
Abstract
Purpose:
Neurofibromatosis type 1 has been linked to several neurological conditions, including epilepsy, Parkinson disease, headache, multiple sclerosis, and sleep disturbances, predominantly through case reports and patient series that lack comparison groups. Our objective was to assess whether specific neurological conditions occur more frequently in individuals with neurofibromatosis type 1 versus those without neurofibromatosis type 1.
Methods:
We used the 2006–2010 MarketScan Commercial Claims and Encounters database to examine associations between neurological conditions and neurofibromatosis type 1. The neurofibromatosis type 1 group was identified through ≥2 International Classification of Diseases, Ninth Revision, Clinical Modification neurofibromatosis codes (237.70, 237.71) occurring ≥30 days apart or one inpatient neurofibromatosis code. A nonneurofibromatosis type 1 comparison group was frequency matched to the neurofibromatosis type 1 group on age and enrollment length at a 10:1 ratio. Unconditional logistic regression was employed to calculate adjusted odds ratios and 95% confidence intervals for associations between neurofibromatosis and neurological conditions.
Results:
Compared with the nonneurofibromatosis type 1 group (n = 85,790), the neurofibromatosis type 1 group (n = 8,579) had significantly higher odds of health insurance claims for epilepsy (odds ratio: 7.3; 95% confidence interval: 6.4–8.3), Parkinson disease (odds ratio: 3.1; 95% confidence interval: 1.3–7.5), headache (odds ratio: 2.9; 95% confidence interval: 2.6–3.1), multiple sclerosis (odds ratio: 1.9; 95% confidence interval: 1.2–2.9), and sleep disturbances/disorder (odds ratio: 1.4; 95% confidence interval: 1.2–3.6).
Conclusion:
This large study provides strong evidence for positive associations between several neurological conditions and neurofibromatosis type 1.
Genet Med advance online publication 05 June 2014
Similar content being viewed by others


Introduction
Neurofibromatosis type 1 (NF1) is one of the most common autosomal dominant genetic disorders, with an estimated birth prevalence of 1 in 3,000 (ref. 1). Although individuals with NF1 are prone to the development of both benign and malignant nervous system tumors, numerous nonmalignant neurological conditions, including learning disabilities2 and attention deficits,2,3,4,5 have been reported to occur more frequently in individuals with NF1. In addition, NF1 has been linked to other chronic neurological problems, including epilepsy,6,7,8,9 sleep disorders,10,11,12 multiple sclerosis (MS),13,14,15,16,17 headaches,18,19 and Parkinson disease (PD).20,21 Most of the latter NF1 associations are derived from case reports and small patient series that are limited by the lack of a non-NF1 comparison group that is needed to assess whether the complications observed in NF1 occur at significantly higher frequencies than in the general population or whether they represent random co-occurrences.
To identify potential associations between NF1 and several chronic neurological conditions in a large population of individuals, we employed administrative claims data from the Truven Health Analytics MarketScan Commercial Claims and Encounters database.22 This database includes deidentified health insurance claims from 88 million Americans from 2006 to 2010, allowing information to be assembled on the health care of thousands of individuals with and without NF1. Using this unique epidemiologic resource, we identified an NF1 group and a comparison group without NF1 to perform the first large-scale study to assess whether specific chronic neurological conditions in individuals with NF1 occur more frequently than in individuals without NF1.
Materials and Methods
Data source
The study data set was assembled from the Truven Health Analytics MarketScan Commercial Claims and Encounters database, which includes deidentified patient-level claims data for health-care encounters of privately insured individuals from 2006 to 2010. The MarketScan database is the largest claims database and represents “real-world” health-care encounters of the privately insured US population.22 Variables available through MarketScan include demographic data (sex and birth year), enrollment dates, dates of specific claims, three-digit zip codes, patient age, and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes for health-care claims. Race/ethnicity information cannot be obtained using MarketScan data. The database differentiates between inpatient and outpatient claims, and between facility and professional claims, and includes information on health-care plan type to identify capitated plans (from health maintenance organizations). All individuals in the commercial database are privately insured, and they are covered by dozens of different health plans across the United States.
Study population
The NF1 cohort was defined using two ICD-9-CM23 diagnosis codes specific for neurofibromatosis (NF1; 237.71) or NF unspecified (237.70). Patients with claims for the ICD-9-CM code 237.72 (neurofibromatosis type 2 (NF2)) were excluded from the study. Subjects were required to have at least two outpatient claims ≥30 days apart or one inpatient claim for the NF ICD-9-CM codes (237.70 or 237.71) to be included in the NF1 cohort. A non-NF1 cohort of individuals was selected from individuals without any ICD-9-CM diagnosis codes for NF (237.70, 237.71, or 237.72). The non-NF1 comparison group was frequency matched to the NF1 group at a 10:1 ratio by 1-year age group on 1 January 2006, or date of first enrollment if born after 1 January 2006, and by enrollment length in months. Specifically, the sample of NF1 patients and the pool of potential control patients were divided into five subgroups based on 12-month periods of total health insurance enrollment in the database. Within each subgroup of enrollment duration for potential controls, we randomly selected 10 patients without replacement so that the age distribution within the control subgroup matched that of the corresponding NF1 subgroup. We matched by enrollment length to control for differences in the number of medical claims due to imbalances in enrollment length between the NF1 and non-NF1 groups.
Variables
Health-care claims related to neurological and other conditions were identified by the following ICD-9-CM codes using the clinical classification software coding schema (http://www.hcup-us.ahrq.gov/toolssoftware/ccs/AppendixASingleDX.txt) or the 2009 ICD-9-CM manual23: epilepsy (345.0–345.91, 780.33, and 780.39), migraine headache (346.0–346.93), headache (784.0), MS (340), PD (332.0), sleep disturbances/disorder (780.5x and 327.3x). Of note, we excluded febrile convulsions (780.31) from the epilepsy case definition. Acute urinary tract infection (UTI) (590.0–590.9, 595.0, 595.89, 595.9, 597.0, 598.0x, and 599.0) and type 1 and 2 diabetes (250.01–250.09) were included as negative controls, based on expert knowledge suggesting that these conditions are not related to NF1. For neurological conditions and diabetes, individuals were required to have any combination of at least two outpatient or inpatient claims ≥30 days apart to be classified as having the condition. For UTI, we required individuals to have only one claim to be classified as having the condition because this is an acute condition.
Variables for conditions specifically linked to NF2 were used in sensitivity analyses to evaluate the robustness of the results when individuals with any evidence of health-care claims for NF2-related conditions (who were not identified as such by 237.72 ICD-9-CM–coded claims) were excluded from analyses. The following diagnosis codes were used for these analyses: Benign neoplasm of brain and other parts of the nervous system: 225.1 (cranial nerves), 225.2 (cerebral meninges), and 225.4 (spinal meninges); Malignant neoplasm of other and unspecified parts of the nervous system: 192.1 (cerebral meninges), 192.3 (spinal meninges), and 192.0 (cranial nerves); Secondary malignant neoplasm of other specified sites: 198.4 (other parts of the nervous system, meninges ((cerebral) (spinal)); Neoplasm of uncertain behavior of endocrine glands and nervous system: 237.6 (meninges), 237.9 (other and unspecified parts of nervous system: cranial nerves); and Disorders of the acoustic nerve: 388.5. In addition, we used the following brain tumor codes to assess whether associations between NF1 and neurological conditions (epilepsy, headache, and migraine) remained when individuals with health-care encounters related to brain tumor diagnoses were excluded (Malignant neoplasm of brain: 191.0–191.9; Benign neoplasm of brain and other parts of nervous system: 225.0–225.9; and Neoplasms of unspecified nature: 239.6 (brain)).
Health-care utilization was estimated from the number of outpatient visits using the Current Procedural Terminology24 codes 99201–99205, 99211–99215, and 99241–99245. Approximate age in years at first administrative claim for comorbidities (neurological conditions, diabetes, and UTIs) was calculated as the difference between the visit year for the first claim for the comorbidity from 2006 to 2010 and the subject’s birth year.
Statistical analysis
Statistical Analysis Software (version 9.2; SAS Institute, Cary, NC) was used for all study analyses. Unconditional logistic regression was used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to determine associations between NF1 group membership and each medical condition, adjusting for the frequency-matching variables (enrollment time in months and age), sex, and number of health-care visits. Health-care visits were used to control for differences in health-care utilization between the two study groups because there would be increased opportunity for medical condition claims in the NF1 group versus the non-NF1 group due to their increased utilization of the health-care system. Chi-square and Fisher’s exact tests were used to evaluate the statistical significance of differences in the frequency of medical condition claims by sex between the NF1 and non-NF1 groups. The Wilcoxon two-sample test (T approximation) was used to test the null hypothesis of no significant difference between the two groups in the age at first health-care claim during the study period (2006–2010) for specific medical conditions. P values were considered significant at the P ≤ 0.05 level.
Results
The NF1 group comprised 8,579 people who met our selection criteria. The non-NF1 comparison group consisted of 85,790 individuals. Subject ages ranged from 0 to 64 years, with a mean age of 24.4 years (SD = 19.3) for both groups ( Table 1 ). The mean enrollment time, percentage of individuals receiving health care through health maintenance organization plans, and geographical distribution did not differ appreciably between the two groups. By contrast, the mean number of health-care visits during the study period for the NF1 group was more than twice as high (17.6 ± 17.1 claims) as the comparison group (8.8 ± 11.7 claims). In addition, there was a slightly higher percentage of females in the NF1 group relative to the comparison group (52.3 vs. 50.5%).
In general, subjects in the NF1 group had significantly higher odds of health insurance claims for all neurological conditions evaluated ( Table 2 ). This finding was also observed when we adjusted for health maintenance organization membership; for this reason, this variable was not included in the final model. Individuals in the NF1 group had a higher odds of health insurance claims related to epilepsy (OR: 7.3; 95% CI: 6.4–8.3), migraine (OR: 2.6; 95%; CI: 2.2–2.9), headache (including migraine) (OR: 2.9; 95% CI: 2.6–3.1), MS (OR: 1.9; 95% CI: 1.2–2.9), PD (OR: 3.1; 95% CI: 1.3–7.5), and sleep disturbances/disorder (OR: 1.4; 95% CI: 1.2–2.6). Although there was no association between NF1 and health-care claims for acute UTIs (OR: 1.0; 95% CI: 0.96–1.1), individuals in the NF1 versus the non-NF1 group exhibited a significantly lower odds of diabetes claims (OR: 0.4; 95% CI: 0.3–0.4). When individuals with claims for conditions that could indicate NF2 (but who did not have claims for this condition) were excluded, the results were not materially different (data not shown).
To address the possibility that associations between NF1 and epilepsy, migraine, or headache were mediated by brain tumors, we conducted analyses that excluded individuals with brain tumor claims. For epilepsy, the overall association was slightly weaker but still significant (OR: 6.7; 95% CI 5.8–7.8). Associations for headache (including migraine) and migraine were similar to those for the analyses that did not exclude these individuals (headache (including migraine): OR: 2.7; 95% CI: 2.4–2.9; migraine: OR: 2.6; 95% CI: 2.3–3.0).
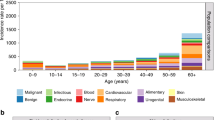
We also sought to determine whether there were any differences in the health insurance claims patterns for each medical condition as a function of age. As expected, there were no individuals in the younger age category in the NF1 group with claims for PD or MS. For other neurological conditions, the magnitude of the association was stronger for migraines, headache (includes migraine), and sleep disturbances/disorders in the younger versus the older age group, whereas the opposite was true for epilepsy.
For each medical condition category, we also assessed whether there was any evidence for differences in the sex distribution and the mean age at first health-care claim between the NF1 and the non-NF1 group ( Table 3 ). Among those identified with two or more health-care claims for epilepsy, migraine, PD, sleep disturbances, or diabetes, there was no significant difference in the percentage of females between the NF1 and non-NF1 groups. By contrast, there was a significantly lower percentage of females among those with claims for headache (including migraine) (64.6 vs. 73.2%), MS (60 and 78.7%), and UTI (77.5 and 84.5%) in the NF1 versus the non-NF1 group, respectively. Individuals in the NF1 group were on average younger at their first administrative claim for headache (including migraine) (29.9 vs. 34.2 years; P < 0.0001), migraine (31.1 vs. 36.4 years; P < 0.0001), and sleep disturbances/disorders (41.2 vs. 44.5 years; P = 0.0113) and older for UTI than those in the non-NF1 group (35.2 vs. 32.4 years; P < 0.0001).
Discussion
We observed a significantly higher odds of health-care claims related to epilepsy, migraine, headache (including migraine), sleep disorders, MS, and PD in individuals with NF1 than in those without NF1 who were identified using administrative claims data. These findings substantiate prior evidence from case reports and clinical series that have suggested causative associations between these neurological problems and NF1.
An increased prevalence of epilepsy or unprovoked seizures in individuals with NF1 has been described in previous smaller studies, in which the prevalence has been estimated between 5.9 and 9.5% (refs. 6,7,8). In the current study, we found that the prevalence of two or more epilepsy-related claims ≥30 days apart was 5.6% in the NF1 group versus 0.6% in the non-NF1 group, with evidence suggesting that both children and adults with NF1 are at risk for developing epilepsy. The propensity for individuals with NF1 to seek medical attention for seizures may be partially due to the presence of central nervous system tumors, as we have recently reported.8 However, the observation that the positive association between NF1 and epilepsy persisted after exclusion of individuals with brain tumor health-care claims suggests that other etiologies may account for epilepsy in this at-risk population.6,7,8
NF1 has been evaluated as a risk factor for headache in studies surveying NF1 patients about headaches,18,19 with mixed results. We observed a significantly higher odds of health-care claims related to headaches and migraines in individuals in the NF1 versus non-NF1 group. Consistent with studies demonstrating that headaches in NF1 do not necessarily result from intracranial tumors,18,19 the association between headaches/migraines and NF1 did not change following the exclusion of individuals with brain tumor claims. Because headaches can severely compromise quality of life, further research is warranted to examine the etiology and impact of headaches in people with NF1.
Previous case reports have also revealed a potential association between NF1 and MS.13,14,15,16,17 However, our study suggests that MS is a rare complication of NF1 (<1.0% individuals with NF1), with a twofold increased odds of MS-related health insurance claims in people with NF1. Although it is not clear why MS should be overrepresented in people with NF1, several lines of evidence suggest that this association has a biological basis. First, the OMG (oligodendrocyte-myelin glycoprotein) gene25 lies within an intron of the NF1 gene, raising the intriguing possibility that impaired OMG function could affect myelination, predisposing some individuals with NF1 to MS.15 However, OMG mutations are neither necessary nor sufficient for primary progressive MS.25 Second, the NF1 gene is highly expressed in oligodendrocytes, the primary cell type affected in MS.26 Third, Nf1 gene inactivation results in increased oligodendrocyte precursor numbers in mice27 and zebrafish,28 and leads to deregulated nitric oxide–mediated blood–brain barrier defects in Nf1 genetically engineered mouse models.29 Further investigation will be required to establish a mechanistic connection between NF1 and MS pathogenesis.
To our knowledge, there are only two published case reports of PD in individuals with NF1.20,21 PD results from insufficient striatal dopamine production resulting in a variety of movement abnormalities.30 Although we observed a threefold increased odds of PD claims in individuals in the NF1 group versus those in the non-NF1 group, there were only seven individuals in the NF1 group who had repeated claims for PD, suggesting that PD occurs very rarely in individuals with NF1. However, the potential association between NF1 and PD is intriguing in light of recent studies demonstrating that the Nf1 protein, neurofibromin, regulates striatal dopamine levels in genetically engineered mouse models.31 In this regard, Nf1 genetically engineered mouse strains exhibit attention and learning deficits that are responsive to dopamine restoration.31,32,33 Additional research will be required to establish a biological basis for this interesting association.
An increased prevalence of abnormal sleep patterns in people with NF1 has also been reported.10,11,12 In the current study, we observed a twofold higher odds of claims for sleep disturbances/disorder in individuals with NF1. Although little is known about the mechanism underlying sleep disturbances in mammals using Nf1 genetically engineered models, elegant studies in Drosophila have demonstrated that the Nf1 gene is critical for maintaining fruit fly circadian rhythm.34
Unexpectedly, we observed a significantly lower odds of diabetes-related health-care claims in individuals in the NF1 group versus those in the non-NF1 group. This inverse relationship is intriguing and has been noted in an anecdotal expert report.35 Although two prior studies have reported diabetes cases in individuals with NF1, the authors of both papers indicated that this is a rare occurrence.36,37 It is not clear why NF1 would be associated with lower risk of diabetes; however, it is possible that this reflects deregulated protein kinase B/mammalian target of rapamycin activity, resulting from defective neurofibromin protein kinase B/mammalian target of rapamycin control.38,39 Further studies will be required to establish a mechanistic connection between these two conditions.
Strengths of this study include its large size and the use of an age-matched and length of enrollment–matched comparison group that allows for estimation of relative differences in the prevalence of chronic neurological conditions in individuals with versus without NF1. In addition, we controlled for health-care utilization to minimize the concern that associations were confounded by this factor. The lack of an association between acute UTI and NF1, and the inverse association between diabetes and NF1 reinforce the concept that the positive associations detected between neurological conditions and NF1 were not due to increased surveillance for medical conditions in this population.
There are also limitations to the use of administrative claims data. Using health insurance claims, rather than physical examinations and laboratory tests, as markers of medical diagnoses (NF1 and comorbidities) may result in misclassification of individuals with respect to NF1 and comorbidities. Misclassification can result from coding errors, coding to rule out conditions, and under- and overcoding. We attempted to minimize misclassification through the application of strict selection criteria that were used in the administrative data analyses, only considering individuals to have the chronic medical conditions if they had ≥2 codes for the condition in the outpatient/inpatient setting ≥30 days apart. However, we note that this approach could miss cases of NF1. In addition, it was recently recommended as a result of a systematic review of ICD codes for the study of neurological conditions that fewer than three ICD codes can be used with sufficient accuracy for identifying cases of epilepsy and MS in administrative data; insufficient data were found for PD to make recommendations.40 Furthermore, although we excluded people with NF2 and NF2-related health-care claims from analyses, it is possible that some individuals with NF2 were not identifiable by ICD-9-CM codes. NF2 is estimated to be 10-fold less common than NF1,41 and therefore failure to exclude all subjects with NF2 is unlikely to materially impact our findings. Finally, the generalizability of this study is limited to privately insured working adults and dependent children with NF1. In addition, because MarketScan predominantly assembles claims data from larger US employers, these results may not be generalizable to individuals who are privately insured through small to medium size employers.22
In conclusion, this large administrative health insurance claims study strengthens existing evidence from uncontrolled studies that individuals with NF1 are at significantly elevated risk for a number of neurological conditions as compared with the general population. In addition, our results suggest that individuals with NF1 are at lower risk for diabetes. Additional research will be required to validate these results, mechanistically study these associations, and identify the specific factors that distinguish individuals with NF1 who are at risk for these neurological complications.
Disclosure
The authors declare no conflict of interest.
References
Crowe FW . A Clinical, Pathological, and Genetic Study of Multiple Neurofibromatosis. Thomas: Springfield, IL, 1956.
Hyman SL, Arthur Shores E, North KN . Learning disabilities in children with neurofibromatosis type 1: subtypes, cognitive profile, and attention-deficit-hyperactivity disorder. Dev Med Child Neurol 2006;48:973–977.
Walsh KS, Vélez JI, Kardel PG, et al. Symptomatology of autism spectrum disorder in a population with neurofibromatosis type 1. Dev Med Child Neurol 2013;55:131–138.
Lidzba K, Granström S, Lindenau J, Mautner VF . The adverse influence of attention-deficit disorder with or without hyperactivity on cognition in neurofibromatosis type 1. Dev Med Child Neurol 2012;54:892–897.
Pride NA, Payne JM, North KN . The impact of ADHD on the cognitive and academic functioning of children with NF1. Dev Neuropsychol 2012;37:590–600.
Vivarelli R, Grosso S, Calabrese F, et al. Epilepsy in neurofibromatosis 1. J Child Neurol 2003;18:338–342.
Hsieh HY, Fung HC, Wang CJ, Chin SC, Wu T . Epileptic seizures in neurofibromatosis type 1 are related to intracranial tumors but not to neurofibromatosis bright objects. Seizure 2011;20:606–611.
Ostendorf AP, Gutmann DH, Weisenberg JL . Epilepsy in individuals with neurofibromatosis type 1. Epilepsia 2013;54:1810–1814.
Barba C, Jacques T, Kahane P, et al. Epilepsy surgery in neurofibromatosis type 1. Epilepsy Res 2013;105:384–395.
Johnson H, Wiggs L, Stores G, Huson SM . Psychological disturbance and sleep disorders in children with neurofibromatosis type 1. Dev Med Child Neurol 2005;47:237–242.
Leschziner GD, Golding JF, Ferner RE . Sleep disturbance as part of the neurofibromatosis type 1 phenotype in adults. Am J Med Genet A 2013;161A:1319–1322.
Licis AK, Vallorani A, Gao F, et al. Prevalence of sleep disturbances in children with neurofibromatosis type 1. J Child Neurol 2013;28:1400–1405.
Pipatpajong H, Phanthumchinda K . Neurofibromatosis type I associated multiple sclerosis. J Med Assoc Thai 2011;94:505–510.
Spinicci G, Cherchi MV, Murru R, Conti M, Marrosu MG . A case of neurofibromatosis and multiple sclerosis. Neurol Sci 2010;31:631–634.
Etemadifar M, Fatehi F, Sahraian MA, et al. Multiple sclerosis and neurofibromatosis type 1: report of seven patients from Iran. Mult Scler 2009;15:1126–1130.
Perini P, Gallo P . The range of multiple sclerosis associated with neurofibromatosis type 1. J Neurol Neurosurg Psychiatry 2001;71:679–681.
Ferner RE, Hughes RA, Johnson MR . Neurofibromatosis 1 and multiple sclerosis. J Neurol Neurosurg Psychiatry 1995;58:582–585.
Clementi M, Battistella PA, Rizzi L, Boni S, Tenconi R . Headache in patients with neurofibromatosis type 1. Headache 1996;36:10.
DiMario FJ Jr, Langshur S . Headaches in patients with neurofibromatosis-1. J Child Neurol 2000;15:235–238.
D’Ambrosio G, Vizioli R . Recklinghausen disease and Parkinson disease: an unusual association. Acta Neurol (Napoli) 1984;6:274–279.
Toshima H, Nagashima T, Hirose K, Tanabe H, Tsubaki T . [A case of neurofibromatosis associated with Parkinson disease showing myokymia-like movement and hypertrophy of the lower extremities]. Rinsho Shinkeigaku 1987;27:288–291.
Hansen L, Chang S. Health Research Data for the Real World: The MarketScan®Databases. Truven Health Analytics. Ann Arbor, MI, May 2013.
Buck C . International Classification of Diseases, Ninth Revision, Clinical Modification, Standard Edition. Saunders Elsevier: St. Louis, MO, 2009.
American Medical Association. CPT 2010 Professional Edition (Spiral). Professional Edition. American Medical Association: Chicago, IL, 2010.
Johnson MR, Ferner RE, Bobrow M, Hughes RA . Detailed analysis of the oligodendrocyte myelin glycoprotein gene in four patients with neurofibromatosis 1 and primary progressive multiple sclerosis. J Neurol Neurosurg Psychiatry 2000;68:643–646.
Daston MM, Scrable H, Nordlund M, Sturbaum AK, Nissen LM, Ratner N . The protein product of the neurofibromatosis type 1 gene is expressed at highest abundance in neurons, Schwann cells, and oligodendrocytes. Neuron 1992;8:415–428.
Bennett MR, Rizvi TA, Karyala S, McKinnon RD, Ratner N . Aberrant growth and differentiation of oligodendrocyte progenitors in neurofibromatosis type 1 mutants. J Neurosci 2003;23:7207–7217.
Lee JS, Padmanabhan A, Shin J, et al. Oligodendrocyte progenitor cell numbers and migration are regulated by the zebrafish orthologs of the NF1 tumor suppressor gene. Hum Mol Genet 2010;19:4643–4653.
Mayes DA, Rizvi TA, Titus-Mitchell H, et al. Nf1 loss and Ras hyperactivation in oligodendrocytes induce NOS-driven defects in myelin and vasculature. Cell Rep 2013;4:1197–1212.
Kumar V, Abbas AK, Aster JC, Robbins SL . Robbins Basic Pathology, 9th edn. Elsevier/Saunders: Philadelphia, PA, 2013.
Brown JA, Emnett RJ, White CR, et al. Reduced striatal dopamine underlies the attention system dysfunction in neurofibromatosis-1 mutant mice. Hum Mol Genet 2010;19:4515–4528.
Brown JA, Xu J, Diggs-Andrews KA, Wozniak DF, Mach RH, Gutmann DH . PET imaging for attention deficit preclinical drug testing in neurofibromatosis-1 mice. Exp Neurol 2011;232:333–338.
Diggs-Andrews KA, Tokuda K, Izumi Y, Zorumski CF, Wozniak DF, Gutmann DH . Dopamine deficiency underlies learning deficits in neurofibromatosis-1 mice. Ann Neurol 2013;73:309–315.
Williams JA, Su HS, Bernards A, Field J, Sehgal A . A circadian output in Drosophila mediated by neurofibromatosis-1 and Ras/MAPK. Science 2001;293:2251–2256.
Riccardi VM . Neurofibromatosis: Phenotype, Natural History, and Pathogenesis, 2nd edn. Johns Hopkins University Press: Baltimore, MD, 1992.
Ozhan B, Ozguven AA, Ersoy B . Neurofibromatosis type 1 and diabetes mellitus: an unusual association. Case Rep Endocrinol 2013;2013:689107.
Zaka-ur-Rab Z, Chopra K . Diabetes melliitus in neurofibromatosis I: an unusual presentation. Indian Pediatr 2005;42:185–186.
Dasgupta B, Yi Y, Chen DY, Weber JD, Gutmann DH . Proteomic analysis reveals hyperactivation of the mammalian target of rapamycin pathway in neurofibromatosis 1-associated human and mouse brain tumors. Cancer Res 2005;65:2755–2760.
Laplante M, Sabatini DM . mTOR signaling in growth control and disease. Cell 2012;149:274–293.
St Germaine-Smith C, Metcalfe A, Pringsheim T, et al. Recommendations for optimal ICD codes to study neurologic conditions: a systematic review. Neurology 2012;79:1049–1055.
Uhlmann EJ, Plotkin SR . Neurofibromatoses. Adv Exp Med Biol 2012;724:266–277.
Acknowledgements
This work was funded in part by Washington University Institute of Clinical and Translational Sciences grant UL1 TR000448 from the National Center for Advancing Translational Sciences (National Institutes of Health) and by grant R24 HS19455 (principal investigator: V. Fraser) from the Agency for Healthcare Research and Quality. C.M. was supported by training grant 2T35HL007815 from the National Heart, Lung, and Blood Institute of the National Institutes of Health (principal investigator: C. Koong-Nah).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Madubata, C., Olsen, M., Stwalley, D. et al. Neurofibromatosis type 1 and chronic neurological conditions in the United States: an administrative claims analysis. Genet Med 17, 36–42 (2015). https://doi.org/10.1038/gim.2014.70
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/gim.2014.70
Keywords
This article is cited by
-
When Neurofibromatosis Meets Diabetes: A Long-Term Follow-up in a Pediatric Case Report
SN Comprehensive Clinical Medicine (2023)
-
Is There a Tendency for Autoimmunity in Neurofibromatosis Type 1? —Case Reports
Indian Journal of Pediatrics (2022)
-
Neurofibromatosis type 1
Nature Reviews Disease Primers (2017)
