
Abstract
This study evaluated the impact of renal function on cardiovascular outcomes in elderly hypertensive patients enrolled in the Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive patients. The patients were randomly assigned to either a strict-treatment group (target systolic blood pressure (BP) <140 mm Hg, n=2212) or a mild-treatment group (target systolic BP, 140 to <160 mm Hg, n=2206), each with efonidipine (a T/L-type Ca channel blocker)-based regimens. Cardiovascular events (stroke, cardiovascular disease and renal disease) were evaluated during the 2-year follow-up period following the prospective randomized open-blinded end-point method. Estimated glomerular filtration rate (eGFR) was elevated throughout the trial period in both the strict-treatment (59.4–62 ml min−1 per 1.73 m2) and the mild-treatment group (58.8–61.4 ml min−1 per 1.73 m2). This tendency was also observed in diabetic patients and patients aged ⩾75 years, with baseline eGFR<60 ml min−1 per 1.73 m2. Baseline eGFR (<60 vs. ⩾60 ml min−1 per 1.73 m2) had no definite relationship with the incidence of cardiovascular events, nor did the level of BP control. Proteinuria at the time of entry into the study, however, was significantly correlated with cardiovascular event rates (7.1%), an association that was more apparent in patients with eGFR<60 ml min−1 per 1.73 m2 (8.2%). Furthermore, the event rate was more elevated in patients with greater declines in eGFR and was amplified when the baseline eGFR was <60 ml min−1 per 1.73 m2. In conclusion, the rates of decline of renal function and proteinuria constitute critical risk factors for cardiovascular events in elderly hypertensive patients, trends that are enhanced when baseline eGFR is diminished. Furthermore, the fact that efonidipine-based regimens ameliorate renal function in elderly hypertensive patients with chronic kidney disease may offer novel information on the mechanisms of cardiovascular protection.
Similar content being viewed by others

Introduction
Hypertension constitutes a critical public health problem, causing multiple organ dysfunctions that can precipitate serious cardiovascular events including heart failure, stroke and vascular disease. The kidney is also an important target organ for hypertension, and damage to this organ aggravates hypertension, forming a vicious circle of hypertensive renal injury. To mitigate renal injury, antihypertensive therapy has been established as an effective modality for delaying the progression of chronic kidney disease (CKD), and a number of studies have reported that lowering blood pressure (BP) minimizes the decline in glomerular filtration rate (GFR).1, 2 Nevertheless, the level to which BP should be reduced has not been determined. Indeed, reducing systolic BP to a level below 110 mm Hg has been reported to deteriorate renal function.3 The optimal BP for renal protection therefore remains to be determined, particularly in elderly hypertensive patients whose renal function is impaired.
A growing body of evidence has been accumulated that proves that antihypertensive therapy provides substantial benefit in reducing the incidence of cardiovascular diseases.4, 5, 6 Furthermore, much attention has been paid to the role of CKD, as several recent studies have demonstrated that CKD is a critical risk factor for the development of cardiovascular disease. A subanalysis of the HOT trial7 showed that elevated serum creatinine is closely associated with an increased incidence of cardiovascular events. Other investigations, including RENAAL8 and HOPE,9 have also reported CKD to be an important determinant of cardiovascular events. In an epidemiological survey in Japan, approximately 10% of the population aged 20 years or older had diminished GFR (<60 ml min−1 per 1.73 m2).10 This observation implies an important problem, namely that Japanese hypertensive patients may be at a greater risk for the development of cardiovascular diseases. Recently, Ninomiya et al.11 demonstrated that CKD is an independent risk factor for the occurrence of cardiovascular disease in the population of Hisayama, a suburban community of Fukuoka city. Their study revealed a critical role for CKD in the development of cardiovascular disease in the community-based Japanese population, although it remains unclear whether this conclusion is applicable to elderly hypertensive patients.
We therefore performed a prospective survey examining the role of hypertension in mediating the progression of CKD in the population used in the Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive patients (JATOS).12 The rationale, design and patient characteristics have already been published,12 and the principal results have been announced.13 This article reports further subanalysis of the JATOS data to clarify the role of antihypertensive therapy in the progression of CKD. Additionally, the link between CKD and the development of cardiovascular events was evaluated.
Methods
Study design
JATOS was a prospective, multicenter, randomized, open-label, two-arm parallel-group comparison study in Japanese elderly hypertensive patients. The study design and protocols have been detailed in a previous publication,12 and the study was registered at the UMIN Clinical Trial Registry (http://www.umin.ac.jp/ctr/index.htm; trial #UMIN000001021). The random assignment, data collection and analyses were performed by the JATOS Central Registration Office. In brief, the main object of the study was to evaluate the role of BP control in the development of cardiovascular diseases during the 2-year observation period. The subjects enrolled (n=4418) were aged 65–85 years and manifested sustained hypertension with systolic BP over 160 mm Hg.13 Patients with severe hypertension (diastolic BP⩾120 mm Hg), secondary hypertension, recent history of stroke, angina pectoris requiring hospitalization, congestive heart failure (New York Heart Association⩾ class II), persistent arrhythmia (for example, atrial fibrillation), dissecting aneurysm, CKD with serum creatinine level ⩾1.5 mg dl−1, poorly controlled diabetes mellitus (DM; fasting blood glucose ⩾200 mg dl−1 or HbA1c⩾8.0%), malignant disease or collagen disease were excluded from the trial. DM and hyperlipidemia were diagnosed in accordance with the guidelines of the Japan Diabetes Society14 and the Japan Atherosclerosis Society,15 respectively. A cardiothoracic ratio >50% on a chest X-ray film was defined as an enlarged heart, and left ventricular hypertrophy was diagnosed based on the Sokolow–Lyon voltage criteria. Progression in New York Heart Association class was deemed as the onset or aggravation of heart failure.
Written informed consent was obtained from all eligible subjects before the run-in period. This trial was performed in compliance with the Declaration of Helsinki. Patients were enrolled from April 2001 to December 2002, and the trial period ended in December 2004. Upon obtaining informed consent, physicians were allowed to give information on patient profiles to the JATOS Central Registration Office, which subsequently assigned the subjects to two systolic BP target arms (strict-treatment group; <140 mm Hg, and mild-treatment group; 140 to <160 mm Hg) by computer-assisted random allocation.12 Antihypertensive therapy with efonidipine (20–60 mg per day), a long-acting Ca channel blocker with renal afferent and efferent arteriolar dilator action,16, 17, 18, 19, 20 was given to all patients, and if the target systolic BP was not achieved, additional antihypertensive agents, including angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, diuretics and β-blockers, were administered.
BP was measured with a sphygmomanometer with the patients in the sitting position at each pre-randomization visit, at randomization visit and at each visit during the follow-up period. Major cardiovascular events constituting primary end points were cerebrovascular disease (cerebral hemorrhage, cerebral infarction, transient ischemic attack, subarachnoid hemorrhage and other types of cerebrovascular disease), cardiac disease (acute myocardial infarction, heart failure, and angina pectoris requiring hospitalization and sudden death), vascular disease (dissecting aneurysms of the aorta and occlusive arterial disease) and renal dysfunction (acute or chronic renal failure and doubling of serum creatinine levels). These events were determined by the Independent Endpoint Evaluation Committee, which was blinded to the treatment assignments. The study was conducted in accordance with the Prospective Randomized Open Blinded End-point method.
Renal function measurement
Serum creatinine values were evaluated in all patients at the pre-randomization visit and every 6 months, and a baseline creatinine concentration above 1.5 mg dl−1 (133 μmol l−1) was considered to be an exclusion criterion. Urinary protein was assessed by the qualitative dipstick method. Estimated glomerular filtration rate (eGFR) was estimated using a modified MDRD formula adapted to the Japanese population, including elderly subjects.10
The effect of antihypertensive therapy on the incidence of cardiovascular events was evaluated on the basis of renal function. Of the two treatment groups, the patients were further stratified by a change in eGFR during the study period (<−20%, −20 to <−10%, −10 to <+10%, +10 to <+20%, ⩾+20%), and the incidence of cardiovascular events was evaluated in each subgroup.
Exploratory analyses
The effects of BP level on cardiovascular events and eGFR were evaluated. The systolic BP values observed at the last two visits were averaged and the subjects were categorized based on these BP levels (that is, <130 mm Hg, 130 to <140 mm Hg, 140 to <150 mm Hg, 150 to <160 mm Hg and ⩾160 mm Hg).
Statistical analysis
Data were expressed as means±s.d. or as proportions. Student's t-test was used to compare continuous variables. Frequency analysis was performed by the χ2 test. Only the time to the first cardiovascular event was considered for the primary end point. Similarly, only the first event in each category was counted for other end points (sudden death, cerebrovascular events, cardiac events or renal events). The effects of the two treatment arms were compared based on the intention-to-treat principle. Incidence proportions were calculated by the Kaplan–Meier method and were compared using the log-rank test. The hazard ratio (HR) and 95% confidence intervals (CIs) for cardiovascular events were estimated using Cox regression analysis. All statistical tests were two-sided and the significance level was set at 5%.
Results
Patient demographics at baseline
Elderly subjects (65–85 years old) with sustained hypertension (systolic BP⩾160 mm Hg) and baseline serum creatinine <1.5 mg dl−1 were enrolled in this trial (n=4418). Upon registration into the trial, the patients were assigned to one of two systolic BP target groups (a strict-treatment group, <140 mm Hg, and a mild-treatment group, 140 to <160 mm Hg). There was no difference in any of the baseline parameters between these two groups (Table 1). The mean number of the antihypertensive drugs given was 1.7 in the strict-treatment group and 1.5 in the mild-treatment group.13
Both groups were further categorized into subgroups with baseline eGFR ⩾ or <60 ml min−1 per 1.73 m2 (Table 1). Systolic BP, diastolic BP and fasting blood glucose did not differ between the strict-treatment and mild-treatment groups with eGFR ⩾60 ml min−1 per 1.73 m2. The prevalence of cardiac enlargement/left ventricular hypertrophy, DM and dyslipidemia was the same between these groups. Likewise, no difference was noted between the strict and the mild groups with eGFR <60 ml min−1 per 1.73 m2 for any of the parameters. When assessed at each subject's final visit, the percentage of efonidipine monotherapy was lower and the use of angiotensin-converting enzyme inhibitors/angiotensin receptor blockers or diuretics was higher in the strict-treatment group than in the mild-treatment group for any eGFR subset (Table 2).
Changes in BP
In the strict-treatment group, systolic and diastolic BP levels were reduced, but 6 months were required to achieve the target BP level (that is, <140 mm Hg, Figure 1a). In the mild-treatment group, systolic BP reached the target BP (that is, 140 to <160 mm Hg) within 3 months and remained within target BP levels throughout the trial period. Likewise, among the subgroup with baseline eGFR ⩾60 ml min−1 per 1.73 m2 and <60 ml min−1 per 1.73 m2, systolic BP in the strict-treatment group was significantly lower than that in the mild-treatment group throughout the trial period (Figures 1b and c).

Temporal changes in blood pressure during the trial. In all patients (a), the subgroup with baseline eGFR ⩾60 ml min−1 per 1.73 m2 (b) and the subgroup with baseline eGFR <60 ml min−1 per 1.73 m2 (c), blood pressure was significantly lower in the strict-treatment group than in the mild-treatment group. **P<0.01 vs. month 0. #P<0.05 vs. strict-treatment group.
Renal outcomes
Renal end points, as assessed by doubling of serum creatinine or end-stage renal disease requiring dialysis therapy, were experienced in eight patients in the strict-treatment group and nine patients in the mild-treatment group (Figure 2). The incidence rate did not differ between these treatment groups (P=0.804). Likewise, the BP control strategy (strict vs. mild treatment) did not affect the incidence of renal events in any of the subgroups with reduced baseline eGFR, DM, male gender, proteinuria at baseline or age over 75 years.

Incidence of renal events in the strict-treatment and mild-treatment groups. The incidence of renal events was evaluated based on several parameters, including eGFR, diabetes, male gender, proteinuria and age. Renal events include end-stage renal disease and doubling of serum creatinine levels.
Changes in eGFR
Figure 3 summarizes the temporal changes in eGFR in the two treatment groups based on various categories. The eGFR was slightly elevated during the trial period, from 59.4 to 62.0 ml min−1 per 1.73 m2 in the strict-treatment group (P<0.0001) and from 58.8 to 61.4 ml min−1 per 1.73 m2 in the mild-treatment group (P<0.0001, Figure 3a, top). There was no difference in eGFR between these two groups at the end of the trial (P=0.3737). Furthermore, in patients with reduced baseline renal function (that is, eGFR<60 ml min−1 per 1.73 m2), there was a greater increase in eGFR, from 48.8 to 55.0 ml min−1 per 1.73 m2 (P<0.0001) in the strict-treatment group and from 48.8 to 54.9 ml min−1 per 1.73 m2 (P<0.0001) in the mild-treatment group (Figure 3b, top).

Temporal changes in eGFR during the trial. Changes in eGFR were evaluated in all patients (a) and those with diminished eGFR (<60 ml min−1 per 1.73 m2, b). The subjects were further divided by systolic blood pressure control categories (strict-treatment group vs. mild-treatment group) or the actual systolic blood pressure achieved at the last two visits (<130 mm Hg, 130 to <140 mm Hg, 140 to <150 mm Hg, 150 to <160 mm Hg, and ⩾160 mm Hg). The effect of blood pressure control on changes in eGFR was evaluated in the subgroups of diabetes (DM) (c), age ⩾75 years (d) and proteinuria (e). *P<0.05, **P<0.01 within trial periods.
We further categorized the subjects based on the actual systolic BP observed at the end of the trial. This analysis revealed that the subgroup that failed to achieve systolic BP below 160 mm Hg manifested no change in eGFR, whereas eGFR was elevated in the remaining categories of patients (Figure 3a, bottom). Similarly, although all BP category groups manifested elevations in eGFR, the subgroup that achieved BP ⩾160 mm Hg exhibited a lower increment in eGFR than the other subgroups (P=0.0021; Figure 3b, bottom).
Patients with DM or proteinuria or those aged ⩾75 years manifested nearly identical changes in eGFR between the two treatment groups (Figures 3c–e). Significant increases in eGFR were observed in patients aged ⩾75 years, whereas no significant change was noted during the treatment period in patients with DM or proteinuria.
The changes in eGFR were further evaluated based on the categorization of the patient profiles (that is, age or presence of DM or proteinuria). eGFR levels were significantly higher in patients <75 years old than in those ⩾75 years old at all points of the treatment period (P<0.0001, Figure 4a) and increased in both age groups during the trial period (<75 years old, P<0.0001; ⩾75 years old, P=0.0003). In patients with DM, eGFR tended to increase, although it did not attain statistical significance (P=0.2550). In subjects with proteinuria, eGFR remained unaltered during the trial period (P=0.3431).

Comparison of temporal changes in eGFR between two subgroups categorized by age, DM or proteinuria. Statistical evaluation was done for all patients (a) and for those with diminished eGFR <60 ml min−1 per 1.73 m2 (b). DM, diabetes.
Among the patients with reduced renal function (that is, baseline eGFR<60 ml min−1 per 1.73 m2), the subgroups of patients aged <75 years and ⩾75 years manifested similar elevations in eGFR (P<0.0001, Figure 4b). Likewise, an increase in eGFR was observed in patients with DM (P=0.0016), but eGFR was unchanged throughout the trial period in patients with proteinuria (P=0.5328). Of interest, eGFR was elevated from 57.7±14.1 to 60.1±16.5 ml min−1 per 1.73 m2 in 215 patients in whom proteinuria disappeared during the trial period. This trend was also observed in the subgroup of patients with baseline eGFR<60 ml min−1 per 1.73 m2 (from 48.7±6.7 to 52.7±13.3 ml min−1 per 1.73 m2, n=133).
Role of CKD in cardiovascular events
Figure 5 shows Kaplan–Meier curves for the incidence of composite cardiovascular events in patients with baseline eGFR<60 and ⩾60 ml min−1 per 1.73 m2. The event rate tended to be greater in patients with baseline eGFR<60 ml min−1 per 1.73 m2 than in those with eGFR⩾60 ml min−1 per 1.73 m2, although the difference did not attain statistical significance (P=0.1723, Figure 5a). When the accumulated event rates were compared between the two treatment groups (that is, mild vs. strict treatment), no difference was noted between the two treatment groups with either baseline eGFR ≥60 (P=0.9553, Figure 5b) or <60 ml min−1 per 1.73 m2 (P=0.9714, Figure 5c). When categorized based on the systolic BP observed at the end of the study, however, the subgroup with systolic BP⩾160 mm Hg carried a higher event rate than other subgroups (P<0.0001, Figures 5d and e).

Cardiovascular event rates in patients with impaired renal function. The cardiovascular event rates in subjects with baseline eGFR <60 ml min−1 per 1.73 m2 were compared with those with eGFR ⩾60 ml min−1 per 1.73 m2 (a). Subjects with preserved (eGFR ⩾60 ml min−1 per 1.73 m2) or impaired renal function (eGFR<60 ml min−1 per 1.73 m2) were further categorized by the target treatment blood pressure (strict treatment vs. mild treatment) (b, c) or the actual blood pressure achieved at the end of the trial (d, e).
Proteinuria at the time of entry into the trial constituted a strong risk predictor of cardiovascular events (P=0.0001), particularly in patients with baseline eGFR<60 ml min−1 per 1.73 m2 (P<0.0001), but not in patients with relatively preserved renal function (Figure 6). The increased risks were attributed primarily to both renal events (HR: 21.95, 95% CI: 2.45–196.30, P=0.006) and cerebrovascular events (HR: 2.10, 95% CI: 1.10–4.00, P=0.024) and marginally to cardiac events (HR: 2.58, 95% CI: 0.97–6.86, P=0.059).

Cardiovascular event rates in patients with proteinuria. The incidence of events was assessed in all patients (a), patients with baseline eGFR⩾60 ml min−1 per 1.73 m2 (b) and patients with baseline eGFR<60 ml min−1 per 1.73 m2 (c). Proteinuria disappeared in 60% of the proteinuric patients at the end of the trial, and the incidence of cardiovascular events was reduced in this subgroup, compared with patients with persistent proteinuria (d).
Among 2366 patients for whom urinalysis data were obtained at both the time of entry and at the end of the study, 15% of the patients had proteinuria upon entry (Figure 6d). Of these patients, proteinuria disappeared in 60% of the subjects; there was no difference in the rate of proteinuria disappearance between the strict-treatment group (61.7%) and the mild-treatment group (59.0%, P=0.6813). In patients without proteinuria at entry, 91% of the patients remained non-proteinuric during the study period. The incidence of cardiovascular events was the highest in patients with sustained proteinuria (7.7%, P=0.0327).
Association between changes in renal function and cardiovascular events
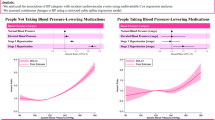
We further assessed the correlation between the incidence of cardiovascular events and changes in eGFR. The observed results were adjusted based on possible confounding factors, including proteinuria and DM at the commencement of the study. The incidence of cardiovascular events increased as the decline rate of eGFR was greater (P=0.0024 in the strict-treatment group, P=0.0002 in the mild-treatment group, Figure 7a). This trend was more pronounced in patients with baseline eGFR<60 ml min−1 per 1.73 m2 (Figure 7c); marked elevations in the event rates were noted in both groups, when eGFR decreased by 20% or more (P=0.0002 in the strict-treatment group and P=0.0001 in the mild-treatment group). When assessed in the whole patient population or in patients with reduced eGFR, no significant difference was observed between the two treatment groups with regard to each category of changes in eGFR. In patients with baseline eGFR⩾60 ml min−1 per 1.73 m2, no significant trend was noted between the changes in eGFR and the incidence of cardiovascular events (Figure 7b).

Effects of the change in eGFR on the incidence of cardiovascular events. Event rates were evaluated based on percent changes in eGFR during the trial period in all patients (a), in patients with baseline eGFR ⩾60 ml min−1 per 1.73 m2 (b) and in patients with baseline eGFR <60 ml min−1 per 1.73 m2 (c).
Discussion
An increasing amount of evidence has shown that inhibition of the renin–angiotensin system constitutes a central strategy for the treatment of CKD.21, 22 Despite extensive investigations that have attempted to alleviate the progression of CKD, no therapeutic modality has been established as a tool that halts the course of CKD in elderly hypertensive patients in whom renal function has declined relentlessly. Furthermore, several recent studies have demonstrated that CKD constitutes a determinant of the development of cardiovascular disease.7, 8, 9, 10 Nevertheless, the extent to which BP should be controlled to minimize the incidence of cardiovascular diseases and to preserve renal function in elderly hypertensive patients has not yet been elucidated.
The JATOS study was designed to clarify the effects of BP levels on cardiovascular events in elderly hypertensive Japanese patients using efonidipine as a baseline antihypertensive drug.12, 13 The present renal subanalysis attempted to elucidate the roles of BP level, age, and the presence of proteinuria or DM in renal function and to evaluate whether baseline renal function or change in eGFR affects the incidence of cardiovascular events. The results showed that the incidence of renal events (that is, doubling of serum creatinine levels or end-stage renal disease) did not differ between the strict-treatment group and the mild-treatment group (Figure 2). The same results were obtained in subgroups of patients with impaired renal function (baseline eGFR<60 ml min−1 per 1.73 m2), DM and proteinuria, and in male patients and those ⩾75 years old. Consistently, the present study showed well-preserved eGFR throughout the trial period and nearly identical temporal changes in eGFR in the two treatment groups (Figure 3). Indeed, the subgroups in which the actual BP fell below 160 mm Hg at the end of the trial manifested similar temporal changes in eGFR. This trial therefore indicates the favorable action of efonidipine-based regimens on renal function in elderly hypertensive patients, and the results are consistent with our previous report suggesting BP-independent protective action of efonidipine.23 In this regard, the MDRD study demonstrated that lowering BP was associated with delayed progression of CKD, particularly when proteinuria exceeded 1 g per day.24 By contrast, the AASK trial indicated that the decline rate of GFR in the usual BP goal group was nearly the same as that in the lower BP goal group.25 These divergent observations may be attributable to several factors, including the age of the participants, the degree of renal function, the amount of proteinuria at baseline, the treatment strategy and the duration of the study.
Aging is associated with a decline in renal function. In the present study, however, we have demonstrated that eGFR is rather elevated in elderly hypertensive patients of both treatment groups during the trial period (Figure 3a), and this tendency is also observed when the baseline eGFR is reduced (that is, <60 ml min−1 per 1.73 m2, Figure 3b). Of more interest, the antihypertensive therapy with the efonidipine-based regimen increased eGFR in patients with impaired renal function who were ⩾75 years old or who suffered from DM (Figure 4b). In this regard, many previous studies have shown that antihypertensive therapy fails to induce sustained elevations in GFR in patients with CKD; GFR declines with long-term treatment with conventional types of Ca channel blockers, as has been shown in several clinical trials, including AASK25 and INSIGHT.26 Indeed, the use of these types of Ca channel blockers in CKD raises concerns because of the potential aggravation of glomerular hypertension, possibly as a result of preferential afferent arteriolar dilation.16 By contrast, novel types of Ca channel blockers, including efonidipine and benidipine, which possess T-type Ca channel blocking activity,27, 28 confer a greater benefit on renal function.23, 29, 30, 31 Of interest, efonidipine possesses renal protective action via efferent arteriolar dilation,17, 18, 19, 20 the inhibition of Rho kinase32 and, possibly, the inhibition of aldosterone activity.33, 34 Our present observations therefore imply a distinct therapeutic applicability of Ca channel blockers in CKD.31, 35
Of note, the present study showed that in patients with proteinuria at baseline, eGFR was lower than in non-proteinuric patients throughout the study period (Figures 4a and b, bottom). These observations are compatible with previous reports showing that proteinuria per se constitutes a risk factor for the development of CKD.36, 37 Nevertheless, the current trial demonstrated that eGFR was maintained at a constant level throughout the study period. Furthermore, in patients whose proteinuria disappeared during the study period, eGFR was actually elevated. It can therefore be surmised that proteinuria constitutes a pivotal target for the treatment of hypertension and that the therapeutic strategy would determine the course of CKD.
Since the recognition of CKD as a deleterious factor regarding the development of cardiovascular events,7, 8, 9 a number of studies have attempted to clarify the roles of several risk factors in this process. The present study, however, failed to demonstrate a critical role of impaired renal function in the development of cardiovascular events, although the event rate tended to be higher in patients with eGFR<60 ml min−1 per 1.73 m2 (P=0.1723, Figure 5a). Furthermore, the event rate did not depend on the target BP levels in the subgroup with preserved or diminished renal function during the 2-year treatment with the efonidipine-based regimen (Figures 5b and c), as long as the achieved BP at the end of the study did not exceed 160 mm Hg (Figures 5d and e). Several reasons may explain the divergent results between our findings and previous observations showing CKD as a cardiovascular risk factor,7, 8, 9 including the observation period, the age of the patients and the use of antihypertensive therapy. As the inclusion criteria for entry into JATOS limited serum creatinine to <1.5 mg dl−1, the small difference in the baseline renal function between these two subgroups may not significantly affect the incidence of cardiovascular events. Further investigations are required to clarify this important issue.
Additional factors affecting the development of cardiovascular disease include the presence of proteinuria. As already reported, proteinuria constitutes an important determinant of cardiovascular disease.38, 39, 40 Concordantly, the present study shows that the incidence of cardiovascular events is higher in patients with proteinuria than in non-proteinuric patients (Figure 6a). Furthermore, although reduced eGFR per se did not elevate the cardiovascular event rate significantly (P=0.1723, Figure 5a), the presence of proteinuria amplified the cardiovascular risk entailed with reduced eGFR (Figure 6c). This result highlights the impact of renal function and proteinuria, that is, the cardiorenal continuum, in elderly hypertensive subjects. Of note, during the trial, proteinuria disappeared in 60% of patients with baseline proteinuria; this group of patients manifested a lower incidence of cardiovascular disease compared with patients with persistent proteinuria (2.8 vs. 7.7%, P=0.0327; Figure 6d). The implication of proteinuria as a therapeutic target is once again emphasized.41
Of interest, the present study shows that the elevated cardiovascular risks associated with proteinuria are not only ascribed to renal events (HR: 21.95, 95% CI: 2.45–196.30, P=0.006), but are also due to cerebrovascular events (HR: 2.10, 95% CI: 1.10–4.00, P=0.024) and marginally to cardiac events (HR: 2.58, 95% CI: 0.97–6.86, P=0.059). Similar findings were observed in the renal subanalysis of the CASE-J study, which showed that CKD is more closely associated with the development of cerebrovascular events than of cardiac events, which is apparent even in the early stage of CKD.40 These observations could reflect the characteristics of Japanese CKD subjects, who are more prone to cerebrovascular events than cardiac events.42
Recent studies have demonstrated that changes in renal function are associated with cardiovascular events. Khan et al.43 reported that the rate of decline in eGFR during the observation period parallels the mortality in patients with left ventricular systolic dysfunction. Recently, Rifkin et al.44 demonstrated that a rapid decline in eGFR is associated with an increased risk of cardiovascular and all-cause mortality in older adults. The present study showed that rate of decrease in eGFR was correlated with the incidence of cardiovascular events in both the strict-treatment and the mild-treatment groups, although there was no difference observed between these groups (Figure 7a). When compared with the patients with baseline eGFR<60 ml min−1 per 1.73 m2, the event rate was markedly elevated in both groups of patients with 20% or greater decreases in eGFR (strict-treatment group, 12.3%; mild-treatment group, 11.8%, Figure 7c). These findings indicate that the rate of decline in renal function determines the incidence of cardiovascular events. Importantly, this tendency is exaggerated when baseline renal function is compromised. Collectively, both baseline function and changes in renal function act in concert to modify cardiovascular insults in elderly hypertensive patients.
In conclusion, the present subanalysis of the JATOS study has demonstrated that antihypertensive therapy with efonidipine-based regimens improves kidney function. Such improvement is observed even in the presence of impaired renal function and appears to be independent of systemic BP. Furthermore, the incidence of cardiovascular events is greater in the subgroup with proteinuria or greater decline in eGFR. These observations offer substantial information on the therapeutic strategy in the treatment of hypertension with regard to renal protection and cardiovascular events in elderly hypertensive patients.
References
Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, Tuttle K, Douglas J, Hsueh W, Sowers J . Preserving renal function in adults with hypertension and diabetes: a consensus approach. National Kidney Foundation Hypertension and Diabetes Executive Committees Working Group. Am J Kidney Dis 2000; 36: 646–661.
Jafar TH, Stark PC, Schmid CH, Landa M, Maschio G, de Jong PE, de Zeeuw D, Shahinfar S, Toto R, Levey AS . Progression of chronic kidney disease: the role of blood pressure control, proteinuria, and angiotensin-converting enzyme inhibition a patient-level meta-analysis. Ann Intern Med 2003; 139: 244–252.
Jafar TH, Schmid CH, Landa M, Giatras I, Toto R, Remuzzi G, Maschio G, Brenner BM, Kamper A, Zucchelli P, Becker G, Himmelmann A, Bannister K, Landais P, Shahinfar S, de Jong PE, de Zeeuw D, Lau J, Levey AS . Angiotensin-converting enzyme inhibitors and progression of nondiabetic renal disease. A meta-analysis of patient-level data. Ann Intern Med 2001; 135: 73–87.
Moser M, Hebert PR . Prevention of disease progression, left ventricular hypertrophy and congestive heart failure in hypertension treatment trials. J Am Coll Cardiol 1996; 27: 1214–1218.
Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, Godwin J, Qizilbash N, Taylor JO, Hennekens CH . Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet 2000; 335: 827–838.
ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002; 288: 2981–2997.
Ruilope LM, Salvetti A, Jamerson K, Hansson L, Warnold I, Wedel H, Zanchetti A . Renal function and intensive lowering of blood pressure in hypertensive participants of the hypertension optimal treatment (HOT) study. J Am Soc Nephrol 2001; 12: 218–225.
Eijkelkamp WB, Zhang Z, Brenner BM, Cooper ME, Devereux RB, Dahlöf B, Ibsen H, Keane WF, Lindholm LH, Olsen MH, Parving HH, Remuzzi G, Shahinfar S, Snapinn SM, Wachtell K, de Zeeuw D . Renal function and risk for cardiovascular events in type 2 diabetic patients with hypertension: the RENAAL and LIFE studies. J Hypertens 2007; 25: 871–876.
Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S . Renal insufficiency as a predictor of cardiovascular outcomes and the impact of ramipril: the HOPE randomized trial. Ann Intern Med 2001; 134: 629–636.
Matsuo S, Imai E, Horio M, Yosuda Y, Tomita K, Nitta K, Yamagata K, Tomino Y, Yokoyama H, Hishida A . Revised equations for estimating glomerular filtration rate (GFR) from serum creatinine in Japan. Am J Kidney Dis 2009; 53: 982–992.
Ninomiya T, Kiyohara Y, Kubo M, Tanizaki Y, Doi Y, Okubo K, Wakugawa Y, Hata J, Oishi Y, Shikata K, Yonemoto K, Hirakata H, Iida M . Chronic kidney disease and cardiovascular disease in a general Japanese population: the Hisayama Study. Kidney Int 2005; 68: 228–236.
JATOS Study Group. The Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS): protocol, patient characteristics, and blood pressure during the first 12 months. Hypertens Res 2005; 28: 513–520.
Ishii M, Goto Y . Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients. Hypertens Res 2008; 31: 2115–2127.
Japan Diabetes Society. Guide for the Treatment of Diabetes Mellitus. Bunkodo: Tokyo, 1999 (in Japanese).
Hata Y, Mabuchi H, Saito Y, Itakura H, Egusa G, Ito H, Teramoto T, Tsushima M, Tada N, Oikawa S, Yamada N, Yamashita S, Sakuma N, Sasaki J . Report of the Japan Atherosclerosis Society (JAS) Guideline for Diagnosis and Treatment of Hyperlipidemia in Japanese adults. J Atheroscler Thromb 2002; 9: 1–27.
Hayashi K, Ozawa Y, Fujiwara K, Wakino S, Kumagai H, Saruta T . Role of actions of calcium antagonists on efferent arterioles -with special references to glomerular hypertension. Am J Nephrol 2003; 23: 229–244.
Hayashi K, Nagahama T, Oka K, Epstein M, Saruta T . Disparate effects of calcium antagonists on renal microcirculation. Hypertens Res 1996; 19: 31–36.
Ozawa Y, Hayashi K, Nagahama T, Fujiwara K, Saruta T . Effect of T-type selective calcium antagonist on renal microcirculation: studies in the isolated perfused hydronephrotic kidney. Hypertension 2001; 38: 343–347.
Arima S, Kohagura K, Xu HL, Sugawara A, Abe T, Satoh F, Takeuchi K, Ito S . Nongenomic vascular action of aldosterone in the glomerular microcirculation. J Am Soc Nephrol 2003; 14: 2255–2263.
Hayashi K, Wakino S, Sugano N, Ozawa Y, Homma K, Saruta T . Ca2+ channel subtypes and pharmacology in the kidney. Circ Res 2007; 100: 342–353.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, Jones DW, Materson BJ, Oparil S, Wright Jr JT, Roccella EJ . The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003; 289: 2560–2572.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagarty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Boudier HA, Zanchetti A . 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: 1462–1536.
Hayashi K, Kumagai H, Saruta T . Effects of efonidipine and ACE inhibitors on proteinuria in human hypertension with renal impairment. Am J Hypertens 2003; 16: 116–122.
Peterson JC, Adler S, Burkanrt JM, Greene T, Hebert LA, Hunsicker LG, King AJ, Klahr S, Massry SG, Seifter JL . Modification of Diet in Renal Disease Study Group: blood pressure control, proteinuria, and the progression of renal disease. Ann Intern Med 1995; 123: 754–762.
Wright Jr JT, Bakris G, Greene T, Agodoa LY, Appel LJ, Charleston J, Cheek D, Douglas-Baltimore JG, Gassman J, Glassock R, Hebert L, Jamerson K, Lewis J, Phillips RA, Toto RD, Middleton JP, Rostand SG . Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: results from the AASK trial. JAMA 2002; 288: 2421–2431.
de Leeuw PW, Ruilope LM, Palmer CR, Brown MJ, Castaigne A, Mancia G, Rosenthal T, Wagener G . Clinical significance of renal function in hypertensive patients at high risk: results from the INSIGHT trial. Arch Intern Med 2004; 164: 2459–2464.
Lee TS, Kaku T, Takebayashi S, Uchino T, Miyamoto S, Hamada T, Perez-Reyes E, Ono K . Actions of mibefradil, efonidipine and nifedipine block of recombinant T- and L-type Ca2+ channels with distinct inhibitory mechanisms. Pharmacology 2006; 78: 11–20.
Furukawa T, Nukada T, Namiki Y, Miyashita Y, Hatsuno K, Ueno Y, Yamakawa T, Isshiki T . Five different profiles of dihydropyridipines in blocking T-type Ca2+ channel subtypes (Cav3.1(α1G), Cav3.2(α1H), and Cav3.3(α1I)) expressed in Xenopus oocytes. Eur J Pharmacol 2009; 613: 100–107.
Fujiwara K, Kanno Y, Hayashi K, Takenaka T, Saruta T . Renal protective effects of efonidipine in partially nephrectomized spontaneously hypertensive rats. Clin Exp Hypertens 1998; 20: 295–312.
Ishimitsu T, Kameda T, Akashiba A, Takahashi T, Ohta S, Yoshii M, Minami J, Ono H, Numabe A, Matsuoka H . Efonidipine reduces proteinuria and plasma aldosterone in patients with chronic glomerulonephritis. Hypertens Res 2007; 30: 621–626.
Omae K, Ogawa T, Nitta K . Influence of T-calcium channel blocker treatment on deterioration of renal function in chronic kidney disease. Heart Vessels 2009; 24: 301–307.
Sugano N, Wakino S, Kanda T, Tatematsu S, Homma K, Yoshioka K, Hasegawa K, Hara Y, Suetsugu Y, Yoshizawa T, Hara Y, Utsunomiya Y, Tokudome G, Hosoya T, Saruta T, Hayashi K . T-type calcium channel blockade as a therapeutic strategy against renal injury in rats with subtotal nephrectomy. Kidney Int 2008; 73: 826–834.
Okayama S, Imagawa K, Naya N, Iwama H, Somekawa S, Kawata H, Horii M, Nakajima T, Uemura S, Saito Y . Blocking T-type Ca2+ channels with efonidipine decreased plasma aldosterone concentration in healthy volunteers. Hypertens Res 2006; 29: 493–497.
Tanaka T, Tsutamoto T, Sakai H, Fujii M, Yamamoto T, Horie M . Comparison of the effects of efonidipine and amlodipine on aldosterone in patients with hypertension. Hypertens Res 2007; 30: 691–697.
Hart P, Bakris GL . Calcium antagonists: do they equally protect against kidney injury? Kidney Int 2008; 73: 795–796.
Iseki K, Ikemiya Y, Iseki C, Takishita S . Proteinuria and the risk of developing end-stage renal disease. Kidney Int 2003; 63: 1468–1474.
Brantsma AH, Bakker SJ, de Zeeuw D, de Jong PE . Extended prognostic value of urinary albumin excretion for cardiovascular events. J Am Soc Nephrol 2008; 19: 1785–1791.
Agrawal B, Berger A, Wolf K, Luft FC . Microalbuminuria screening by reagent strip predicts cardiovascular risk in hypertension. J Hypertens 1996; 14: 223–228.
Kidney Disease Outcomes Quality Initiative (K/DOQI). K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis 2004; 43 (Suppl 1): S1-1–S1-290.
Saruta T, Hayashi K, Ogihara T, Nakao K, Fukui T, Fukiyama K . Effects of candesartan and amlodipine on cardiovascular events in hypertensive patients with chronic kidney disease: subanalysis of the CASE-J study. Hypertens Res 2009; 32: 505–512.
De Zeeuw D, Remuzzi G, Parving HH, Keane WF, Zhang Z, Shahinfar S, Snapinn S, Cooper ME, Mitch WE, Brenner BM . Albuminuria a therapeutic target for cardiovascular protection in type 2 diabetic patients with nephropathy. Circulation 2004; 110: 921–927.
Nakamura K, Okamura T, Hayakawa T, Kadowaki T, Kita Y, Ohnishi H, Saitoh S, Sakata K, Okayama A, Ueshima H . Chronic kidney disease is a risk factor for cardiovascular death in a community-based population in Japan-NIPPON DATA90. Circ J 2006; 70: 954–959.
Khan NA, Ma I, Thompson CR, Humphries K, Salem DN, Sarnak MJ, Levin A . Kidney function and mortality among patients with left ventricular systolic dysfunction. J Am Soc Nephrol 2006; 17: 244–253.
Rifkin DE, Shlipak MG, Katz R, Fried LF, Siscovick D, Chonchol M, Newman AB, Sarnak MJ . Rapid kidney function decline and mortality risk in older adults. Arch Intern Med 2008; 168: 2212–2218.
Acknowledgements
We thank all the investigators and members of the JATOS Data and Safety Monitoring Board for conducting and evaluating JATOS. JATOS was a collaborative study of the Japan Physicians Association and the Japanese Society of Hypertension and was sponsored by Shionogi, Osaka, Japan.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
Drs Saruta, Goto, Ishii and Hayashi report receiving advisory board fees from Shionogi, Osaka, Japan. No other potential conflict of interest relevant to this trial is reported.
Rights and permissions
About this article
Cite this article
Hayashi, K., Saruta, T., Goto, Y. et al. Impact of renal function on cardiovascular events in elderly hypertensive patients treated with efonidipine. Hypertens Res 33, 1211–1220 (2010). https://doi.org/10.1038/hr.2010.162
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2010.162
Keywords
This article is cited by
-
Calcium channel blocker in patients with chronic kidney disease
Clinical and Experimental Nephrology (2022)
-
Going Beyond the Guidelines in Individualising the Use of Antihypertensive Drugs in Older Patients
Drugs & Aging (2019)
-
Multifunctional L/N- and L/T-type calcium channel blockers for kidney protection
Hypertension Research (2015)
-
Combination therapy for hypertension in patients with CKD: a subanalysis of the Combination Therapy of Hypertension to Prevent Cardiovascular Events trial
Hypertension Research (2013)
-
Factors associated with brachial-ankle pulse wave velocity in the general population
Journal of Human Hypertension (2012)
