
Abstract
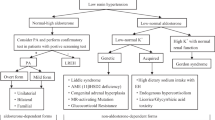
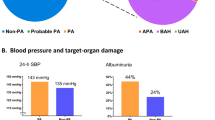
Primary aldosteronism (PA) has been considered a rare cause of hypertension. The introduction of the aldosterone/renin ratio (ARR) as a screening test has led to an increase in the detection rate. The aim of this study was to evaluate the prevalence of PA among unselected hypertensive patients by using an ARR >25 as a screening test. We studied 3,000 consecutive unselected hypertensive patients. Blood samples for the determination of plasma renin activity (PRA), aldosterone (ALD) and electrolytes were drawn in the morning, and patients with an ARR >25 underwent intravenous saline infusion as a confirmatory test. Adrenal CT and a dexamethasone suppression test were performed in patients with confirmed PA. Patients with a positive dexamethasone test underwent genetic testing for glucocorticoid-remediable aldosteronism (GRA). Out of 3,000 hypertensives, 684 (22.8%) showed an ARR >25 and 177 of them (5.9% of the whole population) had a positive saline loading test. Only 44 of them (24.8%) were hypokalemic. CT was performed in all the patients with confirmed PA and 53 of them (29.9%) had a solitary adrenal macroadenoma, 112 (63.3%) had bilateral adrenal enlargement and 12 (6.8%) had normal appearing adrenal glands. Of 177 patients given dexamethasone to identify GRA, 8 (4.5%) showed aldosterone suppression but only one (0.1%) tested positive for the chimeric gene. In conclusion, our findings indicate that standardized application of an ARR >25 to unselected hypertensive patients, followed by i.v. saline loading as a confirmatory test, can result in the detection of a large number of patients with PA (5.9% of the studied population), most of whom are normokalemic. Bilateral adrenal hypertrophy represents the more common form of PA.
Similar content being viewed by others

Article PDF
References
Conn JW : Primary aldosteronism, a new clinical syndrome. J Lab Clin Med 1955; 45: 3–7.
Conn JW : The evolution of primary aldosteronism: 1954–1967. Harvey Lect 1968; 62: 257–291.
Kaplan NM : Commentary on the incidence of primary aldosteronism. Current estimations based on objective data. Arch Intern Med 1969; 123: 152–155.
Berglund G, Andersson O, Wilhemsen L : Prevalence of primary and secondary hypertension: studies in a random population. Br Med J 1976; 2: 554–556.
Tucker R, Labarthe D : Frequency of surgical treatment for hypertension in adults at the Mayo Clinic from 1973 to 1975. Mayo Clin Proc 1977; 52: 549–555.
Hiramatsu K, Yamada T, Yukimura Y, et al: A screening test to identify aldosterone-producing adenoma by measuring renin activity. Results in hypertensive patients. Arch Intern Med 1981; 141: 1589–1593.
Moneva MH, Gomez-Sanchez CE : Establishing a diagnosis of primary aldosteronism. Curr Opin Endocrinol Diabetes 2001; 8: 124–129.
Brown CA, Bouldin MJ, Blackston JW, Duddleston DN, Shepherd JM, Hicks GS : Hyperaldosteronism: the internist's hypertensive disease. Am J Med Sci 2002; 324: 227–231.
Young WF : Minireview: primary aldosteronism—changing concepts in diagnosis and treatment. Endocrinology 2003; 144: 2208–2213.
Kem DC, Weinberger MH, Mayes DM, Nugent CA : Saline suppression of plasma aldosterone in hypertension. Arch Intern Med 1971; 128: 380–386.
Lyons DF, Kem DC, Brown RD, Hanson CS, Carollo ML : Single dose captopril as a diagnostic test for primary aldosteronism. J Clin Endocrinol Metab 1983; 57: 892–896.
Holland O, Brown H, Kuhnert L : Further evaluation of saline infusion for the diagnosis of primary hyperaldosteronism. Hypertension 1984; 6: 717–723.
Castro OL, Yu X, Kem DC : Diagnostic value of the post-captopril test in primary aldosteronism. Hypertension 2002; 39: 935–938.
Young WF : Primary aldosteronism. Management issues. Ann N Y Sci 2002; 970: 61–76.
Gordon RD, Stowasser M, Tunny TJ, Klemm SA, Rutherford JC : High incidence of primary aldosteronism in 199 patients referred with hypertension. Clin Exp Pharmacol Physiol 1994; 21: 315–318.
Loh KC, Koay ES, Khaw MC, Emmanuel SC, Young WF Jr : Prevalence of primary aldosteronism among Asian hypertensive patients in Singapore. J Clin Endocrinol Metab 2000; 85: 2854–2859.
Rayner BL, Opie LH, Davidson JS : Primary hyperaldosteronism: how common is it in patients with severe hypertension? J Hypertens 1999; 17 ( Suppl 3): S177.
Rossi E, Regolisti G, Negro A, Sani C, Davoli S, Perazzoli F : High prevalence of primary aldosteronism using postcaptopril plasma aldosterone to renin ratio as a screening test among Italian hypertensives. Am J Hypertens 2002; 15: 896–902.
Stowasser M, Gordon RD, Gunasekera TG, et al: High rate of detection of primary aldosteronism, including surgically treatable forms, after non-selective screening of hypertensive patients. J Hypertens 2003; 21: 2149–2157.
Mosso L, Carvajal C, Gonzalez A, et al: Primary aldosteronism and hypertensive disease. Hypertension 2003; 42: 161–165.
Mulatero P, Stowasser M, Loh KC, et al: Increased diagnosis of primary aldosteronism, including surgically correctable forms, in Centers from five Continents. J Clin Endocrinol Metab 2004; 89: 1045–1050.
Matsubara M, Sato T, Nishimura T, et al: CYP11B2 polymorphisms and home blood pressure in a population-based cohort in Japanese: the Ohasama study. Hypertens Res 2004; 27: 1–6.
Lifton RP : A chimaeric 11 beta-hydroxylase/aldosterone synthase gene causes glucocorticoid-remediable aldosteronism and human hypertension. Nature 1992; 355: 262–265.
Mulatero P, Morello F, Veglio F : Genetics of primary aldosteronism. J Hypertens 2004; 22: 663–670.
Takeda Y : Genetic alterations in patients with primary aldosteronism. Hypertens Res 2001; 24: 469–474.
Spoto B, Feurlo G, Gervasi A, Bresolin G, Zoccali C : Familial hyperaldosteronism. G Ital Nefrol 2004; 21: 139–143.
Katayama Y, Takata N, Tamura T, et al: A case of primary aldosteronism due to unilateral adrenal hyperplasia. Hypertens Res 2005; 28: 379–384.
Yokota K, Ogura T, Kishida M, et al: Japanese family with glucocorticoid-remediable aldosteronism diagnosed by long-polymerase chain reaction. Hypertens Res 2001; 24: 589–594.
Stowasser M, Gordon RD, Rutherford JC, Nikwan NZ, Daunt N, Slater GJ : Diagnosis and management of primary aldosteronism. J Renin Angiotensin Aldosterone Syst 2001; 2: 156–169.
Seifarth C, Trenkel S, Schobel H, Hahn EG, Hensen J : Influence of antihypertensive medication on aldosterone and renin concentration in the differential diagnosis of essential hypertension and primary aldosteronism. Clin Endocrinol (Oxf) 2002; 57: 457–465.
Mulatero P, Veglio F, Pilon C, et al: Diagnosis of glucocorticoid-remediable aldosteronism in primary aldosteronism: aldosterone response to dexamethasone and long polymerase chain reaction for chimeric gene. J Clin Endocrinol Metab 1998; 83: 2573–2575.
Mulatero P, Curnow KM, Aupetit-Faisant B, et al: Recombinant CYP11B genes encode enzymes that can catalyse conversion of 11-deoxycortisol to cortisol, 18-hydroxycortisol and 18-oxocortisol. J Endocrinol Metab 1998; 83: 3996–4001.
Jonsson JR, Klemm SA, Tunny TJ, Stowasser M, Gordon RD : A new genetic test for familial hyperaldosteronism type I aids in the detection of curable hypertension. Biochem Biophys Res Commun 1995; 207: 565–571.
Omura M, Saito J, Yamaguchi K, Kakuta Y, Nishikawa T : Prospective study on the prevalence of secondary hypertension among hypertensive patients visiting a general outpatient clinic in Japan. Hypertens Res 2004; 27: 193–202.
Tiu SC, Choi CH, Shek CC, et al: The use of aldosterone-renin ratio (ARR) as a diagnostic test for primary hyperaldosteronism and its test characteristics under different conditions of blood sampling. J Clin Endocrinol Metab 2005; 90: 72–78.
Kaplan NM : Primary aldosteronism, in: Kaplan's Clinical Hypertension, 8th ed. Philadelphia, Lippincott Williams & Wilkins 2002, pp 455–479.
Magill SB : Adrenal vein sampling: an overview. Endocrinologist 2001; 11: 357–363.
Yamahara K, Itoh H, Yamamoto A, et al: New diagnostic procedure for primary aldosteronism: adrenal venous sampling under adrenocorticotropic hormone and angiotensin II receptor blocker–application to a case of bilateral multiple adrenal microadenomas. Hypertens Res 2002; 25: 145–152.
Stowasser M : How common is adrenal-based mineralcorticoid hypertension? Curr Opin Endocrinol Diabetes 2000; 7: 143–150.
Lim PO, Jung RT, MacDonald TM : Raised aldosterone to renin ratio predicts antihypertensive efficacy of spironolactone: a prospective cohort follow-up study. Br J Clin Pharmacol 1999; 48: 756–760.
Ganguly A, Chavarri M, Luetscher JA, Dowdy AJ : Transient fall and subsequent return of high aldosterone secretion during continued dexamethasone administration. J Clin Endocrinol Metab 1977; 44: 775–779.
Reincke M, Beuschlein F, Latronico AC, Arlt W, Chrousos G, Allolio B : Expression of adrenocorticotrophic hormone receptor mRNA in human adrenocortical neoplasm: correlation with P450scc expression. Clin Endocrinol 1997; 46: 619–626.
Rossi GP : Remodelling of left ventricle in primary aldosteronism due to Conn's adenoma. Circulation 1997; 95: 1471–1478.
Duprez D, De Buyzere M, Rietzschel ER, Clement DL : Aldosterone and vascular damage. Curr Hypertens Rep 2000; 2: 327–334.
Sato A, Saruta T : Aldosterone-induced organ damage: plasma aldosterone level and inappropriate salt status. Hypertens Res 2004; 27: 303–310.
Iwashima Y, Horio T, Kuroda S, Takishita S, Kawano Y : Influence of plasma aldosterone on left ventricular geometry and diastolic function in treated essential hypertension. Hypertens Res 2002; 25: 49–56.
Kaplan NM : The current epidemic of primary aldosteronism: causes and consequences. J Hypertens 2004; 22: 863–869.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fogari, R., Preti, P., Zoppi, A. et al. Prevalence of Primary Aldosteronism among Unselected Hypertensive Patients: A Prospective Study Based on the Use of an Aldosterone/Renin Ratio above 25 as a Screening Test. Hypertens Res 30, 111–117 (2007). https://doi.org/10.1291/hypres.30.111
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1291/hypres.30.111
