH, Blakeman N, Streeten D . The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens 1994; 12: 609–615.
Dunnell K . Ageing and mortality in the UK--national statistician's annual article on the population. Popul Trends 2008, 6–23.
Hoffmann R . Aging and Mortality. In: Hoffmann R (ed),. Socioeconomic Differences in Old Age Mortality. Springer: Netherlands. 2008 pp. 5–14.
Franco OH, Peeters A, Bonneux L, De Laet C . Blood pressure in adulthood and life expectancy with cardiovascular disease in men and women: life course analysis. Hypertension 2005; 46: 280–186.
Kiiskinen U, Vartiainen E, Puska P, Aromaa A . Long-term cost and life-expectancy consequences of hypertension. J Hypertens 1998; 16: 1103–1112.
Loukine L, Waters C, Choi BC, Ellison J . Health-adjusted life expectancy among Canadian adults with and without hypertension. Cardiol Res Pract 2011; 2011: 612968.
Rumana N, Turin TC, Miura K, Nakamura Y, Kita Y, Hayakawa T, Choudhury SR, Kadota A, Nagasawa SY, Fujioshi A, Takashima N, Okamura T, Okayama A, Ueshima H, NIPPON DATA80 Research Group. Prognostic value of ST-T abnormalities and left high R waves with cardiovascular mortality in Japanese (24-year follow-up of NIPPON DATA80). Am J Cardiol 2011; 107: 1718–1724.
Murakami Y, Ueshima H, Okamura T, Kadowaki T, Hozawa A, Kita Y, Hayakawa T, Okayama A, NIPPON DATA80 Research Group. Life expectancy among Japanese of different smoking status in Japan: NIPPON DATA80. J Epidemiol 2007; 17: 31–37.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ, The National High Blood Pressure Education Program Coordinating Committee. Seventh Report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003; 42: 1206–1252.
Breslow NE, Day NE . Statistical Methods in Cancer Research Volume II-The analysis of case-control studies. International Agency for Research on Cancer: Lyon. 1980 pp 41–81.
Chiang CL . The Life Table and its Applications. Robert E Krieger Publishing: Malabar, FL. 1984 pp 137–167.
Ministry of Health and Welfare. The 18th Life Table. Kosei Tokei Kyokai: Tokyo. 1998 pp 359–399.
Fukutomi K . Bias in the abridged life table constructed by a short method. Bull Inst Public Health 1984; 33: 45–55.
Turin TC, Murakami Y, Miura K, Rumana N, Kadota A, Ohkubo T, Okamura T,, Okayama A, Ueshima H . Diabetes and life expectancy among Japanese–NIPPON DATA80. Diabetes Res Clin Pract 2012; 96: e18–e22.
Acknowledgements
This study was supported by a grant-in-aid from the Ministry of Health, Labor and Welfare under the auspices of the Japanese Association for Cerebro-cardiovascular Disease Control, a Research Grant for Cardiovascular Diseases (7A-2) from the Ministry of Health, Labor and Welfare, and a Health and Labor Sciences Research Grant, Japan (Comprehensive Research on Aging and Health (H11-Chouju-046, H14-Chouju-003, H17-Chouju-012, H19-Chouju-Ippan-014))and the Comprehensive Research on Life-Style Related Diseases Center, including Cardiovascular Diseases and Diabetes Mellitus (H22-Jyunkankitou-Seisyu-Sitei-017). Nahid Rumana is supported by a Research Fellowship and Research Grants-In-Aid (P-21.09139) from the Japan Society for the Promotion of Science (JSPS), Tokyo, Japan. Dr Tanvir Chowdhury Turin is supported by Fellowship Awards from the Canadian Institutes of Health Research (CIHR), Canadian Diabetes Association (CDA), and the Interdisciplinary Chronic Disease Collaboration (ICDC) team grant funded by Alberta Innovates—Health Solutions (AI-HS). We appreciate the members of the NIPPON DATA80/90 Research Group, who are listed in the Appendix.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Appendix
Appendix
The NIPPON DATA80/90 research group
Chairperson: Hirotsugu Ueshima (Department of Health Science, Shiga University of Medical Science, Otsu, Shiga).
Co-Chairperson: NIPPON DATA80: Akira Okayama (The First Institute for Health Promotion and Health Care, Japan Anti-Tuberculosis Association, Tokyo); NIPPON DATA90: Tomonori Okamura (Department of Preventive Medicine and Public Health, Keio University, Tokyo).
Research members: Shigeyuki Saitoh (Department of 2nd Internal Medicine, Sapporo Medical University, Sapporo, Hokkaido), Kiyomi Sakata (Department of Hygiene and Preventive Medicine, Iwate Medical University, Morioka, Iwate), Atsushi Hozawa (Department of Public Health, Yamagata University Graduate School of Medicine, Yamagata), Takehito Hayakawa (Department of Hygiene and Preventive Medicine, Fukushima Medical University, Fukushima), Yosikazu Nakamura (Department of Public Health, Jichi Medical University, Shimotsuke, Tochigi), Yasuhiro Matsumura (Faculty of Health care, Kiryu University, Midori City, Gunma), Nobuo Nishi (Project for the National Health and Nutrition Survey, National Institute of Health and Nutrition, Tokyo), Nagako Okuda (The First Institute for Health Promotion and Health Care, Japan Anti-Tuberculosis Association, Tokyo), Toru Izumi (Faculty of Medicine, Kitasato University, Sagamihara, Kanagawa), Toshiyuki Ojima (Department of Community Health and Preventive Medicine, Hamamatsu University School of Medicine, Hamamatsu, Shizuoka), Koji Tamakoshi (Department of Public Health and Health Information Dynamics, Nagoya University Graduate School of Medicine, Nagoya, Aichi), Hideaki Nakagawa (Department of Epidemiology and Public Health, Kanazawa Medical University, Kanazawa, Ishikawa), Katsuyuki Miura, Takayoshi Ohkubo, Yoshikuni Kita, Aya Kadota (Department of Health Science, Shiga University of Medical Science, Otsu, Shiga), Yasuyuki Nakamura (Cardiovascular Epidemiology, Kyoto Women's University, Kyoto), Katsushi Yoshita (Osaka City University Graduate School of Human Life Science, Osaka), Kazunori Kodama, Fumiyoshi Kasagi (Radiation Effects Research Foundation, Hiroshima), and Yutaka Kiyohara (Department of Environmental Medicine, Kyushu University, Fukuoka).
Rights and permissions
About this article
Cite this article
Turin, T., Murakami, Y., Miura, K. et al. Hypertension and life expectancy among Japanese: NIPPON DATA80. Hypertens Res 35, 954–958 (2012). https://doi.org/10.1038/hr.2012.86
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2012.86
Keywords
This article is cited by
-
J-shaped curve for the association between serum uric acid levels and the prevalence of blood pressure abnormalities
Hypertension Research (2021)
-
Multi-state analysis of hypertension and mortality: application of semi-Markov model in a longitudinal cohort study
BMC Cardiovascular Disorders (2020)
-
Relationship between outpatient visit frequency and hypertension control: a 9-year occupational cohort study
Hypertension Research (2016)
-
Kidney Function, Albuminuria and Life Expectancy
Canadian Journal of Kidney Health and Disease (2014)
-
Chapter 1. Epidemiology of hypertension
Hypertension Research (2014)
