
Abstract
We investigate the associations of antihypertensive drugs in double and triple combination regimens comprising diuretics and/or β-blockers on the development of new-onset diabetes (NOD). This study was a retrospective cohort study carried out using data from claim forms provided to the central regional branch of the Bureau of National Health Insurance (BNHI) in Taiwan from January 2001 to December 2006. We estimated the odds ratios (ORs) of NOD associated with antihypertensive combination therapy use; non-NOD individuals served as the reference group. A total of 2361 NOD cases were identified among the 12 386 hypertensive patients (6143 men and 6243 women, aged 28–86 years (mean age: 68+11)) during the study period. The risk of NOD was higher after adjusting for age and sex among users of double combinations of diuretics plus β-blockers (adjusted OR, 1.25; 95% confidence interval (CI): 1.12–1.58), diuretics plus calcium channel blockers (CCBs; adjusted OR: 1.14; 95% CI: 1.06–1.26) and β-blockers plus calcium channel blockers (adjusted OR: 1.12; 95% CI: 1.04–1.29) than that among non-users. Patients who took angiotensin-converting enzyme (ACE) inhibitors, or α-blockers as part of a double-drug regimen were at a lower risk of developing NOD than were non-users. Double- or triple-drug combinations comprising angiotensin receptor blockers (ARBs) and vasodilators were not associated with risk of NOD. The results of this study suggest that users of double-drug combination therapies containing diuretics and/or β-blockers and an ACE inhibitor or α-blocker are at a significantly lower risk of developing NOD than are other classes.
Similar content being viewed by others

Introduction
The prevalence of type 2 diabetes mellitus is increasing worldwide. Concerns of new-onset diabetes (NOD) have been raised because of the economic burden it poses in various countries.1, 2 Recently, some multiple prospective trials in hypertension opened a debate about the clinical value of NOD in treated hypertensive patients.3, 4, 5, 6, 7, 8 It seems obvious that cardiovascular risk is higher when diabetes and hypertension coexist than when the two conditions stand alone.9 Therefore, the prevention of diabetes in patients with hypertension is of primary importance.
Combination therapy has been recommended as a potential first-line therapy in clinical practice, especially for higher-risk patients, such as those with stage 2 hypertension.10, 11 First-line ‘old’ classes of antihypertensives, such as diuretics and β-blockers, seem to have deleterious effects on glycemic control, whereas the ‘newer’ agents seem to have either neutral or beneficial effects.12, 13 However, data from these studies, which were designed to address the benefit of a single-drug class in diabetes prevention, did not simultaneously compare all major drug classes. Therefore, we evaluated the effect of antihypertensive combination therapy comprising a diuretic and/or a β-blocker on the development of NOD in patients with hypertension in central Taiwan.
Methods
Study population
Our data were taken from claim forms provided to the central regional branch of the Bureau of National Health Insurance (BNHI) in Taiwan from January 2001 to December 2006. The BHNI stores information from the claim forms in two tables: a visit table and a prescription table. Visit tables contain information regarding patient identification numbers, sex, age, three diagnostic codes, medical expenditures and hospital's and physician's information. The prescription table contains the quantity and expenditure for all drugs, operations and treatments. Patients were included in the study if they had hypertension without diabetes at baseline (1 January 2001). We summarized the claim records of each patient into one record.
Study procedures
We used the International Classification of Diseases, Ninth Revision (ICD-9) Clinical Modification code to define hypertension (ICD-9 codes 401–405) and diabetes (ICD-9 codes 250). Patients with a diagnosis of diabetes and/or patients who had taken antidiabetic drugs between 1 January 1999 and 31 December 2000 were excluded. The primary end point was the development of NOD, which was defined as the first time that a diabetes code or antidiabetic prescription appeared in the outpatient claim records. We identified all prescriptions for antihypertensive drugs administered to patients with and without NOD within a 6-year period before the date on which NOD was diagnosed. In Taiwan, these drugs are available only by prescription. Patients who had used only one type of antihypertensive drug before the date on which NOD was diagnosed were categorized as single users according to the following antihypertensive-drug class that they took: diuretics, α-blockers, β-blockers, calcium channel blockers (CCBs), vasodilators, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs; Table 1). Patients using more than one type of antihypertensive drug before the date on which NOD was diagnosed were categorized as combined users. Patients who had used antihypertensive drugs within the previous 6 years, but not the same drug class continuously before the date on which NOD was diagnosed, were excluded from the analyses. This study was approved by our hospital's ethics committee.
Statistical analysis
Continuous variables are presented as mean+s.d. They were compared by the unpaired Student's t-test. Categorical and discrete variables are presented as frequencies and percentages. When appropriate, they were compared by either Fisher's exact test or by the χ2-test. The probability of developing NOD was determined for each combination antihypertensive group. Adjusted and unadjusted odds ratios (ORs) were estimated using logistic regression analysis. The OR was used to measure the probability of developing NOD. The Wald confidence interval (CI) for OR (θ) was used to define the significant difference under α=0.05. If the CI equals 1.0, it is plausible that the true odds of developing NOD are equal among these drug classes. If it is >1, the probability of developing NOD among patients who took these drug classes is higher than that among patients who did not take those classes of drugs. An OR <1 indicates that the combination drug class has a low probability of being associated with the development of NOD. All analyses were carried out using statistical analysis software, (SAS, version 9.1; SAS Institute Inc., Cary, NC, USA).
Results
Description statistics
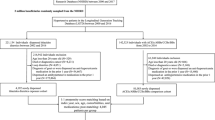
Of the 4 139 245 enrollees included in the database, 12 608 patients were treated with a combination antihypertensive initially. Individuals with a diagnosis of diabetes and/or patients who had taken antidiabetic drugs between 1 January 1999 and 31 December 2000 at baseline (n=42), those treated irregularly, who died or were lost to follow-up (n=180) were excluded. Finally, a total of 12 386 outpatients with hypertension only met the inclusion criteria. Overall, 19.0% (n=2361) of the patients developed NOD; patients ranged in age from 28 to 86 years. The mean age of NOD patients was 67.9 years and that of non-NOD patients was 67.6 years. There were no significant differences in age between these two groups of patients (P=0.24). Men comprised less than half (6143, 49%) of the sample population. Approximately 90% (11 116) of the patients took two drug classes and 10% (1270) took three drug classes (Table 2). More than one-third of the patients (4940, 39%) took CCBs within double- or triple-drug combination therapy regimens with diuretics and/or β-blockers. Only 3% (477) of the patients took ARBs. The distributions of prescription diuretics, α-blockers, ACE inhibitors and vasodilators are shown in Table 2.
Logistic regression results after adjusting for sex and age
Double combination
After adjusting for sex and age, the logistic regression model showed that the risk of developing NOD was lower for individuals who took double-combination therapies comprising diuretics plus α-blockers (OR: 0.85; 95% CI: 0.76–0.96) or diuretics plus ACE inhibitors (OR: 0.86; 95% CI: 0.78–0.94; P<0.05) than that for non-users. Diuretics plus ARBs (adjusted OR: 0.91; 95% CI: 0.78–1.04) and diuretics plus vasodilators (adjusted OR: 0.94; 95% CI: 0.86–1.05) were not associated with an increased risk of NOD (P>0.05). However, diuretics plus β-blockers (adjusted OR: 1.25; 95% CI: 1.12–1.58) and diuretics plus CCBs (adjusted OR: 1.14; 95% CI: 1.06–1.26) had the highest risk estimates of NOD (P<0.05; Table 3).
Risk during the use of double-combination treatments was also estimated for drug classes other than diuretics plus β-blockers. The risk of NOD was significantly higher for patients taking β-blockers plus CCBs (adjusted OR: 1.12; 95% CI: 1.04–1.29) than that for non-users after adjusting for age and sex. β-Blockers plus ARBs (adjusted OR: 0.92; 95% CI: 0.79–1.07) and β-blockers plus vasodilators (adjusted OR: 0.95; 95% CI: 0.86–1.05) were not associated with an increased risk of NOD (P>0.05). However, the risk of developing NOD was significantly lower for patients taking β-blockers plus α-blockers (adjusted OR: 0.86; 95% CI: 0.78–0.97) and for those taking β-blockers plus ACE inhibitors (adjusted OR: 0.87; 95% CI: 0.80–0.96; P<0.05) than that for non-users (Table 3).
Triple combination
Among the triple-combination therapies, the risk of developing NOD was significantly higher for patients taking diuretics plus β-blockers and CCBs (adjusted OR: 1.28; 95% CI: 1.11–1.56) than that for non-users (P<0.05). Although most triple-combination regimens seem to be associated with a trend of increased risk of NOD, our study does not show statistical significance as shown in Table 3.
Discussion
This study suggests that double antihypertensive drug regimens comprising diuretics or β-blockers and ACE inhibitors or α-blockers were independently associated with a decreased risk of developing NOD. However, CCBs were independently associated with an increased risk of NOD. Most triple combinations (diuretics plus β-blockers plus another drug class) were associated with an increased risk of NOD.
In this study, both ACE inhibitors and α-blockers were found to be associated with a low risk of NOD when used in a double-combination therapy that included a diuretic or β-blocker. Numerous studies have consistently suggested that ACE inhibitor and α-blocker classes of antihypertensive medications have differential effects on carbohydrate and lipid metabolism in humans.14, 15 The Captopril Prevention Project was the first controlled clinical trial to suggest that an ACE inhibitor reduces the development of NOD in patients with hypertension.16 Since then, many reports including that of the DREAM trial (the biggest random control trial specifically designed to test the question of whether ACE reduces diabetes risk) have resulted in compatible findings,6, 14, 17 but not STOP-2.18 However, no studies have reported that α-blockers are associated with a reduced risk of NOD in double-combination therapies that include a diuretic or β-blocker. In this study, we found that α-blockers are associated with a decreased risk of NOD.
Some studies have reported that the use of CCBs was independently associated with a decreased risk of NOD in double-combination therapies that include a diuretic or β-blocker.19 In the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT–BPLA) study, it was reported that the relative risk of developing NOD was 30% lower in individuals taking CCB plus a diuretic than that in individuals taking a diuretic plus a β-blocker.17 In contrast to the results of the ASCOT–BPLA study, Padwal and Laupacis12 reported in their study involving 76 176 patients with hypertension that the use of thiazide diuretics, β-blockers, ACE inhibitors and CCB was not associated with NOD. However, the mean length of follow-up in that study was <1 year. Furthermore, their study was an observational community study, and therefore, the results may have lacked the statistical power to show an association between those classes of antihypertensive drugs and NOD.19
Recent studies have suggested that ARBs that interrupt the renin–angiotensin axis are associated with a much lower risk of NOD than are other classes of antihypertensive agents.20, 21 In the Losartan Intervention For Endpoint (LIFE) Study, it was found that ARBs significantly reduced NOD (25%) compared with β-blockers.21 In our study, we found that a diuretic and/or a β-blocker plus an ARB was not associated with NOD; this result is the same as that reported by Bakris et al.22
An important feature of this study was the evaluation of therapies comprising three drug classes (diuretics plus β-blockers plus another drug class) on the risk of developing NOD. Most triple combinations have been reported to accelerate NOD in patients with hypertension.23, 24 Our results are comparable with those reported by Burke et al.,22 who studied the risk of NOD in a cohort of 98 629 patients taking different classes of antihypertensive drugs.24 They found that the adjusted hazard ratio for NOD in individuals taking three or more drug combinations compared with those taking one drug treatment was 1.74 (95% CI: 1.46–2.08).
In conclusion, our findings provide some support for the hypothesis that there are differences in the risk of developing NOD between different antihypertensive drugs. Our results show that patients with hypertension, who take either ACE inhibitors or α-blockers, are at a lower risk of developing NOD than are hypertensive patients who take other classes of antihypertensive drugs in the double-drug combination therapies with diuretics or β-blockers.
Study limitations
Four limitations in this study need to be emphasized. First, this was a retrospective and descriptive study in central Taiwan over a period of 6 years. Moreover, we carried out analyses excluding irregularly treated hypertensive participants (loss to follow-up of >1 month), so caution must be exercised in interpreting our data.
Second, all cases in this study are collected from secondary data of the claim data set of primary care clinics under the central BNHI in Taiwan. We carried out analyses restricted to participants who reported regular follow-up during the study; therefore, it is not clear how our findings can be generalized to patients from different areas.
Third, the risk factors for diabetes, such as obesity, family history, diet and so on are not available in this secondary data. However, those effects could be partly eliminated in a population-based data.
Fourth, this cohort is comprised of hypertensive patients, but they may not be taking these drugs because of hypertension, as there are many other indications for these drugs.
References
Iseki K, Oshiro S, Tozawa M, Ikemiya Y, Fukiyama K, Takishita S . Prevalence and correlates of diabetes mellitus in a screened cohort in Okinawa, Japan. Hypertens Res 2002; 25: 185–190.
Nakayama S, Watada H, Mita T, Ikeda F, Shimizu T, Uchino H, Fujitani Y, Hirose T, Kawamori R . Comparison of effects of olmesartan and telmisartan on blood pressure and metabolic parameters in Japanese early-stage type-2 diabetics with hypertension. Hypertens Res 2008; 31: 7–13.
Rajala U, Qiao Q, Laakso M, Keinänen-Kiukaanniemi S . Antihypertensive drugs as predictors of type 2 diabetes among subjects with impaired glucose tolerance. Diabetes Res Clin Pract 2000; 50: 231–239.
Murayama S, Hirano T, Sakaue T, Okada K, Ikejiri R, Adachi M . Low-dose candesartan cilexetil prevents early kidney damage in type 2 diabetic patients with mildly elevated blood pressure. Hypertens Res 2003; 26: 453–458.
Kudoh T, Nagawaga T, Nakagawa I . Additional small amounts of diuretics improve blood pressure control at low cost without disadvantages in blood sugar metabolism. Hypertens Res 2008; 31: 455–462.
ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002; 288: 2981–2997.
Gress TW, Nieto FJ, Shahar E, Wofford MR, Brancati FL . Hypertension and antihypertensive therapy as risk Factors for type 2 diabetes mellitus. Atherosclerosis risk in communities study. N Engl J Med 2000; 342: 905–912.
Elliott WJ . Differential effects of antihypertensive drugs on new-onset diabetes? Curr Hypertens Report 2005; 7: 249–256.
Campbell NR, McAlister FA, Duong-Hua M, Tu K . Polytherapy with two or more antihypertensive drugs to lower blood pressure in elderly Ontarians. Room for improvement. Can J Cardiol 2007; 23: 783–787.
Saito I, Kobayashi M, Matsushita Y, Mori A, Kawasugi K, Saruta T . Cost-utility analysis of antihypertensive combination therapy in Japan by a Monte Carlo simulation model. Hypertens Res 2008; 31: 455–462.
Smith DH . Fixed-dose combination antihypertensives and reduction in target organ damage: are they all the same? Am J Cardiovas Drug 2007; 7: 413–422.
Padwal R, Laupacis A . Antihypertensive Therapy and incidence of type 2 diabetes: a systematic review. Diabetes Care 2004; 27: 247–255.
Padwal R, Mamdani M, Alter DA, Hux JE, Rothwell DM, Tu K, Laupacis A . Antihypertensive therapy and incidence of type 2 diabetes in an elderly cohort. Diabetes Care 2004; 27: 2458–2463.
Gerstein HC, Yusuf S, Holman R, Bosch J, Pogue J, The DREAM Trial Investigators. Rationale, design and recruitment characteristics of a large, simple international trial of diabetes prevention: the DREAM trial. Diabetologia 2004; 47: 1519–1527.
Lithell HO . Hyperinsulinemia, insulin resistance, and treatment of hypertension. Am J hypertens 1996; 9: 150S–154S.
Hansson L, Lindholm LH, Niskanen L, Lanke J, Hedner T, Niklason A, Luomanmaki K, Dahlof B, de Faire U, Morlin C, Karlberg BE, Wester PO, Bjorck JE . Effect of angiotensin-converting- enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomized trial. Lancet 1999; 353: 611–616.
Dahlöf B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Nieminen M, O'Brien E, Ostergren J, ASCOT Investigators. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366: 895–906.
Hansson L, Lindholm LH, Ekbom T, Dahlof B, Lanke J, Schersten B, Wester PO, Hedner T, de Faire U . Randomised trial of old and new antihypertensive drugs in eldery patients: Cardiovascular mortality and morbidity the Swedish trial on old patients with hypertension-2 study. Lancet 1999; 354: 1751–1756.
Taylor EN, Hu FB, Curhan GC . Antihypertensive medications and the risk of incident type 2 diabetes. Diabetes Care 2006; 29: 1065–1070.
Stump CS, Hamilton MT, Sowers JR . Effect of antihypertensive agents on the development of type 2 diabetes mellitus. Mayo Clin Proc 2006; 6: 796–806.
Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H, LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359: 995–1003.
Bakris G, Molitch M, Hewkin A, Kipnes M, Sarafidis P, Fakouhi K, Bacher P, Sowers J, STAR Investigators. Differences in glucose tolerance between fixed-dose antihypertensive drug combinations in people with metabolic syndrome. Diabetes Care 2006; 29: 2592–2597.
Israili ZH, Lyoussi B, HernAjndez-HernAjndez R, Velasco M . Metabolic syndrome: treatment of hypertensive patients. Am J Ther 2007; 14: 386–402.
Burke TA, Sturkenboom MC, Ohman-Strickland PA, Wentworth CE, Rhoads GG . The effect of antihypertensive drugs and drug combinations on the incidence of new-onset type-2 diabetes mellitus. Pharmacoepi Drug Saf 2007; 16: 979–987.
Acknowledgements
This study was supported by an independent research grant from the Armed Force Taichung General Hospital.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liou, YS., Ma, T., Tien, L. et al. The relationship between antihypertensive combination therapies comprising diuretics and/or β-blockers and the risk of new-onset diabetes: a retrospective longitudinal cohort study. Hypertens Res 32, 496–499 (2009). https://doi.org/10.1038/hr.2009.45
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2009.45
Keywords
This article is cited by
-
Antihypertensive effect of a fixed-dose combination of losartan /hydrochlorothiazide in patients with uncontrolled hypertension: a multicenter study
Clinical and Experimental Nephrology (2012)
-
One-year effectiveness and safety of open-label losartan/hydrochlorothiazide combination therapy in Japanese patients with hypertension uncontrolled with ARBs or ACE inhibitors
Hypertension Research (2010)
