
Abstract
Purpose:
An accurate accounting of persons with Down syndrome (DS) has remained elusive because no population-based registries exist in the United States. The purpose of this study was to estimate this population size by age, race, and ethnicity.
Methods:
We predicted the number of people with DS in different age groups for different calendar years using estimations of the number of live births of children with DS from 1900 onward and constructing DS-specific mortality rates from previous studies.
Results:
We estimate that the number of people with DS living in the United States has grown from 49,923 in 1950 to 206,366 in 2010, which includes 138,019 non-Hispanic whites, 27,141 non-Hispanic blacks, 32,933 Hispanics, 6,747 Asians/Pacific Islanders, and 1,527 American Indians/American Natives. Population prevalence of DS in the United States, as of 2010, was estimated at 6.7 per 10,000 inhabitants (or 1 in 1,499).
Conclusion:
Until 2008, DS was a rare disease. In more recent decades, the population growth of people with DS has leveled off for non-Hispanic whites as a consequence of elective terminations. Changes in childhood survival have impacted the age distribution of people with DS, with more people in their fourth, fifth, and sixth decades of life.
Genet Med 19 4, 439–447.
Similar content being viewed by others


Introduction
Although Down syndrome (DS) is the most common single cause of intellectual disability, an accurate accounting of such persons in the United States has been elusive. Population prevalence data can be helpful in long-term planning for medical and social welfare.1 The best option for obtaining these data would be a well-functioning national registration system of births and deaths of people with disabilities. However, only a few countries have established such systems, including Denmark,1,2 Sweden,3,4 and, to a more limited extent, the United Kingdom and Portugal.5 No population-based registry exists for people with DS in the United States, although the need has been highlighted at national conferences.6,7
In a recent study, de Graaf et al.8 used and validated an alternative approach for the United Kingdom, the Netherlands, and Ireland. In estimating population prevalence, the model uses maternal-age birth data in the general population, maternal age–related chances for a live birth with DS, data regarding elective terminations, and DS-specific mortality rates. Other researchers replicated this approach for England/Wales, with slightly different assumptions.9
In the United States, DS birth prevalence was estimated by de Graaf et al.10 at 12.6 per 10,000 (or 1 in 792) as of 2010. However, only a few studies have estimated US population prevalence. Two previous US studies targeted the age group 0–19 years. For this age group, Shin et al.11 estimated a population prevalence of 10.3 per 10,000 (or 1 in 971) as of 2002. Besser et al.12 estimated 8.3 per 10,000 (or 1 in 1,205) as of 2003. Recently, Presson et al. adopted a strategy related to that of de Graaf et al.8,13 For the period 1909–2007, the number of births of children with DS was estimated based on counts of births by maternal age. Presson et al.13 adjusted for the effect of elective pregnancy terminations by assuming a constant rate of 13% reduction in live births with DS from 1980 to 2007. Additionally, they modeled the survival of people with DS using proportions of deaths by age obtained from death-certificate data from the Centers for Disease Control and Prevention.13 Death-certificate data, however, might be unreliable for modeling the population size of people with DS. According to Presson et al.13, there is underreporting of DS in death certificates. The authors further state that their “life table approach incorrectly assumes that the population size and the age-structure are constant over time.”
In our study, we estimated the population size of DS in the United States by adapting the approach taken by de Graaf et al.,8 modeling survival on the basis of mortality rates derived from historical studies and distinguishing our approach from that of previous researchers ( Table 1 ).
Materials and Methods
Live births
Estimated numbers of live births of children with DS in the United States by year for 1900–2010 were derived from previous work.10
Born after 1983: survival up to 20 years of age
We constructed 1-, 5-, 10-, and 20-year survival rates and interpolated survival between years based on the US survival rates from Kucik et al.14 (Supplementary Materials S1 online).
Born after 1983: survival to more than 20 years of age
For modeling survival beyond 20 years of age after 1983 (and for modeling survival of all ages before 1983), no comprehensive US studies are available. To fill the gap, we adapted the approach taken by de Graaf et al.8 (Supplementary Materials S1 online).
Born before 1983: survival up to 10 years of age
We adapted the approach of de Graaf et al., who used the results from multiple historical studies to estimate 1-, 5-, and 10-year survival rates8 (Supplementary Table S1 online and Supplementary Material S1 online). Figure 1 shows the 1-, 5-, and 10-year survival rates.

Estimates of 1-, 5-, and 10-year survival rates for children with Down syndrome, 1917–2003.
Born before 1983: survival over 10 years of age
For modeling survival beyond 10 years of age, de Graaf et al.8 used data from four studies.15,16,17,18 Wu and Morris9 added two studies.19,20 In our modeling of survival to more than 10 years of age before 1983 (and more than 20 years of age after 1983), we made use of the average of these very similar curves. Like de Graaf et al.,8 we used a more hazardous survival curve based on the previous work of Penrose21 for predicting the survival of cohorts born before 1940 until the calendar year 1950.
Predicting population prevalence
By combining the estimated numbers of births of people with DS in the United States by year with the constructed survival curves (Supplementary Table S2A online and Supplementary Figure S1 online), we estimated the population prevalence and age distribution for each calendar year from 1950 onward.
Predicting nonselective birth prevalence by race/ethnic group
Birth prevalence in the absence of DS-specific terminations of pregnancy (“nonselective birth prevalence”) can be estimated on the basis of maternal-age distribution in the general population by following the strategy described by de Graaf et al.10 (Supplementary Materials S2 online). For the period 1900–2010, we constructed the nonselective number of births of children with DS for five groups: non-Hispanic whites (NHW), non-Hispanic blacks/Africans (NHB), Hispanics (HIS), Asians/Pacific Islanders (AS/PI), and American Indians/American Natives (AI/AN).
Predicting live birth prevalence by race/ethnic group
For the period 1998–2010, the number of live births of children with DS by race/ethnic group can be estimated based on counts in surveillance programs.22,23,24,25,26,27,28,29,30,31,32,33,34 For the period 1969–1997, numbers of live births by ethnic group were extrapolated on the basis of trends in reduction percentages, as constructed by de Graaf et al.10 (Supplementary Materials S2 online).
Estimating survival by race/ethnic group
There is evidence that survival rates for children with DS differ by race/ethnic group.14,35 Previously published data specify 1-year mortality rates by race/ethnic group and by birth cohort (1983–1987; 1988–1992; 1993–1997; 1998–2003).14,36 Combining these data with the data of Wang et al.35 for 1999–2007, we constructed 1-year mortality rates for NHB children with DS in 1985–2003. For the years before 1985 and after 2003, 1-year mortality rates for NHB were extrapolated (Supplementary Materials S3 online).
Survival rates between 1 and 8 years are significantly lower for NHB children with DS than for NHW children with DS.35 There is a significantly lower survival rate for NHB children with DS between 1–5 years and between 5–10 years.14 Therefore, we constructed 5-year and 10-year rates separately for NHB and for all other races combined (Supplementary Materials S3 online). We assumed that beyond the age of 10 years there would be no ethnic differences in survival rates. Finally, we also applied the survival curves for NHB to AI/AN because previous data suggested that 1-year survival for DS is highly similar in these two groups.35
Estimating the number of foreign-born people with DS
Death-certificate data indicate whether the deceased was native- or foreign-born.37 We estimated the number of foreign-born persons with DS by using the proportion of deaths (per birth decade) of foreign-born people with DS for the total number of deaths of people with DS by ethnic group/race; we made use of the last 8 years for which this information was available (1997–2004).
Validation
As a sensitivity analysis, we estimated outcomes for population prevalence if we had followed other assumptions, including those of previous researchers8,9 (Supplementary Materials S7 online). Our current model can be applied to predict the number of deaths of people with DS by age group in different calendar years. As validation, this predicted age distribution was compared with the age distribution of deaths of people with DS in death-certificate data (1968–2010).37
Results
Numbers by age and ethnicity in 2010
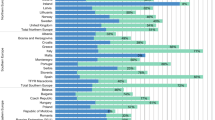
Excluding foreign-born people, the number of people with DS in the United States, as of 2010, was estimated at 199,720, including 136,318 NHW, 26,827 NHB, 29,387 HIS, 5,663 AS/PI, and 1,527 AI/AN ( Figure 2 and Supplementary Materials S4 online). In the absence of elective terminations, these predicted numbers would have been 245,981, including 167,992 NHW, 31,836 NHB, 33,620 HIS, 10,716 AS/PI, and 1,817 AI/AN. This corresponds with reductions in population prevalence related to elective terminations, which are estimated to be 19% for all people with DS, 19% for NHW, 16% for NHB, 13% for HIS, 47% for AS/PI, and 16% for AI/AN.

Estimates of the number of people with Down syndrome in the United States in 2010. The estimates are shown by age for (a) all persons, (b) non-Hispanic whites, (c) non-Hispanic blacks, (d) Hispanics, (e) Asians/Pacific Islanders, and (f) American Indians/American Natives. Because no foreign-born American Indian/American Native children were included in the death-certificate data for 1997–2004, we did not estimate foreign-born children for this group.
For each ethnic group, younger age groups tend to be larger and are most pronounced in HIS and AS/PI, thus reflecting the fast-growing number of births in these ethnic groups, in general, during the past decades. These age differences are largest for HIS. For AS/PI, the estimated number of live births in the younger age groups is considerably reduced by terminations of pregnancies ( Figure 2e ), whereas for HIS the estimated reduction percentages are relatively low ( Figure 2d ).
For most ethnic groups, there is a peak in predicted numbers at approximately 45 years of age consequent to the relatively large estimated numbers of births of children with DS in the 1950s and 1960s (Supplementary Material S2 online) and the improvement in survival for young children with DS (Supplementary Materials S1 and S3 online). For HIS and AS/PI, which are fast-growing immigrant groups, this peak is absent.
Including people born outside of the United States, our estimation of people with DS in the United States is 206,366, including 138,019 NHW, 27,141 NHB, 32,933 HIS, 6,747 AS/PI, and 1,527 AI/AN. Since the 1950s, a few people with DS immigrated into the United States ( Figure 2a ). They were predominantly HIS and AS/PI, and most were born in the 1970s and 1980s ( Figures 2d , e ).
For each ethnic group, including HIS and AS/PI, immigration of people with DS has had only a limited effect on the total predicted number of people with DS ( Figure 2 ). However, as a result of immigration, the estimated numbers of births in the HIS and AS/PI groups, many of whom are young people in their fertile years, have increased rapidly over recent decades.
Historical development in numbers
The number of people with DS (including foreign-born) has shown a linear growth from an estimated 49,923 in 1950 to 206,366 in 2010 ( Figure 3a ). Growth has also been more or less linear for the NHB ( Figure 3c ) and AI/AN ( Figure 3f ) groups. Growth for NHW was linear between 1950 and 1975 but has leveled off in recent decades, mainly as a consequence of elective terminations. For HIS and AS/PI, the growth pattern is exponential ( Figure 3d , e ) because these two ethnic groups consist of many young people in their fertile years. For AS/PI, this exponential pattern would have been even stronger in the absence of the high estimated number of elective terminations in recent decades ( Figure 2e ).

Estimates of the number of people with Down syndrome in the United States, 1950–2010. Estimates are shown by age for (a) all persons, (b) non-Hispanic whites, (c) non-Hispanic blacks, (d) Hispanics, (e) Asians/Pacific Islanders, and (f) American Indians/American Natives.
Changes in childhood survival have had a substantial impact on the age distribution of people with DS (Supplementary Materials S5 online). In 1950, only an estimated 27% were older than 20 years of age and 4% were older than 40 years compared with 57 and 28%, respectively, in 2010. However, for HIS and AS/PI—both of which are immigrant groups with many young people—these latter estimated percentages are lower. As of 2010, the percentages for HIS were 39 and 12% and those for AS/PI were 42 and 11%, respectively.
Population prevalence
Population prevalence of DS in the United States as of 2010 was estimated at 6.7 per 10,000 inhabitants (or 1 in 1,499). If only native-born people were included in the numerator and denominator, then population prevalence would be estimated at approximately 7.5 per 10,000 (or 1 in 1,328). In each ethnic group, the estimated population prevalence for foreign-born people is much lower, between 1 or 2 per 10,000 (Supplementary Materials S6 online). In NHW, NHB, and AI/AN, the population prevalence including only native-born people (in the numerator and denominator) leads to slightly higher estimations of that population prevalence than those including both native- and foreign-born people. However, for HIS and AS/PI, this difference is large because the denominator is strongly influenced by excluding foreign-born people. For HIS, the population prevalence (as of 2010) including foreign- and native-born people is estimated at 6.5 per 10,000 (or 1 in 1,540); when only native-born people are included, it is estimated at 9.8 per 10,000 (or 1 in 1,020). For AS/PI, the corresponding values are an estimated 4.1 per 10,000 (1 in 2,410) and 10.1 per 10,000 (1 in 994), respectively. The values including only native-born people are relatively high for HIS and AS/PI because these immigrant groups consist of many relatively young people in their fertile years.
Using Integrated Public Use Microdata Series–USA estimates for population size,38 including both native- and foreign-born people (in numerator and denominator), the total population prevalence of DS is estimated at approximately 12.7 per 10,000 (1 in 790) for 0- to 4-year-olds and decreases with age to an estimated 8.6 per 10,000 (1 in 1,169) for 20- to 24-year-olds, 6.4 per 10.000 (1 in 1,567) for 30- to 39-year-olds, 1.9 per 10,000 (1 in 5,273) for 60- to 69-year-olds, and to less than 0.1 per 10,000 (1 in 122,364) for those older than 80 years (Supplementary Materials S6 online). Population prevalence for adults 18 years of age and older is estimated at approximately 5.3 per 10,000 (1 in 1,875; corresponding to a total estimate of 125,461 persons) in 2010. Including both native- and foreign-born people (in the numerator and denominator), the population prevalence for HIS and AS/PI seems to be lower than that for other ethnic groups, especially for those between 20 and 60 years of age. For HIS groups born before 1985 and for AS/PI groups born before 1995, excluding foreign-born people (from the numerator and denominator) makes a huge difference, leading to estimates 1.5 to 6 times higher and to values of population prevalence by age group that are much more similar to those for other ethnicities.
Historical development in population prevalence
Before 1970, the United Kingdom appeared to have a slightly lower estimated population prevalence in the absence of terminations than did the United States; however, this was reversed after 1980 (Supplementary Materials S6 online). In comparison to the United States, the effect of elective terminations on population prevalence in the United Kingdom has been more pronounced in recent years. In the United States, in 1995, there were an estimated 8% fewer people with DS than there would have been without elective terminations, and this value increased to approximately 19% in 2010. In the United Kingdom, the corresponding estimated values were 10 and 26%, respectively. As a result, the modeled DS population prevalence is approximately 6.7 per 10,000 in the United States (1 in 1,499) and 6.4 per 10,000 in the United Kingdom (1 in 1,553) as of 2010. In comparison, historically and currently, the Netherlands has considerably higher estimated population prevalence in the absence of elective terminations. The impact of elective terminations on population prevalence is similar to that in the United States, rising from an estimated 5% fewer people with DS as a result of elective terminations in 1995 to 15% as of 2010. The population prevalence of DS in the Netherlands was estimated at approximately 8.2 per 10,000 (1 in 1,223) as of 2010.
Sensitivity analysis and validation
We compared the results of our current model with the results of survival modeled according to the models by de Graaf et al.8 and Wu and Morris,9 respectively (Supplementary Materials S7 online). Our current model estimated the total number of people with DS (excluding foreign-born people with DS) to be 199,720. The model by de Graaf et al.8 estimated that number to be 192,456 (4% lower), and Wu and Morris’s model9 estimated 205,089 (3% higher). The age distributions are slightly different. In the age range of 0–20, the model by de Graaf et al. predicts higher numbers than the current model8 and the model by Wu and Morris predicts lower numbers.9 However, between ages 25 and 59 years, this pattern reverses. For those more than 60 years of age, both alternative models predict lower numbers than the current model does.
In Supplementary Materials S7 online, the age distribution at death of people with DS, as predicted by the three models, is compared with the age distribution of people with DS in the death-certificate data (1986–2010)37 by comparing the mean, 25th, 50th, and 75th percentiles of these distributions for the corresponding calendar years.
Discussion
Previously, Presson et al.13 predicted the best estimate of native-born people with DS in the United States to be 250,700. Our estimates are considerably lower at 206,366 (which includes people born outside the United States) and 199,720 (which excludes those individuals). Up to 20 years of age, model differences can be explained mainly by the input of different live birth numbers. For recent years, we based our estimates on counts in surveillance programs, whereas Presson et al.13 estimated the number of expected births in the absence of terminations, and adjusted these by an assumed rate of 13% reduction from 1980 onward. For ages more than 30 years, as a result of using different survival curves, our model predicts considerably lower numbers than Presson et al did. Both models predict a peak at approximately 45 years of age. However, in the work by Presson et al., this peak occurs for approximately 4,600 people; in our model, it occurs for approximately 3,200 (30% lower). In summary, the models differ in both total number and estimates for specific age groups.
De Graaf et al.10 previously demonstrated that systematic changes of some input variables had only limited outcome effects on the constructed birth rates. Regarding survival rates, we compared the results of our current model with those of two alternatives: those of de Graaf et al. and those of Wu and Morris (Supplementary Materials S7 online).8,9 Prediction of the total number of people with DS is only slightly different; however, there are differences in the predicted age distribution. As validation, we compared the age distribution at death for people with DS as predicted by these models with this age distribution in the death-certificate data (Supplementary Material S7 online).37 Our current model has a better fit than both alternatives. In addition, our current model also fits very well with the age distribution in the death-certificate data, if analyzed in detail (Supplementary Figure S7C online) or by ethnic group (Supplementary Figure S7D online).
Without a valid estimate of DS population size by age group, it is impossible to construct reliable survival rates on the basis of death-certificate data. Presson et al.13 circumvented this problem by assuming a constant size of the birth cohorts of children with DS over time—and a constant rate of childhood survival—thus constructing an approximation with the same survival curve for each year of birth. By contrast, we constructed both population size by age and differential survival curves for each year of birth using other sources of information ( Table 1 ). Subsequently, our model was used to predict the age distribution at death for people with DS, which as a validation was compared with the actual age distribution in the death-certificate data, assuming that underreporting of DS is similar for different age groups. This last assumption might not be entirely true; however, the close fit in age distribution at death between our model and the death-certificate data seems to support the notion that these two approaches validate each other.
DS has changed from a predominantly childhood disability in the 1950s, with only an estimated 27% older than 20 years of age and 4% older than 40 years, to a disability that also affects many people in older age groups. As of 2010, approximately 57% were older than 20 years and an estimated 28% older than 40 years. However, for HIS and AS/PI, both of which are fast-growing immigrant groups with many young people, these latter percentages are lower. The substantial growth in the number of adults and elderly people with DS living in the United States indicates the importance of advocating adult- and senior-specific services and research.
In contrast to the work by Presson et al.,13 our study offers a detailed picture of the changing ethnic composition of the population of people with DS. For each ethnic group, the direct effect of immigration of people with DS is small. However, as a result of immigration of many HIS and AS/PI people in their fertile years, the estimated number of births (of children with and without DS) in these two groups has increased substantially in recent decades. Consequently, the estimated percentage of young HIS and AS/PI people with DS has increased, whereas the percentage of young NHW people with DS has decreased (Supplementary Figure S4B online), mainly reflecting the change in the ethnic composition of the United States, in general, and—to a lesser extent—ethnic differences regarding elective terminations. We consider it important to differentiate between ethnic groups because our model negates the, perhaps, “easy” assumption that population prevalence by age group will be more or less similar for all ethnic groups.
As a consequence of elective terminations, the (native-born) population of DS had been reduced by an estimated 19% as of 2010. This effect is lower than that in the United Kingdom (26%) and slightly higher than in the Netherlands (15%). Although the effect of elective terminations on the number of people with DS in the US population is limited, large ethnic differences exist. The reduction of the number of (native-born) people with DS, consequent to elective terminations, is as low as an estimated 13% for HIS and as high as an estimated 47% for AS/PI, reflecting the large ethnic differences in reduction percentages of births in recent decades, as explored by de Graaf et al.10 Noninvasive prenatal screening with cell-free DNA was introduced in the United States at the end of 2011; it remains an open question how many more elective terminations will result from expanded prenatal diagnoses.
The historical changes in age distribution in the DS population are due in part to longer adulthood survival after 1950. However, the most substantial explanation is the ever-increasing survival of young children with DS over the past 100 years. This has led to increasing mean and median life expectancy rates, which have risen from an estimated 26 years (mean) and 4 years (median) in 1950 to 53 years (mean) and 58 years (median) in 2010 (Supplementary Figure S3B online). There are also some ethnic differences in life expectancy. For NHB (and AI/AN), estimates of mean and median life expectancy were slightly lower, at 22 and 2 years, respectively, in 1950 and 50 and 57 years in 2010.
Importantly, there is a difference between “life expectancy” and “mean age of death.” Life expectancy is the prediction of how many years a person born in a specific year will probably live, whereas mean age of death is the average age of death in the calendar year under observation. Mean age of death is strongly influenced by the age distribution of people living in the specific population, which is a result of the relative sizes of birth cohorts and of historical childhood survival rates within these cohorts. According to our model, the mean and median age of death also increased, and even more rapidly, from an estimated 3 and 0 years, respectively, in 1950 to 12 and 2 years in 1970 to 35 and 38 years in 1990 to 48 and 54 years in 2010 (Supplementary Figure S7B–D online), similar to the rapid changes in age of death found in death certificates by Yang et al.39 and Presson et al.13 for the United States and by Englund et al.40 for Sweden.
In comparison to the differences in life expectancy, ethnic differences in age of death are much more pronounced (Supplementary Figure S7D online) because this construct is influenced not only by differences in age-specific survival at that moment of time but also by the age distribution of the living population. Therefore, the substantial differences in the historical development of age of death by ethnicity, as found in the death certificates37 by other researchers,39 only partly reflect real differences in survival rates at the time.
One important consequence of our results is the identification of DS as a rare disease according to the definition of the Rare Diseases Act of 2002. Including foreign-born people, estimations up to 2008 were less than 200,000. Excluding foreign-born people, estimations for all years were less than 200,000. Furthermore, DS is no longer a childhood disability. Within the United States, there are many adults with DS and the estimated median life expectancy is now approaching 58 years.
Disclosure
B.G.S. serves in a nonpaid capacity on the board of directors or scientific advisory boards for the Massachusetts Down Syndrome Congress, the Band of Angels Foundation, and the National Center for Prenatal and Postnatal Down Syndrome Resources (all nonprofit organizations). B.G.S. is codirector of the Massachusetts General Hospital Down Syndrome Program and occasionally gets remunerated by Down syndrome nonprofit organizations for speaking engagements about Down syndrome. He receives support for clinical drug trials involving people with Down syndrome from Hoffmann–La Roche, Inc. He has a sister with Down syndrome. G.G. works for the Dutch Down Syndrome Foundation, a nonprofit organization. He had a daughter with Down syndrome who passed away in 2005 at the age of 15. F.B. works for Down Syndrome Education International and Down Syndrome Education USA. The charities receive donations and grants from individuals and organizations to conduct research and develop resources and services to improve early intervention and education for children with Down syndrome. He also serves in an unpaid capacity as vice president of the European Down Syndrome Association and as member of the Professional Advisory Committee of the US National Center for Prenatal and Postnatal Down Syndrome Resources. He has a sister with Down syndrome. The other authors declare no conflict of interest.
References
Nguyen-Nielsen M, Svensson E, Vogel I, Ehrenstein V, Sunde L. Existing data sources for clinical epidemiology: Danish registries for studies of medical genetic diseases. Clin Epidemiol 2013;5:249–262.
Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol 2014;29:541–549.
Cnattingius S, Ericson A, Gunnarskog J, Källén B. A quality study of a medical birth registry. Scand J Soc Med 1990;18:143–148.
Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health 2011;11:450.
Sousa P, Bazeley M, Johansson S, Wijk H. The use of national registries data in three European countries in order to improve health care quality. Int J Health Care Qual Assur Inc Leadersh Health Serv 2006;19:551–560.
Oster-Granite ML, Parisi MA, Abbeduto L, et al. Down syndrome: national conference on patient registries, research databases, and biobanks. Mol Genet Metab 2011;104:13–22.
Rasmussen SA, Whitehead N, Collier SA, Frías JL. Setting a public health research agenda for Down syndrome: summary of a meeting sponsored by the Centers for Disease Control and Prevention and the National Down Syndrome Society. Am J Med Genet A 2008;146A:2998–3010.
de Graaf G, Vis JC, Haveman M, et al. Assessment of prevalence of persons with Down syndrome: a theory-based demographic model. J Appl Res Intellect Disabil 2011;24:247–262.
Wu J, Morris JK. The population prevalence of Down’s syndrome in England and Wales in 2011. Eur J Hum Genet 2013;21:1016–1019.
de Graaf G, Buckley F, Skotko BG. Estimates of the live births, natural losses, and elective terminations with Down syndrome in the United States. Am J Med Genet A 2015;167A:756–767.
Shin M, Besser LM, Kucik JE, Lu C, Siffel C, Correa A ; Congenital Anomaly Multistate Prevalence and Survival Collaborative. Prevalence of Down syndrome among children and adolescents in 10 regions of the United States. Pediatrics 2009;124:1565–1571.
Besser LM, Shin M, Kucik JE, Correa A. Prevalence of down syndrome among children and adolescents in metropolitan Atlanta. Birth Defects Res A Clin Mol Teratol 2007;79:765–774.
Presson AP, Partyka G, Jensen KM, et al. Current estimate of Down syndrome population prevalence in the United States. J Pediatr 2013;163:1163–1168.
Kucik JE, Shin M, Siffel C, Marengo L, Correa A ; Congenital Anomaly Multistate Prevalence and Survival Collaborative. Trends in survival among children with Down syndrome in 10 regions of the United States. Pediatrics 2013;131:e27–e36.
Glasson EJ, Sullivan SG, Hussain R, Petterson BA, Montgomery PD, Bittles AH. The changing survival profile of people with Down’s syndrome: implications for genetic counselling. Clin Genet 2002;62:390–393.
Maaskant MA. Mental handicap and ageing. Maastricht University, Dwingeloo, Kavanah; 1993.
Baird PA, Sadovnick AD. Life expectancy in Down syndrome. J Pediatr 1987;110:849–854.
Dupont A, Vaeth M, Videbech P. Mortality and life expectancy of Down’s syndrome in Denmark. J Ment Defic Res 1986;30 (Pt 2):111–120.
Day SM, Strauss DJ, Shavelle RM, Reynolds RJ. Mortality and causes of death in persons with Down syndrome in California. Dev Med Child Neurol 2005;47:171–176.
Tennant PW, Pearce MS, Bythell M, Rankin J. 20-year survival of children born with congenital anomalies: a population-based study. Lancet 2010;375:649–656.
Penrose LS. The incidence of mongolism in the general population. J Ment Sci 1949;95:685–688.
Birth defects surveillance data from selected states, 1996–2000. Birth Defects Res A Clin Mol Teratol 2003;67:729–818.
Birth defects surveillance data from selected states, 1997–2001. Birth Defects Res A Clin Mol Teratol 2004;70:677–771.
Birth defects surveillance data from selected states, 1998–2002. Birth Defects Res A Clin Mol Teratol 2005;73:758–853.
National Center on Birth Defects and Developmental Disabilities, Centers for Disease Control and Prevention. Birth defects surveillance data from selected states, 1999–2003. Birth Defects Res A Clin Mol Teratol 2006;76:894–960.
Population-based birth defects surveillance data from selected states, 2000–2004. Birth Defects Res A Clin Mol Teratol 2007;79:874–942.
Population-based birth defects surveillance data from selected states, 2001–2005. Birth Defects Res A Clin Mol Teratol 2008;82:831–961.
Population-based birth defects surveillance data from selected states, 2002–2006. Birth Defects Res A Clin Mol Teratol 2009;85:939–1055.
Selected birth defects data from population-based birth defects surveillance programs in the United States, 2003–2007. Birth Defects Res A Clin Mol Teratol 2010;88:1062–1174.
National Birth Defects Prevention Network. Selected birth defects data from population-based birth defects surveillance programs in the United States, 2004–2008. Birth Defects Research (Part A) 2011;91:1028–1149.
National Birth Defects Prevention Network. Major birth defects data from population-based birth defects surveillance programs in the United States, 2005–2009. http://www.nbdpn.org/annual_reports.php. Accessed 5 February 2015.
National Birth Defects Prevention Network. Major birth defects data from population-based birth defects surveillance programs in the United States, 2006–2010. http://www.nbdpn.org/annual_reports.php. Accessed 5 February 2015.
National Birth Defects Prevention Network. Major birth defects data from population-based birth defects surveillance programs in the United States, 2007–2011. http://www.nbdpn.org/annual_reports.php. Accessed 9 February 2015.
National Birth Defects Prevention Network. Major birth defects data from population-based birth defects surveillance programs in the United States, 2008–2012. http://www.nbdpn.org/annual_reports.php. Accessed 9 February 2015.
Wang Y, Liu G, Canfield MA, et al.; National Birth Defects Prevention Network. Racial/ethnic differences in survival of United States children with birth defects: a population-based study. J Pediatr 2015;166:819–26.e1.
Centers for Disease Control and Prevention. Key findings: trends in survival among children with Down syndrome in 10 regions of the US. http://www.cdc.gov/ncbddd/birthdefects/features/keyfindings-ds-survival.html. Accessed 28 July 2015.
National Center for Health Statistics, Centers for Disease Control and Prevention. Mortality data—vital statistics NCHS’ multiple cause of death data, 1968–2010. Compressed Mortality Files, as compiled by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. http://www.nber.org/data/vital-statistics-mortality-data-multiple-cause-of-death.html. Accessed 15 February 2015.
Ruggles S, Genadek K, Goeken R, Grover J, Sobek M. Integrated Public Use Microdata Series: Version 6.0. Machine-readable database. 2015.
Yang Q, Rasmussen SA, Friedman JM. Mortality associated with Down’s syndrome in the USA from 1983 to 1997: a population-based study. Lancet 2002;359:1019–1025.
Englund A, Jonsson B, Zander CS, Gustafsson J, Annerén G. Changes in mortality and causes of death in the Swedish Down syndrome population. Am J Med Genet A 2013;161A:642–649.
Author information
Authors and Affiliations
Corresponding author
Supplementary information
Supplementary Materials
(DOCX 1531 kb)
Rights and permissions
About this article

Cite this article
de Graaf, G., Buckley, F. & Skotko, B. Estimation of the number of people with Down syndrome in the United States. Genet Med 19, 439–447 (2017). https://doi.org/10.1038/gim.2016.127
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/gim.2016.127
Keywords
This article is cited by
-
The detailed profile of congenital heart diseases in 254 children with Down syndrome in Saudi Arabia
The Cardiothoracic Surgeon (2024)
-
Characterization of autoimmune eye disease in association with Down’s syndrome
Eye (2024)
-
Understanding the genetic mechanisms and cognitive impairments in Down syndrome: towards a holistic approach
Journal of Neurology (2024)
-
Integration of ATAC-seq and RNA-seq identifies MX1-mediated AP-1 transcriptional regulation as a therapeutic target for Down syndrome
Biological Research (2023)
-
The association between cardiovascular health and cognition in adults with Down syndrome
Journal of Neurodevelopmental Disorders (2023)
