
Abstract
Purpose:
Schwannomatosis, a subtype of neurofibromatosis, is characterized by multiple benign, nonvestibular, nonintradermal schwannomas. Although the tumor suppressor SMARCB1 gene has been frequently identified as the underlying genetic cause of half of familial and ~10% of sporadic schwannomatosis, for most other cases, further causative genes remain to be discovered. Herein, we characterize the genome of a schwannomatosis family without constitutional inactivation of the SMARCB1 gene to explore novel genomic alterations predisposing individuals to the familial disease.
Methods:
We performed whole-genome/exome sequencing on genomic DNA of both schwannomatosis-affected and normal members of the family.
Results:
We identified a novel missense mutation (p.Asp208His; c.622G>C) in the coenzyme Q10 (CoQ10) biosynthesis monooxygenase 6 gene (COQ6) in schwannomatosis-affected members. The deleterious effects of the COQ6 mutations were validated by their lack of complementation in a coq6-deficient yeast mutant. Our study further indicated that the resultant haploinsufficiency of COQ6 might lead to CoQ10 deficiency and chronic overproduction of reactive oxygen species in Schwann cells.
Conclusion:
Although the exact oncogenetic mechanisms in this schwannomatosis family remain to be elucidated, our data strongly indicate a probable role of COQ6 mutation and CoQ10 deficiency in the development of familial schwannomatosis.
Genet Med 16 10, 787–792.
Similar content being viewed by others

Main
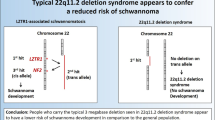
Schwannomatosis is characterized by the development of multiple schwannomas in the absence of bilateral vestibular schwannomas, and it is the third major form of neurofibromatosis (NF). It is clinically and genetically distinct from NF type 1 (NF1) and NF type 2 (NF2).1 Although biallelic NF2 mutations are found in every schwannoma in individuals with schwannomatosis, constitutional NF2 mutations are not found in schwannomatosis patients.2 Germline alterations of the SMARCB1/INI1/hSNF5 gene, encoding a core component of the SWI/SNF chromatin remodeling complex, occur in 40–60% of schwannomatosis families and in 10% of sporadic cases; however, further causative genes remain to be found.3,4 Interestingly, Piotrowski et al.5 have most recently identified LZTR1 gene mutations predisposing to multiple schwannomas in ~80% of 22q-related schwannomatosis cases lacking mutation in SMARCB1, indicating that various genetic abnormalities may potentially lead to the same disease.
In this study, we sequenced the genome of a schwannomatosis-affected Chinese family without constitutional inactivation of the SMARCB1 and LZTR1 genes to explore novel genetic alterations predisposing individuals to the familial disease.
Materials and Methods
Familial schwannomatosis
Eight members with schwannomatosis from four consecutive generations of a family included in this study were selected according to the following criteria: age: > 30 years; two or more nonintradermal schwannomas, at least one with histological confirmation; no evidence of vestibular tumor on high-quality magnetic resonance imaging scan; and no known constitutional NF2 mutation.1 The ages at initial symptoms of body pains and numbness were ~37–49 years for the disease-affected members. Among five individuals with spinal imaging, the spinal schwannoma manifested as intradural, extramedullary nodules in areas of the lumbar, thoracic, and cervical spine. The detailed clinical features of these patients are summarized in Supplementary Table S1 online.
Whole-genome/exome sequencing, sequence alignment, variant calling, and annotation
Genomic DNA (3 μg) from peripheral blood mononuclear cells was used for (i) the exon capture using the SureSelect Human All Exon Kit (Agilent Technologies, Santa Clara, CA) and (ii) sequencing and cluster generation using the Illumina Genome Analyzer IIx (Illumina, San Diego, CA), as we previously reported.6 Single-base substitutions were detected based on minimum total coverage of 10 and minimum variant coverage of 3. These variants were annotated using the SeattleSeq Web server (http://snp.gs.washington.edu/SeattleSeqAnnotation/). Small insertions/deletions and the log2 copy number variation were calculated for tumor versus normal tissue and were median centered, as we previously reported.6
Complementation in coq6-null yeast mutant
The Saccharomyces cerevisiae coq6-null mutant W303ΔG63 (Mat α ade2-1, his 3-1,15 leu2-3,112 trp1-1 ura3-1 ΔCOQ6:HIS3), yeast coq6 gene expression plasmid, and a low-copy-number (pQM) or a high-copy-number (pRCM) yeast expression plasmid containing the human COQ6 open reading frame with an in-frame amino terminal yeast mitochondrial leader sequence (as positive control for yeast rescuing studies) were generous gifts of Dr Catherine F. Clarke (University of California, Los Angeles). The D208H mutation of human COQ6 was introduced by site-directed mutagenesis (Stratagene, La Jolla, CA). The S. cerevisiae coq6-null mutants were unable to survive in media containing a nonfermentable carbon source unless a functional coq6 gene was introduced into them, and the yeast complementation experiment was performed as previously reported.7
Measurement of CoQ10 level, mitochondrial membrane potential, and ROS level
The CoQ10 level in cells was measured using a human CoQ10 ELISA kit, and this level was converted to nanograms per microgram of total cellular protein. Mitochondrial membrane potential (ΔΨm) was measured using the standard mitochondrial-specific dual-fluorescence probe JC-1 (5,5′,6,6′-tetrachloro-1,1′,3,3′-tetraethylbenzimidazolylcarbocyanine iodide), as previously reported.8 Rat COQ6 gene–specific small interfering RNA and scrambled small interfering RNA were transfected into rat Schwann cells to decrease COQ6, and then production of intracellular reactive oxygen species (ROS) in rat Schwann cells was also monitored by the fluorescence emission of 2′,7′-dichlorofluorescein at 72 hours posttransfection.8 Hemagglutinin-tagged human wild-type COQ6 and D208H COQ6 open reading frames were cloned into the pcDNA3.1 (+) mammalian expression plasmid and introduced into human fibroblast IMR90 cells to assess rescue of COQ6 knockdown by small interfering RNA.
Results
Characterization of familial schwannomatosis without constitutional inactivation of SMARCB1 gene
The disease-affected members of the family were a father and his daughter in the first and second generations, respectively, and five of eight siblings in the third generation (named as S1–S8); in addition, one member of the fourth generation has been diagnosed with schwannomatosis thus far ( Figure 1a ). The schwannomatosis tissues of S2 and S7 displayed similar morphological features under hematoxylin-and-eosin staining (upper panel in Figure 1b ) and positive staining for S-100 protein, clearly indicating their Schwann cell origin (lower panel in Figure 1b ).

Identification of D208H COQ6 mutation in familial schwannomatosis. (a) The pedigree of a familial schwannomatosis family. Filled symbols indicate schwannomatosis-affected members; the eight siblings of the third generation are marked as S1–S8. (b) Hematoxylin-and-eosin (upper panel) and S-100 protein (lower panel) staining of schwannomatosis tissues of S2 and S7. (c) Sanger sequencing maps of wild-type COQ6 of a representative normal member (top) and heterozygous D208H COQ6 (bottom) of a representative affected member. Genomic DNA samples of S4 and S5 were analyzed by whole-genome/exome sequencing; genomic DNA samples of S2, S3, and S7 were sequenced by whole-exome analysis. The COQ6 gene of S2–S5, S7, S8, and the only disease-affected member in the fourth generation was analyzed by Sanger sequencing. (d) Reverse transcription–polymerase chain reaction and Sanger sequencing demonstrated the presence of c.622G>C (D208H) COQ6 gene messenger RNA in the schwannomatosis tissues of S2 (top) and S7 (bottom). (e) Full conservation of the residue in the COQ6 protein across evolution from Escherichia coli to Homo sapiens (top). Homology model of COQ6 flavin adenine dinucleotide (FAD)-binding domain indicated that the change from D to H at residue 208 would clash with S212 and V214 of the COQ6 FAD-binding domain (bottom).
Constitutional mutations in SMARCB1, LZTR1, NF1, and NF2 genes—including point mutations, intragenic insertions/deletions, and gene duplication—were not found in the family by whole-genome sequencing analysis.3,4,5 Consistent with this observation, genetic abnormalities of SMARCB1, NF1, and NF2 in the schwannomatosis tissues of S2 and S7 were not discovered by fluorescence in situ hybridization analysis (Supplementary Figure S1a–c online) and Sanger sequencing. Immunohistochemical analysis further showed that SMARCB1 (Supplementary Figure S2a online), NF1 (Supplementary Figure S2b online), and NF2 (Supplementary Figure S2c online) proteins were normally expressed in these tissues.
Identification of constitutional COQ6 mutation in the schwannomatosis-affected family by whole-genome/exome sequencing
The distribution of schwannomatosis-affected members in the family indicated an autosomal dominant trait. To explore the genetic differences between the affected and unaffected members, we performed whole-genome sequencing on the genomic DNA samples of S4 (schwannomatosis-affected) and S5 (normal). Comparative analysis of whole-genome sequencing showed that there were no deleted/amplified DNA regions in S4 compared with the DNA of S5 (Supplementary Figure S3 online). No genetic abnormalities in the SMARCB1, LZTR1, NF1, and NF2 genes were further identified by whole-genome sequencing analysis (Supplementary Table S2 online). We further performed whole-exome sequencing on the genomic DNA samples of S2, S3, and S7 (Supplementary Figure S4 online). Twelve shared heterozygous variants, including nine missense variants (Supplementary Table S3 online), were identified by these methods (Supplementary Figure S4 online). Variants of the FLG2 gene were found to be false positives by Sanger sequencing. Variants of HRNR and GSTT2 proteins were assessed as benign by PolyPhen-2 (Polymorphism Phenotyping software, version 2).9 The de novo heterozygous variants of MYPN, COQ6, CKMT1A, CYP11A1, DUOX1, and TRIOBP genes were commonly found in all affected members.
On the basis of intensive literature review and mutation prediction of these genetic variants, we focused on a heterozygous mutation (p.Asp208His/D208H; c.622G>C), reference sequence NM_182476.2) of the COQ6 gene, whose function is essential but not redundant. Sanger sequencing analysis showed that the D208H allele was found in the disease-affected but not in normal family members ( Figure 1c ). The messenger RNA transcript of the D208H COQ6 allele was found in the schwannomatosis tissues of S2 and S7 by reverse transcription–polymerase chain reaction ( Figure 1d ). In addition to the heterozygous D208H mutation, molecular analysis did not discover other COQ6 genetic variants in these schwannomatosis tissues. COQ6 monooxygenase is evolutionarily conserved,7 and the D208 residue is located at the highly conserved flavin adenine dinucleotide (FAD)-binding domain. The missense mutation altered an amino acid residue that is uniformly conserved from Escherichia coli to Homo sapiens (humans) ( Figure 1e , upper panel). Structural modeling of the FAD-binding domain of human COQ6 using Composer in Sybyl (Tripos, St Louis, MO)10 indicated that the H208 residue would clash with the residues S212 and V214 in the FAD-binding domain ( Figure 1e , lower panel), indicating that H208 may negatively affect COQ6 function by interfering with its binding to FAD.
Validation of loss-of-function D208H COQ6 mutant and impact of knockdown of COQ6 on CoQ10 and ROS production in Schwann cells
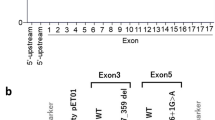
As shown in Figure 2a (left panel), all the transformed coq6-null yeast mutants grew normally in SD-Ura selective media (synthetic defined media with uracil dropout, in which glucose acts as fermentable carbon source). The yeast coq6 gene (pRS1-yQ6, positive control) and wild-type human COQ6 (hWt) gene, but not the D208H COQ6 mutant (D208H-Q6), in both high-copy-number (pRCM) and low-copy-number (pQM) plasmids (the empty vectors were negative controls) rescued the growth of coq6-null yeasts plated on YPG media (yeast extract/peptone/glycerol media, in which glycerol acts as a nonfermentable carbon source),7,11 which indicated that the D208H COQ6 mutant lacked complementation in coq6-deficient yeast mutants. Furthermore, we also verified that knockdown of COQ6 dramatically decreased CoQ10 production in human fetal lung fibroblast IMR90 cells over a period of 72 hours ( Figure 2b ). Knockdown of COQ6 in IMR90 cells dramatically decreased mitochondrial membrane potential, which may cause cell death by energy depletion, and concurrently increased ROS levels over 48 hours (Supplementary Figure S5a,b online). Furthermore, we showed that only reconstitution of wild-type human COQ6, not the D208H COQ6 mutant, rescued the IMR90 cells after knockdown of COQ6 ( Figure 2c ). Moreover, we also modeled the haploinsufficiency of COQ6 by knockdown of COQ6 gene in rat Schwann cells and found that ROS production increased in a dosage-dependent manner ( Figure 2d ), which might suggest that haploinsufficiency of COQ6 may cause chronic ROS overproduction in Schwann cells.

Loss-of-function D208H COQ6 mutation and the impact of COQ6 knockdown on reactive oxygen species (ROS) production in rat Schwann cells. (a) Wild-type human COQ6 (hWt), but not D208H mutation–containing COQ6, rescued growth of yeast coq6-null mutants plated on YPG (yeast extract/peptone/glycerol) media containing glycerol as the nonfermentable carbon source. Triplicate colonies of yeast cells harboring the indicated plasmids seeded onto both SD-Ura and YPG plate media and incubated at 30 °C for 3–6 days (pRS1-yQ6 plasmid containing the yeast coq6 gene was the positive control, and the empty high-copy-number (pRCM) and low-copy-number (pQM) plasmids were the negative controls). (b) Time-dependent decrease of CoQ10 resulting from COQ6 knockdown in IMR90 cells. Western blot of COQ6 and glyceraldehyde 3-phosphate dehydrogenase loading control (left panel) and relative quantification of CoQ10 (right panel). (c) Reconstitution of wild-type human COQ6, not D208H COQ6, rescued the decrease of mitochondrial membrane potential (MMP) and increase of ROS in COQ6-attenuated IMR90 cells. At 24 hours after the transfection with control small interfering RNA (siRNA) (Ctrl–siR) or COQ6 siRNA (Q6–siR), plasmids expressing EGFP (control), His-tag-fused wild-type human COQ6 (Wt–Q6), or D208H COQ6 (Mt–Q6) were reintroduced into IMR90 cells (blank for mock-transfected cells); 48 hours later, MMP and ROS level were determined. Upper panel: western blot of protein expression levels; lower-left panel: percentage of IMR90 cells with decreased MMP measured by JC-1 assay; lower-right panel: percentage of IMR90 cells with increased ROS monitored by the 2‘,7‘-dichlorofluorescein (DCF) assay (**P < 0.01 compared with blank). (d) Knockdown of COQ6 increased ROS production in rat Schwann cells in a dosage-dependent manner. Rat Schwann cells were transfected with 5, 10, and 20 pmol/l COQ6 siRNA; at 72 hours posttransfection, ROS and COQ6 protein levels in these cells were determined by the dichlorofluorescein assay (upper panel, percentage of cells with increased ROS) and western blot (lower panel, with β-actin loading control), respectively. JC-1, 5,5‘,6,6‘-tetrachloro-1,1‘,3,3‘-tetraethylbenzimidazolylcarbocyanine iodide.
Discussion
CoQ10 is an electron carrier in the mitochondrial respiratory chain and is also a lipid-soluble antioxidant implicated in protecting cells from damage by ROS.11 Mutations in COQ10 biosynthesis genes cause primary CoQ10 deficiency. A previous study showed that severe CoQ10 deficiency (<30%) caused a marked defect in bioenergetics, with decreased adenosine triphosphate production and sometimes decreased cell growth, but no increase in ROS or oxidative stress–induced death.12 By contrast, intermediate decreases in CoQ10 (30–50%) caused mild defects in bioenergetics, with significant increases in ROS and oxidative stress–induced cell death.12 Our knockdown of COQ6 in IMR90 cells also resulted in a similar reduction of cellular CoQ10 and mitochondrial membrane potential. We also identified that knockdown of COQ6 impaired mitochondrial function and increased ROS overproduction in rat Schwann cells, with a positive correlation between decreased COQ6 protein and ROS production.
Elevated levels of ROS and decreased levels of ROS scavengers and antioxidant enzymes are associated with various human diseases including cancers. For example, increased ROS production caused by mitochondrial DNA mutations has been linked to tumor progression in prostate cancer models.13 Abnormally low plasma levels of CoQ10 have been found in a number of cancer types, including cervical cancer and melanoma.14,15 Decreased levels of CoQ10 have been detected in human breast cancer tissues.16 However, whether deficiency of CoQ10 predisposes individuals to certain cancers is not known. Similarly, the roles of CoQ10 biosynthesis gene mutations have not been appreciated in cancers. The association is only now becoming apparent with the identification of COQ2 gene (one of the CoQ10 biosynthesis enzymes) mutations in human colon and rectal cancers, ovarian carcinoma, and glioblastoma multiforme by cancer genomic studies.17,18
In this study, we have identified a heterozygous loss-of-function COQ6 missense mutation in familial schwannomatosis. A critical issue related to implication of the genetic alteration in the familial disease is whether the heterozygous loss-of-function COQ6 displays haploinsufficiency. A large-scale screening study for genes in yeast displaying haploinsufficiency found that haploinsufficiency of coq6 resulted in a mild reduction of fitness in a medium containing glucose.19 A recent study demonstrated that both homozygous and compound heterozygous loss-of-function mutations in the human COQ6 gene caused early-onset steroid-resistant nephritic syndrome with sensorineural deafness, which progressed to end-stage renal failure by a median age of <2 years, and two single heterozygous nonsense mutations were also identified in two families with cyclosporin A–dependent nephritic syndrome and diffuse mesangial sclerosis.7 Therefore, it may be assumed that the COQ6 haploinsufficiency may be conditional and tissue/cell specific. In the family under study, none of the members harboring the mutated allele had nephritic syndrome, but they did have schwannomatosis, indicating diversity and heterogeneity of clinical phenotypes caused by defects of the same gene. Germline abnormalities associated with cancer may be detected in every cell in the body or only in the tumor cells. Interestingly, despite the presence of a constitutional genetic abnormality that might affect growth regulatory pathways in all cells, people are generally predisposed to only certain tumor types.20 In this particular family, we consider that the D208H COQ6 allele may lead to a chronic or conditional haploinsufficiency of COQ6 in a cell/tissue-specific manner, causing chronic ROS overproduction in Schwann cells through an unknown mechanism, thus predisposing the family members to familial schwannomatosis.
In summary, although the exact oncogenetic mechanism of the loss-of-function COQ6 gene in the disease remains a challenging question to be elucidated, we have, for the first time, suggested an association of the defect in one of the CoQ10 biosynthesis genes, COQ6, with familial schwannomatosis. The mutated COQ6 allele may lead to CoQ10 deficiency and chronic overproduction of ROS in Schwann cells, which may predispose individuals to the disease.
Disclosure
The authors declare no conflict of interest.
References
Baser ME, Friedman JM, Evans DG . Increasing the specificity of diagnostic criteria for schwannomatosis. Neurology 2006;66:730–732.
MacCollin M, Willett C, Heinrich B, et al. Familial schwannomatosis: exclusion of the NF2 locus as the germline event. Neurology 2003;60:1968–1974.
Hulsebos TJ, Plomp AS, Wolterman RA, Robanus-Maandag EC, Baas F, Wesseling P . Germline mutation of INI1/SMARCB1 in familial schwannomatosis. Am J Hum Genet 2007;80:805–810.
Hadfield KD, Newman WG, Bowers NL, et al. Molecular characterisation of SMARCB1 and NF2 in familial and sporadic schwannomatosis. J Med Genet 2008;45:332–339.
Piotrowski A, Xie J, Liu YF, et al. Germline loss-of-function mutations in LZTR1 predispose to an inherited disorder of multiple schwannomas. Nat Genet 2014;46:182–187.
Zhang K, Chu K, Wu X, et al. Amplification of FRS2 and activation of FGFR/FRS2 signaling pathway in high-grade liposarcoma. Cancer Res 2013;73:1298–1307.
Heeringa SF, Chernin G, Chaki M, et al. COQ6 mutations in human patients produce nephrotic syndrome with sensorineural deafness. J Clin Invest 2011;121:2013–2024.
Tong V, Teng XW, Chang TK, Abbott FS . Valproic acid II: effects on oxidative stress, mitochondrial membrane potential, and cytotoxicity in glutathione-depleted rat hepatocytes. Toxicol Sci 2005;86:436–443.
Adzhubei IA, Schmidt S, Peshkin L, et al. A method and server for predicting damaging missense mutations. Nat Methods 2010;7:248–249.
Sutcliffe MJ, Haneef I, Carney D, Blundell TL . Knowledge based modelling of homologous proteins, Part I: Three-dimensional frameworks derived from the simultaneous superposition of multiple structures. Protein Eng 1987;1:377–384.
Gin P, Hsu AY, Rothman SC, et al. The Saccharomyces cerevisiae COQ6 gene encodes a mitochondrial flavin-dependent monooxygenase required for coenzyme Q biosynthesis. J Biol Chem 2003;278:25308–25316.
Quinzii CM, López LC, Von-Moltke J, et al. Respiratory chain dysfunction and oxidative stress correlate with severity of primary CoQ10 deficiency. FASEB J 2008;22:1874–1885.
Petros JA, Baumann AK, Ruiz-Pesini E, et al. mtDNA mutations increase tumorigenicity in prostate cancer. Proc Natl Acad Sci USA 2005;102:719–724.
Palan PR, Mikhail MS, Shaban DW, Romney SL . Plasma concentrations of coenzyme Q10 and tocopherols in cervical intraepithelial neoplasia and cervical cancer. Eur J Cancer Prev 2003;12:321–326.
Rusciani L, Proietti I, Rusciani A, et al. Low plasma coenzyme Q10 levels as an independent prognostic factor for melanoma progression. J Am Acad Dermatol 2006;54:234–241.
Portakal O, Ozkaya O, Erden Inal M, Bozan B, Kosan M, Sayek I . Coenzyme Q10 concentrations and antioxidant status in tissues of breast cancer patients. Clin Biochem 2000;33:279–284.
Parsons DW, Jones S, Zhang X, et al. An integrated genomic analysis of human glioblastoma multiforme. Science 2008;321:1807–1812.
Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012;487:330–337.
Deutschbauer AM, Jaramillo DF, Proctor M, et al. Mechanisms of haploinsufficiency revealed by genome-wide profiling in yeast. Genetics 2005;169:1915–1925.
Davidoff AM . Pediatric oncology. Semin Pediatr Surg 2010;19:225–233.
Acknowledgements
This work was supported by grants from the Department of Health (DOH100-TD-C-111-008; DOH101-TD-C-111-008; DOH102-TD-C-111-008), Taipei, Taiwan. We thank all the family members for participating in this study. We thank Dr Catherine F. Clarke at the Department of Chemistry and Biochemistry and the Molecular Biology Institute, University of California, Los Angeles, for generous gifts of the yeast coq6-null mutant and the yeast and human COQ6 plasmids; Victoria Bedell of the Cytogenetic Core Laboratory, City of Hope, for assistance in fluorescence in situ hybridization assays; and Dr Peiguo Chu and Loera Sofia at the Department of Pathology for assistance in immunohistochemistry analysis. We are grateful to Dr Lynne Smith for critical review of the manuscript.
Author information
Authors and Affiliations
Corresponding authors
Supplementary information
Supplementary Figure S1
(DOC 4439 kb)
Supplementary Figure S2
(DOC 7498 kb)
Supplementary Figure S3
(DOC 162 kb)
Supplementary Figure S4
(DOC 62 kb)
Supplementary Figure S5
(DOC 846 kb)
Supplementary Table S1
(DOC 35 kb)
Supplementary Table S2
(DOC 37 kb)
Supplementary Table S3
(DOC 47 kb)
Rights and permissions
This work is licensed. under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article

Cite this article
Zhang, K., Lin, JW., Wang, J. et al. A germline missense mutation in COQ6 is associated with susceptibility to familial schwannomatosis. Genet Med 16, 787–792 (2014). https://doi.org/10.1038/gim.2014.39
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/gim.2014.39
Keywords
This article is cited by
-
An association of peripheral nerve sheath tumors and lipomas
Acta Neurochirurgica (2017)
-
The molecular pathogenesis of schwannomatosis, a paradigm for the co-involvement of multiple tumour suppressor genes in tumorigenesis
Human Genetics (2017)
-
Pathogenese und Molekularpathologie des Vestibularisschwannoms
HNO (2017)
