
Abstract
Beta-thalassemia is caused by the reduced (beta+) or absent (beta0) synthesis of the beta globin chains of the hemoglobin tetramer. Three clinical and hematological conditions of increasing severity are recognized, i.e., the beta-thalassemia carrier state, thalassemia intermedia, and thalassemia major. The beta-thalassemia carrier state, which results from heterozygosity for beta-thalassemia, is clinically asymptomatic and is defined by specific hematological features. Thalassemia major is a severe transfusion-dependent anemia. Thalassemia intermedia comprehend a clinically and genotypically very heterogeneous group of thalassemia-like disorders, ranging in severity from the asymptomatic carrier state to the severe transfusion-dependent type. The clinical severity of beta-thalassemia is related to the extent of imbalance between the alpha and nonalpha globin chains. The beta globin (HBB) gene maps in the short arm of chromosome 11, in a region containing also the delta globin gene, the embryonic epsilon gene, the fetal A-gamma and G-gamma genes, and a pseudogene (ψB1). Beta-thalassemias are heterogeneous at the molecular level. More than 200 disease-causing mutations have been so far identified. The majority of mutations are single nucleotide substitutions, deletions, or insertions of oligonucleotides leading to frameshift. Rarely, beta-thalassemia results from gross gene deletion. In addition to the variation of the phenotype resulting from allelic heterogeneity at the beta globin locus, the phenotype of beta-thalassemia could also be modified by the action of genetic factors mapping outside the globin gene cluster and not influencing the fetal hemoglobin. Among these factors, the ones best delineated so far are those affecting bilirubin, iron, and bone metabolisms. Because of the high carrier rate for HBB mutations in certain populations and the availability of genetic counseling and prenatal diagnosis, population screening is ongoing in several at-risk populations in the Mediterranean. Population screening associated with genetic counseling was extremely useful by allowing couples at risk to make informed decision on their reproductive choices. Clinical management of thalassemia major consists in regular long-life red blood cell transfusions and iron chelation therapy to remove iron introduced in excess with transfusions. At present, the only definitive cure is bone marrow transplantation. Therapies under investigation are the induction of fetal hemoglobin with pharmacologic compounds and stem cell gene therapy.
Similar content being viewed by others


Main
Beta-thalassemia is one of most common autosomal recessive disorders worldwide. High prevalence is present in populations in the Mediterranean, Middle-East, Transcaucasus, Central Asia, Indian subcontinent, and Far East. It is also relatively common in populations of African descent. The highest incidences are reported in Cyprus (14%), Sardinia (12%), and South East Asia1,2 Detailed information on the frequency of beta-thalassemia in the different regions is available from Weatherall and Clegg1 The high gene frequency of beta-thalassemia in these regions is most likely related to the selective pressure from Plasmodium falciparum malaria, as it is indicated by its distribution quite similar to that of present or past malaria endemia.3 Carriers of beta-thalassemia are indeed relatively protected against the invasion of Plasmodium falciparum. However, because of population migration and, to a limited extent, slave trade, beta-thalassemia is, at present, also common in Northern Europe, North and South America, Caribbean, and Australia.
Beta-thalassemia is caused by the reduced (beta+) or absent (beta0) synthesis of the beta globin chains of the hemoglobin (Hb) tetramer, which is made up of two alpha globin and two beta globin chains (alpha2beta2).1 Three clinical and hematological conditions of increasing severity are recognized, i.e., the beta-thalassemia carrier state, thalassemia intermedia, and thalassemia major. The beta-thalassemia carrier state, which results from heterozygosity for beta-thalassemia, is clinically asymptomatic and is defined by specific hematological features. Thalassemia major is a severe transfusion-dependent anemia. Thalassemia intermedia comprehends a clinically and genotypically very heterogeneous group of thalassemia-like disorders, ranging in severity from the asymptomatic carrier state to the severe transfusion-dependent type. The clinical severity of beta-thalassemia is related to the extent of imbalance between the alpha globin and nonalpha globin chains. The nonalpha globin chains include, in addition to the beta globin chains, also the gamma chains, which are a specific component of fetal Hb (HbF; alpha2gamma2) and are present in a small amount in normal adult individuals and in increased but variable amount in the beta-thalassemia syndromes. Within the red blood cell precursors, when the beta globin chains are reduced or absent, the unassembled alpha chains precipitate and lead to oxidative damage of the cell membrane, thereby resulting in apoptosis (ineffective erythropoiesis).4–6
CLINICAL FEATURES
Beta-thalassemia major
Homozygotes for beta-thalassemia may develop either thalassemia major or thalassemia intermedia. Individuals with thalassemia major usually come to medical attention within the first 2 years and require regular blood transfusion to survive. Those presenting later do not require transfusion and receive a diagnosis of thalassemia intermedia. Differentiation of thalassemia major from thalassemia intermedia at presentation is a difficult and critical issue that should be strongly pursued, because it may avoid unnecessary transfusions in thalassemia intermedia and start early transfusions in thalassemia major. Analysis of the genotype at the alpha and beta loci and testing for the presence of ameliorating genetic factors may be useful in this differentiation (see later).
Affected infants with thalassemia major fail to thrive and become progressively pale. Feeding problems, diarrhea, irritability, recurrent bouts of fever, and enlargement of the abdomen, caused by splenomegaly, may occur. If a regular transfusion program that maintains a minimum Hb concentration of 95–105 g/L is initiated, then growth and development are normal until the age of 10–11 years. After the age of 10–11 years, affected individuals are at risk of developing severe complications related to posttransfusional iron overload, depending on their compliance with chelation therapy.
Complications of iron overload include growth retardation and failure of sexual maturation and also those complications observed in adults with HFE-associated hereditary hemochromatosis (HH): involvement of the heart (dilated myocardiopathy and pericarditis), liver (chronic hepatitis, fibrosis, and cirrhosis), and endocrine glands (resulting in diabetes mellitus and insufficiency of the parathyroid, thyroid, pituitary, and, less commonly, adrenal glands). Infectious complications, including hepatitis B and C virus and HIV, relatively common in old patients, are now very rare because of the introduction of vaccination (hepatitis B) and development of blood donor screening methods based on viral nucleic acid enzymatic amplification. Other complications are hypersplenism (usually related to late and irregular transfusions), venous thrombosis (occurring especially after splenectomy), osteoporosis (which is multifactorial, being strongly associated with bone marrow expansion, hypogonadism, diabetes mellitus, hypothyroidism, hypoparathyroidism, low insulin-like growth factor 1, cardiac dysfunction, and may regard specific patients because of the presence of peculiar genetic predisposing factors; see later), and lung hypertension (secondary to chronic hemolysis).7–9 The risk for hepatocellular carcinoma is increased because of liver viral infection, iron overload, and longer survival.10
Survival of individuals who have been well transfused and treated with appropriate chelation extends beyond the age of 30 years. Myocardial disease caused by transfusional siderosis is the most important life-limiting complication of iron overload in beta-thalassemia. In fact, cardiac complications are reported to cause 71% of deaths in individuals with beta-thalassemia major.11
The classic clinical picture of thalassemia major is currently only seen in some developing countries, in which the resources for carrying out long-term transfusion programs are not available. The most relevant features of untreated or poorly transfused individuals are growth retardation, pallor, jaundice, brown pigmentation of the skin, poor musculature, genu valgum, hepatosplenomegaly, leg ulcers, development of masses from extramedullary hematopoiesis, and skeletal changes that result from expansion of the bone marrow. These skeletal changes include deformities of the long bones of the legs and typical craniofacial changes (bossing of the skull, prominent malar eminence, depression of the bridge of the nose, tendency to a mongoloid slant of the eye, and hypertrophy of the maxillae, which tends to expose the upper teeth).1 Individuals who have not been regularly transfused usually die before the third decade.
Beta-thalassemia intermedia
Patients with thalassemia intermedia show a markedly heterogeneous clinical picture. Principle symptoms are pallor, jaundice, cholelithiasis, liver and spleen enlargement, moderate to severe skeletal changes, leg ulcers, extramedullary masses of hyperplastic erythroid marrow, a tendency to develop osteopenia and osteoporosis, and thrombotic complications resulting from a hypercoagulable state because of the lipid membrane composition of the abnormal red blood cells (particularly in splenectomized patients).1,12 By definition, transfusions are not required or only occasionally required. Iron overload occurs mainly from increased intestinal absorption of iron caused by ineffective erythropoiesis.
Recently, the mechanism of iron hyperabsorption in beta-thalassemia has been at least partly elucidated. Iron absorption is essentially controlled by hepcidin, a small peptide secreted by the hepatocytes, which blocks iron uptake in the intestine and iron release from the reticuloendothelial system.13 Hepcidin binds ferroportin, an iron transporter present on the surface of absorptive enterocytes, macrophages, and hepatocytes, and the hepcidin-ferroportin complex is internalized and rapidly degraded, thereby explaining the defective intestinal iron absorption.14 Transcription of hepcidin is controlled by bone morphogenetic proteins (BMP), which activate the SMAD protein complex that translocates to the nucleus and stimulates hepcidin transcription.15 Hepcidin expression is enhanced by iron overload and inflammation, whereas it is inhibited by anemia and hypoxia.
Recent studies have shown that serum from untransfused thalassemia patients have high level of growth differentiation factor 15, a member of the transforming growth factor superfamily-like BMPs, whose production is related to the expansion of the erythroid compartment. Growth differentiation factor 15 inhibits hepcidin expression by opposing the effect of BMP, thereby leading to intestinal iron hyperabsorption and increased iron release from macrophages.16 Consequently, the secretion of ferritin is reduced and its serum level relatively decreased. Therefore, in thalassemia intermedia, the determination of serum ferritin underestimates the extent of iron accumulation. In contrast, in thalassemia major, red cell transfusions decrease the erythropoietic drive and increase iron overload, resulting in relatively high hepcidin level, which reduces dietary iron absorption and iron release from macrophages. This may contribute to iron accumulation in Kupffer cells17–19 (Fig. 1). The associated complications of iron overload may present later, but it may be as severe as those seen in individuals with thalassemia major who depend on transfusions.

Mechanism of control of hepcidin synthesis. Bone morphogenetic protein (BMP) through the BMP-HJV coreceptor activates SMAD protein complex, which translocates to the nucleus, acts on the promoter, and activates hepcidin production.
HEMATOLOGICAL FEATURES
Beta-thalassemia carrier state
Carriers of beta-thalassemia are clinically asymptomatic. The characteristic hematological features are microcytosis (reduced red blood cell volume), hypochromia (reduced red blood cell Hb content), increased HbA2 level (the minor component of the adult Hb, which is made up of two alpha and two delta chains [alpha2delta2]), and slightly imbalanced alpha/beta + gamma globin chain synthesis ratio (1.5–2.4), by in vitro synthesis of radioactive-labeled globin chains.
The Hb pattern of beta-thalassemia heterozygotes is characterized by 92–95% HbA, >3.8 HbA2, and variable amount of HbF (0.5–4%). Examination of the blood smear reveals microcytosis, hypochromia, and marked variations in size and shape of the red blood cells.
Thalassemia major
Patients with thalassemia major have a severe microcytic and hypochromic anemia, associated with increased number of red blood cells and low mean corpuscular volume (MCV) and mean corpuscular Hb (MCH). Peripheral blood smear shows, in addition to microcytosis and hypochromia, anisocytosis, poikilocytosis (spiculated tear drop and elongated cells), and nucleated red blood cells (i.e., erythroblasts). The number of erythroblasts is related to the degree of anemia and is markedly increased after splenectomy.
Hb pattern (by cellulose acetate electrophoresis or high-performance liquid chromatography [HPLC]) varies according to the type of beta-thalassemia. In beta0-thalassemia, characterized by the lack of beta globin chain synthesis, HbA is absent, HbF is 95–98%, and HbA2 is 2–5%. In beta+-thalassemia homozygotes with a residual variable beta globin synthesis or beta0/beta+ compound heterozygotes, the Hb pattern shows HbA between 10 and 30%, HbF in the order of 70–90%, and HbA2 of 2–5%.
Bone marrow examination is usually not necessary for diagnosis of affected individuals. Bone marrow is extremely cellular, mainly as a result of marked erythroid hyperplasia, with a myeloid/erythroid ratio reversed from the normal 3 or 4 to 0.1 or less.
In vitro synthesis of radioactive-labeled globin chains in affected individuals reveals in beta0-thalassemia a complete absence of globin beta chains and a marked excess of alpha globin chains compared with gamma globin chains; the alpha/gamma ratio is >2.0. In beta+-thalassemia, the variable degree of reduction of beta globin chains results in severe (thalassemia major) to mild (thalassemia intermedia) clinical phenotypes. The imbalance of the alpha/beta + gamma ratio is similar to that in beta0-thalassemia major.
Thalassemia intermedia
Patients with thalassemia intermedia have a moderate anemia and show a markedly heterogeneous hematological picture, ranging in severity from that of the beta-thalassemia carrier state to that of thalassemia major.
MOLECULAR GENETICS
Beta-thalassemia
The beta globin (HBB) gene maps in the short arm of chromosome 11 in a region also containing the delta globin gene, the embryonic epsilon gene, the fetal A-gamma and G-gamma genes, and a pseudogene (ψB1). The five functional globin genes are arranged in the order of their developmental expression (Fig. 2).

Chromosome localization and structure of alpha and beta globin gene clusters (for details see text).
The HBB gene, which spans 1.6 Kb, contains three exons and both 5′ and 3′ untranslated regions (UTRs). The HBB is regulated by an adjacent 5′ promoter in which a TATA, CAAT, and duplicated CACCC boxes are located. A major regulatory region, containing also a strong enhancer, maps 50 Kb from the beta globin gene (Fig. 2). This region, dubbed locus control region (LCR), contains four (HS-1 to HS-4) erythroid specific DNAse hypersensitive sites (HSs), which are a hallmark of DNA-protein interaction. Each HS site is constituted by a combination of several DNA motifs interacting with transcription factors, among which the most important are GATA-1 (GATA indicates the relative recognition motif), nuclear factor erythroid 2, erythroid Kruppel-like factor, and friend of GATA 1.The importance of LCR for the control of the beta-like globin gene expression has been discovered by studying a series of naturally occurring deletions that totally or partly remove the HS sites and result in the inactivation of the intact downstream beta globin gene. Several transcription factors bind and regulate the function of the HBB gene, the most important of which is erythroid Kruppel-like factor 1, which binds the proximal CACCC box, and whose knockout in the mouse leads to a beta-thalassemia-like clinical picture.
Beta-thalassemias are heterogeneous at the molecular level. More than 200 disease-causing mutations have been so far identified. The majority of mutations are single nucleotide substitutions or deletions or insertions of oligonucleotides leading to frameshift. Rarely beta-thalassemias result from gross gene deletion. A complete updated list of beta-thalassemia mutations is available through the Globin Gene Server Web Site (http://www.globin.cse.psu.edu).
Point mutations affecting the beta globin expression belong to three different categories: mutations leading to defective beta-gene transcription (promoter and 5′ UTR mutations); mutations affecting messenger RNA (mRNA) processing (splice-junction and consensus sequence mutations, polyadenylation, and other 3′ UTR mutations); and mutations resulting in abnormal mRNA translation (nonsense, frameshift, and initiation codon mutations).
Beta0-thalassemias, characterized by the complete absence of beta chain production result from deletion, initiation codon, nonsense, frameshift, and splicing mutations, especially at the splice-site junction. On the other hand, beta+-thalassemias, characterized by reduced production of the beta chains, are produced by mutations in the promoter area (either the CACCC or TATA box), the polyadenylation signal, and the 5′ or 3′ UTR or by splicing abnormalities. According to the extent of the reduction of the beta chain output, the beta+-thalassemia mutations may be divided into severe, mild, and silent. A list of the mild and silent mutations is reported in Table 1.
The silent mutations, which are characterized by normal hematological findings and defined only by a mildly imbalanced alpha/beta globin chain synthesis ratio, result from mutations of the distal CACCC box, the 5′ UTR, the polyadenylation signal and some splicing defects. The mild mutations show moderate thalassemia-like hematological features and imbalanced globin chain synthesis and are produced by mutations in the proximal CACCC box, TATA box, 5′ UTR, or exon 1, causing alternative splicing (Hb Malay, HbE, and codon 24 T→A), or in the consensus splicing sequence, 3′ UTR, and poly-A site. Mutations activating a cryptic splicing site in exon 1, at codons 19, 26, and 27, are associated with a mild or silent phenotype, because of the preferential use of the normal splice site, and result in the production of the abnormal Hb Malay, HbE (extremely common in South East Asia), and Hb Knossos, respectively.
A few beta0-thalassemias display a mild phenotype (for instance, cd6-A and cd 8-AA) because of the linkage with the nondeletion promoter mutation of the G-gamma gene (−158 G-gamma), which is associated with high production of HbF during hematologic stress.
Deletions affecting the beta globin gene are very rare, except for a 619-bp deletion removing the 3′ end of the beta globin gene, which is relatively common in Sind and Punjab populations of India and Pakistan. Another group of deletions (complex beta-thalassemia), in addition to the beta globin gene, involve also the delta (delta-beta0-thalassemia), the delta and A-gamma genes (G-gammaA-gammadeltabeta0-thalassemia), or the whole beta globin gene cluster. Finally, partial or total deletions of the LCR, but leaving the beta globin gene intact, inactivate the beta globin gene.
Despite the marked molecular heterogeneity, the prevalent molecular defects are limited in each at risk population (Fig. 3), in which 4–10 mutations usually account for most of the beta globin disease-causing allele.

Most common beta-thalassemia mutations in different countries.
Beta-thalassemic hemoglobinopathies
Under this category are included different structurally abnormal Hbs associated with a beta-thalassemia phenotype. Three different molecular mechanisms are responsible for these phenotypes: activation of cryptic splice site in exons, leading, for instance, to the production of HbE (already mentioned); formation of a delta-beta hybrid gene; or mutation causing hyperunstable beta globin.
The delta-beta hybrid genes leading to beta-thalassemia are dubbed Hb Lepore genes and are made up of N-terminal amino acid sequence of the normal delta chain and the C terminal sequence of the normal beta chain. Depending on the codon of transition from delta to beta sequences, different Hb Lepore genes have been described. In peripheral blood, Hbs Lepore are present in low percentage of total Hb (around 10% in carriers) because of the low production, which depends on the reduced activity of the delta promoter and on the relative instability of the variant Hb. These characteristics explain why Hbs Lepore are considered a beta-thalassemia-like mutation.
Hyperunstable beta globins comprehend a group of beta globin mutants, which result in the production of Hb variants that are extremely unstable and precipitate before assembling with the alpha chains to produce the Hb tetramer. This results in ineffective erythropoiesis, which is exacerbated by the concomitant relative excess of the alpha chains, thereby leading to phenotypic thalassemia-like manifestations (more frequently in thalassemia intermedia than in the heterozygous state).
Beta-thalassemia-like mutations mapping outside the beta globin gene cluster
In rare instances, the beta-thalassemia defect does not lie in the beta globin gene cluster. Some mutations in the X-linked transcription factor GATA-1 may produce thrombocytopenia associated with thalassemia trait, whereas molecular lesions affecting the general transcription factor TFIIH result, in addition to thalassemia-like hematological features, in xeroderma pigmentosum and trichothiodystrophy.20,21
Molecular diagnosis of beta-thalassemia
Commonly occurring mutations of the HBB gene are detected by a number of polymerase chain reaction (PCR)-based procedures. The most commonly used methods are reverse dot blot analysis or primer-specific amplification with a set of probes or primers complementary to the most common mutations in the population from which the affected individual originated.22 Other methods based on real-time PCR or microarray technology because of their reproducibility, rapidity, and easy handling are potentially suitable for the routine clinical laboratory.23,24
If targeted mutation analysis fails to detect the mutation, scanning or sequence analysis can be used. Sensitivity of both mutation scanning and sequence analysis is 99%. In the meantime, the presence of an extended deletion should be investigated by using multiplex ligation-dependent probe amplification (MPLA).
PHENOTYPE-GENOTYPE CORRELATION
Homozygous beta-thalassemia
Homozygosity or compound heterozygosity for beta-thalassemia most commonly result in the clinical phenotype of transfusion-dependent thalassemia major. However, a consistent proportion of homozygotes develop milder forms, called thalassemia intermedia, which range in severity from thalassemia major to the beta-thalassemia carrier state.25–29
To understand the clinical-molecular relationships, we should remember that the main pathophysiological determinant of the severity of the beta-thalassemia syndromes is the extent of alpha/nonalpha globin chain imbalance (see Introduction). Therefore, any factor capable of reducing the alpha/nonalpha chain imbalance may have an ameliorating effect on the clinical picture.
The most clinically important mechanism consistently resulting in thalassemia intermedia is the coinheritance of homozygosity or compound heterozygosity for mild beta-thalassemia alleles, namely a beta-thalassemia defect associated with a consistent residual output of beta chains from the affected beta globin locus (see Molecular genetics). The most common mild mutations are beta+IVS-I nt 6 (T→C)—found in the Mediterranean area, and beta codon 26 (G→A), which gives rise to HbE, prevailing in South-East Asia (Table 1). By contrast, compound heterozygotes for a mild and a severe defect result in a spectrum of phenotypes ranging from severe to mild forms. Therefore, from the clinical point of view, in presence of a mild beta-thalassemia/severe beta-thalassemia genotype, we cannot predict the development of mild clinical picture.
The mildest beta-thalassemia alleles are the silent alleles (Table 1), which show normal hematological features and can be identified solely by a slight imbalance of alpha/nonalpha globin chain synthesis ratio.30–32 Homozygosity for silent alleles produces a very mild form of thalassemia intermedia. Mild beta-thalassemia also results from the beta-silent/beta-mild or beta-silent/beta-severe genotypes.
It should be pointed out that, as we will see later on, even the homozygous beta0 or severe beta+-thalassemia may develop an attenuated form resulting from coinherited modifying ameliorating genetic factors.
The second mechanism leading to mild beta-thalassemia is the coinheritance of homozygous beta-thalassemia and an alpha-thalassemia determinant that, by reducing the alpha chain output, decreases the alpha/nonalpha chain imbalance. A single alpha globin gene deletion is sufficient to improve the clinical phenotype of homozygous beta+-thalassemia, whereas in beta0-thalassemia, the deletion of two alpha globin genes or the presence of an inactivating mutation of the major alpha2 globin gene is necessary.26,33,34
The third mechanism is the coinheritance of a genetic determinant that is able to sustain a continuous production of gamma chains in adult life, thereby reducing the extent of the alpha/nonalpha chain imbalance. The nature of the beta-thalassemia mutation per se may affect the ability to produce gamma chains. This mechanism occurs in delta beta0-thalassemia, which is because of deletions of variable extent within the beta globin cluster, and in those more limited deletions involving only the 5′ region of the beta globin promoter. In other cases, the reason for the high gamma chain output depends on the co-transmission of a nondeletion form of hereditary persistence of HbF (HPFH), caused by point mutations at G-gamma or A-gamma promoters (−196 C→T A-gamma; −158 C→T G-gamma). A C→T mutation at position −196 A-gamma has been found to be associated in cis with the codon 39 nonsense mutation in some Sardinian beta-thalassemia chromosomes (Sardinian deltabeta0-thalassemia).35 The increase in gamma chain production from the −196 A-gamma gene probably compensates for the absence of beta chain production from the affected beta locus. Compound heterozygosity for this determinant and for typical beta–thalassemia, thus, develops thalassemia intermedia. Homozygotes for the Sardinian deltabeta0-thalassemia are clinically normal and can be detected solely by hematological analysis.36 Heterozygotes for Sardinian deltabeta-thalassemia have thalassemia-like hematological features and high HbF levels.37 In contrast, C→T −158 G-gamma is silent both in normal subjects and beta-thalassemia heterozygotes but leads to a high HbF production rate during hematopoietic stress, as occurs in homozygous beta-thalassemia or sickle cell anemia.38 The −158 G-gamma mutation may be associated with IVS II nt 1 (G→A), frameshift 8 (AA), frameshift 6 (-A), and someone with codon 39 nonsense mutations, thereby explaining the mild phenotype possibly associated with these mutations.
Coinheritance of genetic determinants capable of sustaining a continuous production of HbF in adult life and mapping outside the beta globin cluster may also determine a mild phenotype. It should be noted that the residual amount of HbF in normal adults is unevenly distributed and mainly contained in a subpopulation of red blood cells, denominated “F cells.” Both HbF and F-cells percentage, in normal adults and in beta-thalassemia heterozygotes, show a wide variation quantitative trait loci (QTLs)with a continuous distribution.38 Those individuals with a moderate increase of HbF in the order of 0.8–5%, with an heterocellular distribution, are indicated as carriers of heterocellular HPFH. So far, two HPFH have been mapped on chromosome 2p16 and chromosome 6q23.39–41The locus on chromosome 2p16 has been located by genome-wide association study on the BCL11A gene, and the single nucleotide polymorphism (SNP) rs11886868 in its intron 2 was found strongly associated with HbF levels. Furthermore, the C allele of this SNP was significantly higher in Sardinian individuals with elevated HbF levels (HPFH). The BCL11A variants were shown to influence HbF levels also in nonanemic Caucasians from a European twin study.40 The same C variant was significantly higher in beta0-thalassemia homozygotes for the codon 39 nonsense mutation with a mild phenotype (thalassemia intermedia), as compared with those with the same beta globin genotype, but with a severe phenotype, compensating for the imbalance of Hb production through the augmentation of HbF levels.39 Furthermore, the BCL11A variant C allele by increasing HbF levels was associated with a mild phenotype also in sickle cell disease.39,42 In conclusion, the BCL11A gene is able to modify the phenotype of homozygous beta-thalassemia and sickle cell anemia by increasing HbF levels. The BCL11A gene encodes a zinc-finger transcription factor, which regulates the globin switching during ontogeny by interacting with specific sequence in the beta globin cluster and repressing the HbF expression43,44
According to these results, the identification of BCL11A polymorphism in young homozygous beta-thalassemia and sickle cell anemia patients may serve as a prognostic indication for the severity of the disease. Furthermore, targeted down-regulation of BCL11A in patients could elevate HbF levels, thereby ameliorating the severity of these inherited anemias.
Another HPFH locus has been mapped many years ago on chromosome 6q23 by linkage analysis in a large Indian family with segregating beta-thalassemia45 and confirmed more recently by twin studies.38 Further studies have shown that the chromosome 6 genetic variant responsible for HbF variation maps in the HBS1L-MYB region. Specifically, the G allele of SNP rs9389268 is associated with high HbF levels. The causal variant in this region and its mechanism for increasing HbF is not yet known. HBS1L is a putative member of the “GTPase superfamily,” whereas MYB has a crucial role in normal erythropoiesis. Recent studies have shown that the HBS1L-MYB intergenic polymorphisms contain regulatory sequences controlling MYB expression.46 However, further studies are necessary to elucidate the biological role of these two genes in the modulation of HbF. The HBS1L-MYB locus contributes 3–7% of trait variance,39,42 whereas the BCL11A variant explain 7–12%.42,47
Two QTL loci mapping on chromosome 848,49 and chromosome X,50,51 respectively, have not been validated in subsequent genome-wide linkage and association studies.39,40
The loci-modulating HbF levels explain only partially its variation. This consideration clearly indicates the existence of other QTL traits for HbF in the human genome. Recent studies from our group indicate that the BCL11A, HBS1L-MYB region, and alpha-thalassemia contribute differently in the amelioration of clinical severity in thalassemia intermedia (odd ratio 5.15, 4.61, and 3.3, respectively). Taken together, the loci are able to correctly predict 75% of the phenotypes of homozygous beta0-thalassemia.52
In conclusion, despite the significant progress made in this field of thalassemia disorders, in a significant number of cases of thalassemia intermedia, the molecular mechanism has not been so far elucidated.
Heterozygous beta-thalassemia
From the clinical point of view, heterozygous beta-thalassemia, whether beta0 or beta+, is completely asymptomatic and is characterized hematologically by high red blood cell count, microcytosis, hypochromia, increased HbA2 levels, and unbalanced alpha/nonalpha globin chain synthesis. However, several environmental or genetic factors may modify this phenotype, leading either to thalassemia intermedia, despite the presence of a single beta globin gene affected, or to hematologically atypical carrier states (see Beta-thalassemia carrier identification).
To date, two mechanisms have been identified, which may increase the clinical and hematological severity of beta-thalassemia heterozygotes. The first is related to the coinheritance of both heterozygous beta-thalassemia and triple or quadruple alpha globin gene arrangement, which, by increasing the magnitude of imbalance of alpha/non alpha globin chain synthesis, may cause an excess of unassembled alpha chains, thereby resulting in premature destruction of red blood cell precursors. Beta-thalassemia carriers who are heterozygous or homozygous for the triplicated alpha globin gene arrangement may indeed develop a clinical phenotype of intermediate severity.53–56 Similarly, phenotype of thalassemia intermedia has also been seen in beta-thalassemia carriers who have inherited a chromosome containing the quadruplicated alpha globin gene arrangement.57–59 However, normal people carrying the triplicated or quadruplicated alpha globin gene arrangement have a normal phenotype most likely, because the small excess of alpha chains that is synthesized can be eliminated by proteolysis.
The other mechanism increasing the severity in beta-thalassemia heterozygotes depends on the presence of a mutation in the beta globin gene, which causes an extreme instability of the beta globin chains.60,61 Heterozygotes for this condition are more severely affected than subjects with the beta-thalassemia carrier state, because in addition to producing an excess of alpha chains, they synthesize highly unstable beta chains that bind heme and precipitate in red blood cell precursors before assembling with the alpha chains. This leads to the production of inclusion bodies made up of alpha and unstable beta chains. Beta-thalassemia resulting from hyperunstable beta chains is transmitted in a dominant fashion or may result from a de novo mutation.
Mutations leading to hyperunstable beta chains include missense mutations, minor deletions leading to loss of intact codon, and frameshifts. Most mutations in the phase termination codons that result in dominant beta-thalassemia lie in exon 3, whereas those producing the typical recessively inherited forms are located in exons 1 or 2. In exons 1 or 2 mutations, very little beta globin mRNA is found in the cytoplasm of red blood cell precursors, whereas exon 3 mutations are associated with a substantial amount of abnormal cytoplasmic mRNA. This leads to the synthesis of truncated beta chains products, which are unstable and thereby act in a dominant-negative fashion, causing premature destruction of red blood cells. This difference depends on the fact that premature termination codon mutations lying in exons 1 or 2 activate the process of nonsense-mediated mRNA decay, therefore precluding the accumulation of mRNA encoding for truncated peptides.62 The diagnosis of dominant beta-thalassemia is difficult, because the unstable beta globin chains in peripheral blood are not easily detected, not even by very accurate electrophoretic or chromatographic procedures. The suspicion for such conditions should derive from the presence of beta-thalassemia-like disorders of intermediate severity arising de novo or transmitted according to a dominant pattern.
Exceptionally, beta-thalassemia intermedia may develop in subjects heterozygous for beta-thalassemia because of a mosaic somatic deletion of the in trans beta globin gene in a subpopulation of hematopoietic cells.63,64
Compound heterozygosity for beta-thalassemia and some beta chain structural variant (HbD-Los Angeles beta 121 Glu→Gln; HbC beta 6 Glu→Lys; HbO-Arab beta 121 Glu→Lys) may produce thalassemia intermedia as a result of globin chain imbalance in combination with the modified structural and functional characteristic of the variants.65
Finally, the proposed role, if any, of the alpha-Hb stabilizing protein (AHSP) as a modulating factor of the phenotype has not yet clarified.66 AHSP forms a stable complex with free alpha-Hb and protect free alpha chain from precipitation, thereby acting as a specific alpha-Hb molecular chaperone. In the mouse system, knockout of AHSP leads to reduced lifespan of circulating red blood cells, causing increased apoptosis of erythroid precursors and exacerbating the severity of heterozygous beta-thalassemia, which usually displays a thalassemia intermedia phenotype.66 The studies of AHSP in humans led to inconstant results. It seems, however, that variation of the AHSP level may be able to aggravate the phenotype of simple heterozygotes for beta-thalassemia.67,68 The most common ascertained mechanism leading to thalassemia intermedia are summarized in Table 2.
Other clinical genetic modifiers
In addition to the variation of the phenotype resulting from allelic heterogeneity at the beta globin locus, from the effect of alpha or gamma globin gene mutation or from coinheritance of heterocellular HPFH delineated above, the phenotype of beta-thalassemia could also be modified by the action of genetic factors mapping outside the globin gene cluster and not influencing the HbF. Among these factors, the ones best delineated so far are those affecting bilirubin, iron, and bone metabolisms.69
Because of the rapid turnover of red cell precursors and the resulting breakdown of the heme products, both homozygotes and heterozygotes for beta-thalassemia may develop mild jaundice and have the propensity to gallstone formation. In beta-thalassemia, the level of indirect bilirubin and gallstone formation are related to a polymorphic motif in the promoter of the gene involved in the hepatic glucuronidation of bilirubin, namely bilirubin UDP-glucuronosyltransferase (UGT1A). In normal individuals, the promoter has six TA repeats in the TATA box (TA)6. Homozygotes for an additional repeat (TA)7 develop mild unconjugated hyperbilirubinemia (Gilbert syndrome) because of less efficient activity of UGT1. Studies performed in the last few years in thalassemia major, thalassemia intermedia, and beta-thalassemia carrier state have shown that patients developing hyperbilirubinemia, jaundice, and gallstones usually have the more common and less efficient TA7 motif.70–75 It should be pointed out that the same phenomenon has been observed in many varieties of hemolytic anemia.76–79 These findings have led us to conclude that the Gilbert syndrome mutation acts as a modifying gene in beta-thalassemia by determining or promoting the development of jaundice or gallstones.
Patients with beta-thalassemia, especially when not well chelated, develop extensive iron accumulation in many tissues including liver, heart, and endocrine glands, in part, because of the destruction of transfused red blood cells and, in part, particularly in thalassemia intermedia, because of increased iron absorption. Some studies seem to indicate that the common mutation of the HFE gene (C282Y), which causes the common type of HH, might be involved in determining the variability of iron overload in patients with thalassemia intermedia.80 Longo et al.81 by studying a large group of thalassemia major patients found that the presence of a single mutation in HFE gene (C282Y and H63D) does not influence the severity of iron loading, assessed by serum ferritin and liver iron concentration, likely because the effect of the mutations on iron overload is hidden as a result of treatment (i.e., posttransfusional iron overload and iron chelation). Furthermore, homozygosity for the H63D mutation, whose functional significance in HH is still being evaluated, when coinherited with heterozygous beta-thalassemia seems to determine an increase in iron overload.82 Conversely, coinherited heterozygosity for beta-thalassemia seems to increase the rate of iron accumulation in C282Y homozygotes.83
Another common complication, in adults with beta-thalassemia, is the development of marked and progressive osteoporosis, which depends on many factors including hypogonadism and extent of iron chelation. However, recent evidence seems to indicate that the development of this complication may be also related to polymorphisms of the genetic loci involved in bone metabolism, namely vitamin D receptor and the COLIAI gene.84–88
Finally, it should be pointed out that there is marked evidence indicating that the high frequency of beta-thalassemia in certain areas of the world is related to heterozygote advantage vis-a-vis Plasmodium falciparum malaria.89 Exposure to malaria, however, resulted also in the expansion of polymorphisms at many other genetic loci, including human leukocyte antigen (HLA), tumor necrosis factor alpha, and intercellular adhesion molecule-1, which have an important role in the defense mechanisms against infectious diseases.90–92 This consideration may indicate that children with beta-thalassemia may respond to infections differently than normal children.
BETA-THALASSEMIA CARRIER IDENTIFICATION
The typical phenotype of the beta-thalassemia trait, essentially characterized by reduced MCV, MCH, and increased HbA2, may be modified by several coinherited genetic factor, which may cause problems in carrier identification (Table 3).
Coinheritance of heterozygous beta-thalassemia and alpha-thalassemia may raise the MCV and the MCH, high enough to determine normal values at least in some of these double heterozygotes. This may occur as a result of either a deletion of two alpha globin structural genes or as a nondeletion lesion affecting the major alpha globin gene (the two functional alpha genes, denominated as alphal and alpha2, have a relative expression of 1:3). Fortunately, these carriers may be easily identified for their high HbA2 levels.93,94
Elevation of HbA2 is the most important feature in the detection of heterozygous beta-thalassemia, but a substantial group of beta-thalassemia heterozygotes may have normal HbA2. The first mechanism to account for the abnormally low HbA2 levels in a beta-thalassemia carrier is the presence of a specific mild beta-thalassemia mutation, such as the beta+ IVS-I nt 6 mutation.95 A second common mechanism is the coinheritance of heterozygous beta-thalassemia and delta-thalassemia. The decreased output of the delta globin chains may result in normalization of HbA2 levels.96,97 Also, gammadeltabeta- and deltabeta-thalassemia carriers have normal HbA2. However, all these normal-HbA2 atypical heterozygotes have low MCV and MCH. Because of this phenotype, normal HbA2 beta-thalassemia heterozygotes should be differentiated from alpha-thalassemia heterozygotes by globin chain synthesis analysis and/or by alpha, beta, and delta globin gene analysis. Deltabeta-thalassemia, in addition, may easily be defined by the variable but markedly increased HbF.
Another major problem in carrier screening is the identification of silent beta-thalassemia or the triple or quadruple alpha globin gene arrangement, both of which may lead to the production of intermediate forms of beta-thalassemia by interacting with typical heterozygous beta-thalassemia. Silent beta-thalassemias are characterized by normal MCV and MCH values and normal HbA2 and by the fact that they are defined only by the slight imbalance in the alpha/nonalpha globin synthesis.
Nevertheless, on examining the hematological features of these carriers, one may find borderline HbA2 or MCV and MCH values, which may alert for the presence of atypical beta-thalassemia, thus requiring further studies (globin chain synthesis or gene analysis). The most common silent beta-thalassemia is the beta+ −101 C→T mutation; others are very rare.98 The triple-quadruple alpha globin gene arrangement may show a slight imbalance of alpha/nonalpha chain synthesis or, more commonly, may be completely silent. An extreme, although rare, instance of thalassemia gene combination, which may result in carrier identification, is the coinheritance of alpha, delta, and beta-thalassemia, which may lead to a completely silent phenotype.99
Carrier detection procedure
Several procedures have been proposed for beta-thalassemia carrier screening.100 The cheapest and simplest is based on MCV and MCH determination, followed by HbA2 quantitation for subjects showing microcytosis (low MCV) and reduced Hb content per red blood cell (low MCH). However, because with this procedure a considerable proportion of double heterozygotes for beta- and alpha-thalassemia may be missed (these are found in many populations, such as Sardinians, where both disorders are common), it can only be used in populations with a low frequency of alpha-thalassemia. At our center in Cagliari, in the first set of examinations, we include MCV and MCH determination and Hb chromatography by HPLC, which can quantitate HbA2 and HbF and can detect the most common Hb variants (HbS, HbC, and HbE) that may result in a Hb disorder by interacting with beta-thalassemia (Fig. 4). It should be stated that HPLC is also capable of detecting Hb Knossos, a mild beta-thalassemia allele, which is not identified by using common procedures for Hb analysis. In the presence of low MCV and MCH and elevated HbA2 levels, a diagnosis of heterozygous beta-thalassemia is made. A phenotype characterized by microcytosis, hypochromia, normal-borderline HbA2, and normal HbF may result from iron deficiency, alpha-thalassemia, gammadeltabeta-thalassemia, beta + delta-thalassemia, or mild beta-thalassemia. After excluding iron deficiency through appropriate studies (red blood cell, zinc protoporphyrin determination, and transferrin saturation), the different thalassemia determinants leading to this phenotype are discriminated by globin chain synthesis analysis and eventually by alpha, beta, and delta globin gene analysis.100 In the presence of normal MCV and borderline HbA2 levels, we are inclined to suspect the presence of a silent mutation or the triple or quadruple alpha globin gene arrangement and, therefore, proceed directly to alpha- and beta globin gene analysis, because the alpha/beta globin chain synthesis ratio could also be normal.101 Definition of the type of thalassemias in these carriers is solely recommended when they mate with a carrier of a typically high HbA2 beta-thalassemia or an undetermined type of thalassemia. In those rare cases showing normal or low MCV-MCH, normal or reduced HbA2 levels, and high HbF, we suspect the presence of deltabeta-thalassemia, which should be differentiated from HPFH. This distinction is performed by globin chain synthesis analysis (normal in HPFH and unbalanced in deltabeta-thalassemia) or beta-cluster gene analysis or both.

Flowchart for thalassemia carrier identification.
Molecular diagnosis of modifying genes
Molecular diagnosis is carried out in patients affected by homozygous beta-thalassemia for defining the genotype, which may be useful for predicting the severity of the disease, and in carriers identified by hematological analysis.
The procedures available to detect the beta-thalassemia mutation have been already described.23,24As previously mentioned, delta globin gene analysis may be necessary to define double heterozygotes for delta- and beta-thalassemia that may be mistaken for alpha-thalassemia trait. The suspicion of interacting delta-thalassemia may arise when borderline HbA2 levels are found or when family studies show segregating delta-thalassemia (characterized by normal MCV-MCH and low HbA2) and beta-thalassemia. However, identification of delta and beta double heterozygotes may be accomplished by globin chain synthesis analysis and/or alpha, beta, and delta globin gene analysis.101,102
Definition of the delta-thalassemia mutation may be carried out using one of the previously mentioned PCR-based methods. As in beta-thalassemia, also in delta-thalassemia, each population at risk has its own spectrum of common delta-thalassemia mutations that may be defined through a limited number of specific primers/probes. In Sardinians, for instance, few delta-thalassemia mutations have been so far detected. The list of delta-thalassemia mutations is available at the repository of the human beta and delta globin gene mutation. Although most of the delta-thalassemia determinants are in trans (on opposite chromosomes) to beta-thalassemia, some have also been detected in cis (on the same chromosome).103
Definition of the alpha globin gene arrangement may be performed to discriminate between heterozygosity for alpha-thalassemia and double heterozygosity for delta- and beta-thalassemia or gammadeltabeta-thalassemia. This analysis could also be useful in defining coinherited alpha-thalassemia in homozygous beta-thalassemia, which may lead to the prediction of a mild clinical condition. Deletion alpha0- or alpha+-thalassemias are detected by PCR using two primers flanking the deletion breakpoint, which amplify a DNA segment only in presence of specific deletions.104 Nondeletion alpha-thalassemia may be detected by restriction endonuclease analysis or allelic oligonucleotide specific probes on selectively amplified alpha1 and alpha2 globin genes. Alpha globin gene triplication and quadruplication may be detected by the MPLA procedure.
Definition of coinherited HPFH determinants can be useful in predicting the severity of the phenotype of an affected fetus. As mentioned above, in fact, on increasing the gamma chain output, coinherited HPFH with homozygous beta-thalassemia may lead to a milder phenotype. The presence of high HbF in the parents may lead to the suspicion of double heterozygosity for beta-thalassemia and HPFH. The 196 C→T in the A-gamma gene and −158 C→T in the G-gamma gene mutations have been proved to be capable of ameliorating the clinical phenotype of homozygous beta-thalassemia. The HPFH determinants may easily be detected through restriction endonuclease or dot blot analysis with oligonucleotide-specific probes on PCR-amplified DNA. Furthermore, definition of the polymorphisms at the BCL11A and HBS1L-MYB region may lead to predict the development of a specific mild phenotype.
If targeted mutation analysis fails to detect the mutation, mutation scanning or sequence analysis can be used to detect mutations in the HBB coding region (mutations in the noncoding region would not be detected by this analysis). Sensitivity of both mutation scanning and sequence analysis is 99%.
Deletions of variable extent of the beta gene or of the HBB cluster that result in beta-thalassemia or in the complex beta-thalassemias, called gammadeltabeta-thalassemia and deltabeta-thalassemia, are rare causes of beta-thalassemia and testing that deletions is available clinically by using MPLA.
POPULATION SCREENING
Because of the high carrier rate for HBB mutations in certain populations and the availability of genetic counseling and prenatal diagnosis, population screening is ongoing in several at-risk populations in the Mediterranean.105 Carrier testing relies on hematological analysis. When the hematological analysis indicates a beta-thalassemia carrier state, molecular genetic testing of HBB can be performed to identify a disease-causing mutation. If both partners of a couple have the HBB disease-causing mutation, each of their offspring has a ¼ risk of being affected. Through genetic counseling and the option of prenatal testing, such a couple can opt to bring to term only those pregnancies in which the fetus is unaffected.
The optimal time for the assessment of genetic risk, definition of carrier status, and genetic counseling is before pregnancy. It is appropriate to offer genetic counseling (including discussion on the availability of prenatal diagnosis, potential risks to offspring, and reproductive options) to young adults who are carriers.
Population screening associated with genetic counseling is extremely useful by allowing couples at risk to make informed decision on their reproductive choices. Furthermore, in the population at risk targeted by screening, a consistent reduction of the birth rate of affected children was registered, as shown in the Sardinian population.
Prenatal diagnosis
In high-risk pregnancies in which both members are defined carriers for beta-thalassemia, prenatal diagnosis is possible by analysis of DNA extracted from fetal cells obtained by amniocentesis, usually performed at approximately 15–18 weeks' gestation, or chorionic villus sampling at approximately 10–12 weeks' gestation. Both disease-causing alleles must be identified before prenatal testing can be performed.
Alternatively, following an accurate genetic counseling explaining the pros and cons of the procedure preimplantation genetic diagnosis may be considered.
Prenatal diagnosis by analysis of fetal cells in maternal blood is not yet available but is being investigated on a research basis.106,107 Finally, analysis of fetal DNA in maternal plasma for the presence of the father's mutation may lead to prenatal exclusion of homozygous beta-thalassemia. This testing is not yet clinically available but under investigation on a research basis with promising results.108,109
In indeterminate-risk pregnancies, either one parent is a definite heterozygote and the other parent has a beta-thalassemia-like hematologic picture, but no HBB mutation has been identified by sequence analysis, or a mother is a known heterozygote and the father is unknown or unavailable for testing, especially if the father belongs to a population at risk. In either instance, the options for prenatal testing should be discussed in the context of formal genetic counseling. In indeterminate-risk pregnancies, the prenatal testing strategy is the analysis for the known HBB mutation. If the known HBB mutation is present, analysis of globin chain synthesis is performed on a fetal blood sample obtained by percutaneous umbilical blood sampling at approximately 18–21 weeks' gestation.
CLINICAL MANAGEMENT
A comprehensive review of the management of thalassemia major and thalassemia intermedia has been published by Thalassemia International Federation and is available at the Thalassemia International Federation Web site.110
Transfusion program
In thalassemia major, regular transfusions correct the anemia, suppress erythropoiesis, and inhibit increased gastrointestinal absorption of iron. Before starting the transfusions, it is absolutely necessary to carry out hepatitis B vaccination and perform extensive red blood cell antigen typing, including Rh, Kell, Kidd, and Duffy and serum immunoglobulin determination, the latter of which detects individuals with IgA deficiency who need special (repeatedly washed) blood unit preparation before each transfusion. The transfusion regimen is designed to obtain a pretransfusion Hb concentration of 95–100 g/L. Transfusions are usually given every 2–3 weeks.
Treatment of individuals with thalassemia intermedia is symptomatic and based on splenectomy and folic acid supplementation. Treatment of extramedullary erythropoietic masses is based on radiotherapy, transfusions, or, in selected cases, hydroxyurea (with a protocol similar to that used for sickle cell disease). Hydroxyurea also increases globin gamma chains and may have other undefined mechanisms. Because individuals with thalassemia intermedia may develop iron overload from increased gastrointestinal absorption of iron or from occasional transfusions, chelation therapy is started when the serum ferritin concentration exceeds 300 μg/L.17,111
Transfusional iron overload
The most common secondary complications are those related to transfusional iron overload, which can be prevented by adequate iron chelation. After 10–12 transfusions, chelation therapy is initiated with desferrioxamine B (DFO), administered 5–7 days a week by 12-hour continuous subcutaneous infusion via a portable pump. Recommended dosage depends on the individual's age and the serum ferritin concentration. Young children start with 20–30 mg/kg/day, increasing up to 40 mg/kg/day after the age of 5–6 years. The maximum dose is 50 mg/kg/day after growth is completed. The dose may be reduced if serum ferritin concentration is low. By maintaining the total body iron stores below critical values (i.e., hepatic iron concentration <7.0 mg per gram of dry weight liver tissue), DFO therapy prevents the secondary effects of iron overload, resulting in a consistent decrease in morbidity and mortality.11 Ascorbate repletion (daily dose not to exceed 100–150 mg) increases the amount of iron removed after DFO administration. Side effects of DFO are more common in the presence of relatively low iron burden and include ocular and auditory toxicity, growth retardation, and, rarely, renal impairment and interstitial pneumonitis. DFO administration also increases susceptibility to Yersinia infections. The major drawback of DFO chelation therapy is low compliance resulting from complications of administration.
In clinical practice, the effectiveness of DFO chelation therapy is monitored by routine determination of serum ferritin concentration. However, serum ferritin concentration is not always reliable for evaluating iron burden, because it is influenced by other factors, the most important being the extent of liver damage.
Determination of liver iron concentration in a liver biopsy specimen shows a high correlation with total body iron accumulation and is the gold standard for evaluation of iron overload. However, (1) liver biopsy is an invasive technique involving the possibility (though low) of complications; (2) liver iron content can be affected by hepatic fibrosis, which commonly occurs in individuals with iron overload and hepatitis C virus infection; and (3) irregular iron distribution in the liver can lead to possible false-negative results.112
In recent years, magnetic resonance imaging (MRI) techniques for assessing iron loading in the liver and heart have improved.113–115 T2 and T2* parameters have been validated for liver iron concentration. Cardiac T2* is reproducible, is applicable between different scanners, correlates with cardiac function, and relates to tissue iron concentration.113,114 Clinical utility of T2* in monitoring individuals with siderotic cardiomyopathy has been demonstrated.116 Calibration of T2* in the heart will be available in the near future.
Magnetic biosusceptometry (SQUID), which gives a reliable measurement of hepatic iron concentration, is another option117; however, magnetic susceptometry is currently available only in a limited number of centers worldwide.
Two other chelators have been introduced into clinical use: deferiprone and deferasirox
Deferiprone (L-1), a bidentated oral chelator, available for several years in many countries, is administered in a dose of 75–100 mg/kg/day. The main side effects of deferiprone therapy include neutropenia, agranulocytosis, arthropathy, and gastrointestinal symptoms that demand close monitoring.118 Recent findings seem to exclude any correlation between deferiprone treatment and progression of liver fibrosis.119 The effect of deferiprone on liver iron concentration may vary among the individuals treated. However, results from independent studies suggest that deferiprone may be more cardioprotective than DFO. Compared with those being treated with DFO, individuals on treatment with deferiprone have better myocardial MRI pattern and less probability of developing (or worsening preexisting) cardiac disease.120–123 These retrospective observations have been confirmed in a prospective study.124 After many years of controversy, deferiprone is emerging as a useful iron chelator equivalent/alternative to DFO.125,126
Deferasirox became recently available for clinical use in patients with thalassemia. It is effective in adults and children and has a defined safety profile that is clinically manageable with appropriate monitoring. The most common treatment-related adverse events are gastrointestinal disorders, skin rash, and a mild, nonprogressive increase in serum creatinine concentration.127,129 Postmarketing experience and several phase IV studies will further evaluate the safety and efficacy of deferasirox.
New strategies of chelation using a combination of DFO and deferiprone have been effective in individuals with severe iron overload; toxicity was manageable.130–135 In the past few years, particular attention has been directed to the early diagnosis and treatment of cardiac disease because of its critical role in determining the prognosis of individuals with beta-thalassemia. Assessment of myocardial siderosis and monitoring of cardiac function combined with intensification of iron chelation result in excellent long-term prognoses.116,136
Follow-up
For individuals with thalassemia major, follow-up to monitor the effectiveness of transfusion therapy and chelation therapy and their side effects includes the following:
-
Physical examination every month by a physician familiar with the affected individual and the disease;
-
Assessment of liver function tests (serum concentration of alanine transaminase) every 2 months;
-
Determination of serum ferritin concentration every 3 months;
-
Assessment of growth and development every 6 months (for pediatric patients);
-
Annual assessment includes the following:
-
Ophthalmologic and audiologic examinations;
-
Complete cardiac evaluation and evaluation of thyroid, endocrine pancreas, parathyroid, adrenal, and pituitary function (usually after 10 years);
-
Liver ultrasound evaluation, determination of serum alpha-fetoprotein concentration in adults with hepatitis C and iron overload for early detection of hepatocarcinoma; and
-
Bone densitometry to assess for osteoporosis in the adult.
-
-
Assessment for liver and heart iron with MRI should be in general recommended after 10 years of age and repeated according to the severity of iron overload, transfusion, and chelation regimes137; and
-
Regular gallbladder echography for early detection of cholelithiasis,70 particularly in individuals with the Gilbert syndrome genotype (i.e., presence of the [TA]7/[TA]7 motif in the promoter of the UGT1A gene).
Bone marrow transplantation
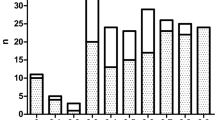
Bone marrow transplantation (BMT) from an HLA-identical sib represents an alternative to traditional transfusion and chelation therapy. If BMT is successful, iron overload may be reduced by repeated phlebotomy, thus eliminating the need for iron chelation. The outcome of BMT is related to the pretransplantation clinical conditions, specifically the presence of hepatomegaly, extent of liver fibrosis, and magnitude of iron accumulation. In children who lack the above risk factors, disease-free survival is over 90%138 (Fig. 5). A lower survival rate of approximately 60% is reported in individuals with all three risk factors. Chronic graft-versus-host disease of variable severity may occur in 5–8% of individuals. BMT from unrelated donors has been performed on a limited number of individuals with beta-thalassemia. Provided that selection of the donor is based on stringent criteria of HLA compatibility and that individuals have limited iron overload, results are comparable with those obtained when the donor is a compatible sib.139 However, because of the limited number of individuals enrolled, further studies are needed to confirm these preliminary findings. Cord blood transplantation from a related donor offers a good probability of a successful cure and is associated with a low risk of graft-versus-host disease.140,141 For couples who have already had a child with thalassemia and who undertake prenatal diagnosis in a subsequent pregnancy, prenatal identification of HLA compatibility between the affected child and an unaffected fetus allows collection of placental blood at delivery and the option of cord blood transplantation to cure the affected child.142 On the other hand, in case of an affected fetus and a previous normal child, the couple may decide to continue the pregnancy and pursue BMT later, using the normal child as the donor.

Disease-free survival in 61 thalassemic patients (age, 1–15 years) transplanted from a familial donor at BMT Unit Ospedale Regionale Microcitemico di Cagliari, Italy.
Therapies under investigation
New chelation strategies, including the combination or alternate treatment with the available chelators, are under investigation. Induction of HbF synthesis can reduce the severity of beta-thalassemia by improving the imbalance between alpha and nonalpha globin chains. Several pharmacologic compounds including 5-azacytidine, decytabine, and butyrate derivatives have had disappointing results in clinical trials.143 These agents induce HbF by different mechanisms that are not yet well defined. Their potential in the management of beta-thalassemia syndromes is still under investigation.
The studies on BCL11 pave the way to develop a therapy based on down-regulation of this gene, which may lead to an increase of HbF level, thereby ameliorating the clinical severity of the disease.39 Interesting possibility of a new therapy are open by the finding of association of low cMYB level (one of the gene mapping on 6q23) and high HbF level.144
The efficacy of hydroxyurea treatment in individuals with thalassemia is still unclear. Hydroxyurea is used in persons with thalassemia intermedia to reduce extramedullary masses, to increase Hb levels, and, in some cases, to improve leg ulcers. A good response, correlated with particular polymorphisms in the beta globin cluster (i.e., C→T at −158 G-gamma) has been reported in individuals with transfusion dependence.145,146 However, controlled and randomized studies are warranted to establish the role of hydroxyurea in the management of thalassemia syndromes.
The possibility of correction of the molecular defect in hematopoietic stem cells by transfer of a normal gene via a suitable vector or by homologous recombination is being actively investigated.147 The most promising results in the mouse model have been obtained with lentiviral vectors.148,149 Specifically, the vector developed by Sadelain et al. containing HS2, 3, and 4 from LCR associated with an extended beta globin gene led to partial correction of anemia in a beta-thalassemia mouse.147 Regarding the alternative approach, in a mouse model of sickle cell anemia, Chang et al.150 were able to correct the molecular defect by homologous recombination by transfecting the embryonic stem cells from the affected mice with a DNA fragment containing the normal beta globin gene sequences. Hematopoietic stem cells, derived from the corrected embryonic stem cells ex vivo, were able to produce HbA and HbS, thereby leading to a phenotype similar to human sickle cell trait. This and other similar experiments indicate the possibility of curing inherited hemoglobinopathies by homologous recombination in embryonic stem cells.
A new opportunity in the field of stem cell research has been recently determined by the discovery that transfection of four transcription factors (Oct 3–4, Sox 2, cMyc, and Klf4) in several types of adult cells (e.g., fibroblasts) may produce a cell with very similar characteristics to embryonic stem cells (induced pluripotent stem cell [iPS]).151,152 Further research in this field demonstrated that cMyc may not be necessary, thereby reducing the risk of oncogenic transformation. iPS from patients affected by a number of monogenic diseases, such as spinal muscular atrophy or amyotrophic lateral sclerosis, have been already produced. Based on this technology, Hanna et al.153 have recently obtained iPS from fibroblasts of a mouse affected by sickle cell anemia. The iPSs were corrected ex vivo by homologous recombination. Hematopoietic stem cells derived from ex vivo-corrected iPS were able to cure the affected mouse. This experiment offers proof of principle that genetically corrected iPS cells may lead to a cure for the inherited hemoglobinopathies.
REFERENCES
Wheatherall DJ, Clegg JB . The thalassemia syndromes. 4th ed. Oxford, England: Blackwell Science Ltd, 2001.
Weatherall DJ, Clegg JB, Higgs DR, Wood WG . The hemoglobinopathies. In: Scriver CR, Beaudet Al, Sly WS, Valle D, Vogelstein B, editors. The metabolic and molecular bases of inherited disease (OMMBID). Chapter 101. New York, NY: McGraw-Hill, 2002. Available at: www.ommbid.com. Accessed December 31, 2007.
Flint J, Harding RM, Boyce AJ, Clegg JB . The population genetics of the haemoglobinopathies. Baillieres Clin Haematol 1993; 6: 215–262.
Rund D, Rachmilewitz E . Beta-thalassemia. N Engl J Med 2005; 353: 1135–1146.
Cao A, Galanello R . Beta-thalassemia. Available at: http://www.geneclinics.org. Accessed December 1, 2005.
Olivieri N, Weatherall DJ . Clinical aspects of β-thalassemia. In: Steinberg MH, Forget BG, Higgs DR, Nagel RL, editors. Disorders of hemoglobin, genetics, pathophysiology, and clinical management. Cambridge, England: Cambridge University, 2001; 277–341.
Voskaridou E, Anagnostopoulos A, Konstantopoulos K, et al. Zoledronic acid for the treatment of osteoporosis in patients with beta-thalassemia: results from a single-center, randomized, placebo-controlled trial. Haematologica 2006; 91: 1193–1202.
Voskaridou E, Terpos E . New insights into the pathophysiology and management of osteoporosis in patients with beta thalassaemia. Br J Haematol 2004; 127: 127–139.
Origa R, Fiumana E, Gamberini MR, et al. Osteoporosis in beta-thalassemia: clinical and genetic aspects. Ann N Y Acad Sci 2005; 1054: 451–456.
Borgna-Pignatti C, Vergine G, Lombardo T, et al. Hepatocellular carcinoma in the thalassaemia syndromes. Br J Haematol 2004; 124: 114–117.
Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica 2004; 89: 1187–1193.
Eldor A, Rachmilewitz EA . The hypercoagulable state in thalassemia. Blood 2002; 99: 36–43.
Ganz T . Hepcidin, a key regulator of iron metabolism and mediator of anemia of inflammation. Blood 2003; 102: 783–788.
Nemeth E, Tuttle MS, Powelson J, et al. Hepcidin regulates cellular iron efflux by binding to ferroportin and inducing its internalization. Science 2004; 306: 2090–2093.
Wang RH, Li C, Xu X, et al. A role of SMAD4 in iron metabolism through the positive regulation of hepcidin expression. Cell Metab 2005; 2: 399–409.
Tanno T, Bhanu NV, Oneal PA, et al. High levels of GDF15 in thalassemia suppress expression of the iron regulatory protein hepcidin. Nat Med 2007; 13: 1096–1101.
Origa R, Galanello R, Ganz T, et al. Liver iron concentrations and urinary hepcidin in beta-thalassemia. Haematologica 2007; 92: 583–588.
Gardenghi S, Marongiu MF, Ramos P, et al. Ineffective erythropoiesis in beta-thalassemia is characterized by increased iron absorption mediated by down-regulation of hepcidin and up-regulation of ferroportin. Blood 2007; 109: 5027–5035.
Weizer-Stern O, Adamsky K, Amariglio N, et al. Downregulation of hepcidin and haemojuvelin expression in the hepatocyte cell-line HepG2 induced by thalassaemic sera. Br J Haematol 2006; 135: 129–138.
Viprakasit V, Gibbons RJ, Broughton BC, et al. Mutations in the general transcription factor TFIIH result in beta-thalassaemia in individuals with trichothiodystrophy. Hum Mol Genet 2001; 10: 2797–2802.
Freson K, Matthijs G, Thys C, et al. Different substitutions at residue D218 of the X-linked transcription factor GATA1 lead to altered clinical severity of macrothrombocytopenia and anemia and are associated with variable skewed X inactivation. Hum Mol Genet 2002; 11: 147–152.
Old J, Traeger-Synodinos J, Galanello R, Petrou M, Angastiniotis M . Prevention of Thalassemias and other hemoglobin disorders. Vol 2: Laboratory Methods. Nicosia, Cyprus: Thalassemia International Federation (TIF), 2005.
Vrettou C, Traeger-Synodinos J, Tzetis M, Malamis G, Kanavakis E . Rapid screening of multiple beta-globin gene mutations by real-time PCR on the LightCycler: application to carrier screening and prenatal diagnosis of thalassemia syndromes. Clin Chem 2003; 49: 769–776.
Ye BC, Zhang Z, Lei Z . Molecular analysis of alpha/beta-thalassemia in a southern Chinese population. Genet Test 2007; 11: 75–83.
Ho PJ, Hall GW, Luo LY, Weatherall DJ, Thein SL . Beta-thalassaemia intermedia: is it possible consistently to predict phenotype from genotype?. Br J Haematol 1998; 100: 70–78.
Galanello R, Dessi E, Melis MA, et al. Molecular analysis of beta zero-thalassemia intermedia in Sardinia. Blood 1989; 74: 823–827.
Cao A, Gasperini D, Podda A, Galanello R . Molecular pathology of thalassemia intermedia. Eur J Int Med 1990; 1: 227–236.
Rund D, Oron-Karni V, Filon D, Goldfarb A, Rachmilewitz E, Oppenheim A . Genetic analysis of beta-thalassemia intermedia in Israel: diversity of mechanisms and unpredictability of phenotype. Am J Hematol 1997; 54: 16–22.
Wainscoat JS, Thein SL, Weatherall DJ . Thalassaemia intermedia. Blood Rev 1987; 1: 273–279.
Gonzalez-Redondo JM, Stoming TA, Kutlar A, et al. A C-T substitution at nt-101 in a conserved DNA sequence of the promotor region of the beta-globin gene is associated with “silent” beta-thalassemia. Blood 1989; 73: 1705–1711.
Bianco I, Cappabianca MP, Foglietta E, et al. Silent thalassemias: genotypes and phenotypes. Haematologica 1997; 82: 269–280.
Murru S, Pischedda MC, Cao A, et al. A promoter mutation of the beta-globin gene (−101 C–>T) has an age-related expression pattern. Blood 1993; 81: 2818–2819.
Wainscoat JS, Kanavakis E, Wood WG, et al. Thalassaemia intermedia in Cyprus: the interaction of alpha and beta thalassaemia. Br J Haematol 1983; 53: 411–416.
Cao A, Galanello R, Rosatelli MC . Genotype-phenotype correlations in beta-thalassemias. Blood Rev 1994; 8: 1–12.
Pirastu M, Kan YW, Galanello R, Cao A . Multiple mutations produce delta beta° thalassemia in Sardinia. Science 1984; 223: 929–930.
Galanello R, Barella S, Satta S, Maccioni L, Pintor C, Cao A . Homozygosity for nondeletion delta-beta(0) thalassemia resulting in a silent clinical phenotype. Blood 2002; 100: 1913–1914.
Cao A, Melis MA, Galanello R, et al. Delta beta (F)-thalassaemia in Sardinia. J Med Genet 1982; 19: 184–192.
Thein SL, Menzel S . Discovering the genetics underlying foetal haemoglobin production in adults. Br J Haematol 2009; 145: 455–467.
Uda M, Galanello R, Sanna S, et al. Genome-wide association study shows BCL11A associated with persistent fetal hemoglobin and amelioration of the phenotype of beta-thalassemia. Proc Natl Acad Sci U S A 2008; 105: 1620–1625.
Menzel S, Garner C, Gut I, et al. A QTL influencing F cell production maps to a gene encoding a zinc-finger protein on chromosome 2p15. Nat Genet 2007; 39: 1197–1199.
Thein SL, Menzel S, Peng X, et al. Intergenic variants of HBS1L-MYB are responsible for a major quantitative trait locus on chromosome 6q23 influencing fetal hemoglobin levels in adults. Proc Natl Acad Sci U S A 2007; 104: 11346–11351.
Lettre G, Sankaran VG, Bezerra MA, et al. DNA polymorphisms at the BCL11A, HBS1L-MYB, and beta-globin loci associate with fetal hemoglobin levels and pain crises in sickle cell disease. Proc Natl Acad Sci U S A 2008; 105: 11869–11874.
Sankaran VG, Menne TF, Xu J, et al. Human fetal hemoglobin expression is regulated by the developmental stage-specific repressor BCL11A. Science 2008; 322: 1839–1842.
Chen Z, Luo HY, Steinberg MH, Chui DH . BCL11A represses HBG transcription in K562 cells. Blood Cells Mol Dis 2009; 42: 144–149.
Thein SL, Weatherall DJ . A non-deletion hereditary persistence of fetal hemoglobin (HPFH) determinant not linked to the beta-globin gene complex. Prog Clin Biol Res 1989; 316B: 97–111.
Wahlberg K, Jiang J, Rooks H, et al. The HBS1L-MYB intergenic interval associated with elevated HbF levels shows characteristics of a distal regulatory region in erythroid cells. Blood 2009; 114: 1254–1262.
Sedgewick AE, Timofeev N, Sebastiani P, et al. BCL11A is a major HbF quantitative trait locus in three different populations with beta-hemoglobinopathies. Blood Cells Mol Dis 2008; 41: 255–258.
Garner CP, Tatu T, Best S, Creary L, Thein SL . Evidence of genetic interaction between the beta-globin complex and chromosome 8q in the expression of fetal hemoglobin. Am J Hum Genet 2002; 70: 793–799.
Garner C, Silver N, Best S, et al. Quantitative trait locus on chromosome 8q influences the switch from fetal to adult hemoglobin. Blood 2004; 104: 2184–2186.
Miyoshi K, Kaneto Y, Kawai H, et al. X-linked dominant control of F-cells in normal adult life: characterization of the Swiss type as hereditary persistence of fetal hemoglobin regulated dominantly by gene(s) on X chromosome. Blood 1988; 72: 1854–1860.
Dover GJ, Smith KD, Chang YC, et al. Fetal hemoglobin levels in sickle cell disease and normal individuals are partially controlled by an X-linked gene located at Xp22.2. Blood 1992; 80: 816–824.
Galanello R, Sanna S, Perseu L, et al. Amelioration of Sardinian beta-zero thalassemia by genetic modifiers. Blood 2009; 114: 3935–3937.
Galanello R, Ruggeri R, Paglietti E, Addis M, Melis MA, Cao A . A family with segregating triplicated alpha globin loci and beta thalassemia. Blood 1983; 62: 1035–1040.
Thein SL, Al-Hakim I, Hoffbrand AV . Thalassaemia intermedia: a new molecular basis. Br J Haematol 1984; 56: 333–337.
Kulozik AE, Thein SL, Wainscoat JS, et al. Thalassaemia intermedia: interaction of the triple alpha-globin gene arrangement and heterozygous beta-thalassaemia. Br J Haematol 1987; 66: 109–112.
Kanavakis E, Metaxotou-Mavromati A, Kattamis C, Wainscoat JS, Wood WG . The triplicated alpha gene locus and beta thalassaemia. Br J Haematol 1983; 54: 201–207.
Thompson CC, Ali MA, Vacovsky M, Boyadjian S . The interaction of anti 3.7 type quadruplicated alpha-globin genes and heterozygous beta-thalassemia. Hemoglobin 1989; 13: 125–135.
Sollaino MC, Paglietti ME, Perseu L, Giagu N, Loi D, Galanello R . Association of alpha globin gene quadruplication and heterozygous beta thalassemia in patients with Thalassemia intermedia. Haematologica 2009; 94: 1445–1448.
Harteveld CL, Refaldi C, Cassinerio E, Cappellini MD, Giordano PC . Segmental duplications involving the alpha-globin gene cluster are causing beta-thalassemia intermedia phenotypes in beta-thalassemia heterozygous patients. Blood Cells Mol Dis 2008; 40: 312–316.
Thein SL . Dominant beta thalassaemia: molecular basis and pathophysiology. Br J Haematol 1992; 80: 273–277.
Murru S, Poddie D, Sciarratta GV, et al. A novel beta-globin structural mutant, Hb Brescia (beta 114 Leu-Pro), causing a severe beta-thalassemia intermedia phenotype. Hum Mutat 1992; 1: 124–128.
Thein SL . Is it dominantly inherited beta thalassaemia or just a beta-chain variant that is highly unstable?. Br J Haematol 1999; 107: 12–21.
Badens C, Mattei MG, Imbert AM, et al. A novel mechanism for thalassaemia intermedia. Lancet 2002; 359: 132–133.
Galanello R, Perseu L, Perra C, et al. Somatic deletion of the normal beta-globin gene leading to thalassaemia intermedia in heterozygous beta-thalassaemic patients. Br J Haematol 2004; 127: 604–606.
Huisman TH . Silent beta-thalassemia and thalassemia intermedia. Haematologica 1990; 75 ( suppl 5): 1–8.
Kong Y, Zhou S, Kihm AJ, et al. Loss of alpha-hemoglobin-stabilizing protein impairs erythropoiesis and exacerbates beta-thalassemia. J Clin Invest 2004; 114: 1457–1466.
Lai MI, Jiang J, Silver N, et al. Alpha-haemoglobin stabilising protein is a quantitative trait gene that modifies the phenotype of beta-thalassaemia. Br J Haematol 2006; 133: 675–682.
Galanello R, Perseu L, Giagu N, Sole G, Perra C . AHSP expression in beta thalassemia carriers with thalassemia intermedia phenotype. Blood 2003; 102: Abstract 1881
Weatherall DJ . Phenotype-genotype relationships in monogenic disease: lessons from the thalassaemias. Nat Rev Genet 2001; 2: 245–255.
Galanello R, Piras S, Barella S, et al. Cholelithiasis and Gilbert's syndrome in homozygous beta-thalassaemia. Br J Haematol 2001; 115: 926–928.
Dewey KW, Grossman H, Canale VC . Cholelithiasis in thalassemia major. Radiology 1970; 96: 385–388.
Borgna-Pignatti C, De Stefano P, Pajno D, Tomasi G, Gatti C . Cholelithiasis in children with thalassemia major: an ultrasonographic study. J Pediatr 1981; 99: 243–244.
Scutellari PN, Bighi S, Orzincolo C, Cervi PM, Nibbio A . Incidence of biliary calculosis in beta-thalassemic syndromes. Minerva Pediatr 1981; 33: 983–990.
Borgna-Pignatti C, Rigon F, Merlo L, et al. Thalassemia minor, the Gilbert mutation, and the risk of gallstones. Haematologica 2003; 88: 1106–1109.
Galanello R, Perseu L, Melis MA, et al. Hyperbilirubinaemia in heterozygous beta-thalassaemia is related to co-inherited Gilbert's syndrome. Br J Haematol 1997; 99: 433–436.
Iolascon A, Faienza MF, Moretti A, Perrotta S, Miraglia del Giudice E . UGT1 promoter polymorphism accounts for increased neonatal appearance of hereditary spherocytosis. Blood 1998; 91: 1093.
Miraglia del Giudice E, Perrotta S, Nobili B, Specchia C, D'Urso G, Iolascon A . Coinheritance of Gilbert's syndrome increases the risk for developing gallstones in patients with hereditary spherocytosis. Blood 1999; 94: 2259–2262.
Cappellini MD, Martinez di Montemuros F, Sampietro M, Tavazzi D, Fiorelli G . The interaction between Gilbert's syndrome and G6PD deficiency influences bilirubin levels. Br J Haematol 1999; 104: 928–929.
Galanello R, Cipollina MD, Carboni G, et al. Hyperbilirubinemia, glucose-6-phosphate-dehydrogenase deficiency and Gilbert's syndrome. Eur J Pediatr 1999; 158: 914–916.
Rees DC, Singh BM, Luo LY, Wickramasinghe S, Thein SL . Nontransfusional iron overload in thalassemia. Association with hereditary hemochromatosis. Ann N Y Acad Sci 1998; 850: 490–494.
Longo F, Zecchina G, Sbaiz L, Fischer R, Piga A, Camaschella C . The influence of hemochromatosis mutations on iron overload of thalassemia major. Haematologica 1999; 84: 799–803.
Melis MA, Cau M, Deidda F, Barella S, Cao A, Galanello R . Mutation in HFE gene increases iron overload in beta-thalassemia carriers. Haematologica 2002; 87: 242–245.
Piperno A, Mariani R, Arosio C, et al. Haemochromatosis in patients with beta-thalassaemia trait. Br J Haematol 2000; 111: 908–914.
Rees DC, Singh BM, Luo LY, Wickramasinghe S, Thein Sl . Genetic influenes on bone disease in thalassemia. Blood 1998; 92: S532a.
Wonke B . Bone disease in beta-thalassaemia major. Br J Haematol 1998; 103: 897–901.
Perrotta S, Cappellini MD, Bertoldo F, et al. Osteoporosis in beta-thalassaemia major patients: analysis of the genetic background. Br J Haematol 2000; 111: 461–466.
Dresner Pollak R, Rachmilewitz E, Blumenfeld A, Idelson M, Goldfarb AW . Bone mineral metabolism in adults with beta thalassemia major and intermedia. Br J Haematol 2000; 111: 902–907.
Wonke B, Jensen C, Hanslip JJ, et al. Genetic and acquired predisposing factors and treatment of osteoporosis in thalassaemia major. J Pediatr Endocrinol Metab 1998; 11( suppl 3): 795–801.
Weatherall DJ, Clegg JB, Kwiatkowski D . The role of genomics in studying genetic susceptibility to infectious disease. Genome Res 1997; 7: 967–973.
Hill AVS, Allsopp CEM, Kwiatkowski D . Common west African HLA antigens are associated with protection from severe malaria. Nature 1991; 352: 595–600.
McGuire W, Hill AVS, Allsopp CEM, Greenwood BM, Kwiatkowski D . Variation in the TNF-alfa promoter region associated with susceptibility to cerebral malaria. Nature 1994; 371: 508–511.
Fernandez-Reyes D, Craig AG, Kyes SA, et al. A high frequency African coding polymorphism in the N-terminal domain of ICAM-1 predisposing to cerebral malaria in Kenya. Hum Mol Genet 1997; 6: 1357–1360.
Melis MA, Pirastu M, Galanello R, Furbetta M, Tuveri T, Cao A . Phenotypic effect of heterozygous alpha and beta 0-thalassemia interaction. Blood 1983; 62: 226–229.
Rosatelli C, Falchi AM, Scalas MT, Tuveri T, Furbetta M, Cao A . Hematological phenotype of the double heterozygous state for alpha and beta thalassemia. Hemoglobin 1984; 8: 25–35.
Tamagnini GP, Lopes MC, Castanheira ME, Wainscoat JS, Wood WG . Beta + thalassemia—Portuguese type: clinical, haematological and molecular studies of a newly defined form of beta thalassaemia. Br J Haematol 1983; 54: 189–200.
Moi P, Paglietti E, Sanna A, et al. Delineation of the molecular basis of delta- and normal HbA2 beta-thalassemia. Blood 1988; 72: 530–533.
Tzetis M, Traeger-Synodinos J, Kanavakis E, Metaxotou-Mavromati A, Kattamis C . The molecular basis of normal HbA2 (type 2) beta-thalassemia in Greece. Hematol Pathol 1994; 8: 25–34.
Ristaldi MS, Murru S, Loudianos G, et al. The C-T substitution in the distal CACCC box of the beta-globin gene promoter is a common cause of silent beta thalassaemia in the Italian population. Br J Haematol 1990; 74: 480–486.
Galanello R, Paglietti ME, Addis M, et al. Pitfalls in genetic counselling for beta-thalassemia: an individual with 4 different thalassemia mutations. Clin Genet 1988; 33: 151–155.
Cao A, Galanello R, Rosatelli MC . Prenatal diagnosis and screening of the haemoglobinopathies. Baillieres Clin Haematol 1998; 11: 215–238.
Galanello R, Barella S, Ideo A, et al. Genotype of subjects with borderline hemoglobin A2 levels: implication for beta-thalassemia carrier screening. Am J Hematol 1994; 46: 79–81.
Galanello R, Melis MA, Podda A et al Deletion delta-thalassemia: the 7.2 kb deletion of Corfu delta beta-thalassemia in a non-beta-thalassemia chromosome. Blood 1990; 15: 75:11747–1749.
Loudianos G, Cao A, Pirastu M, Vassilopoulos G, Kollia P, Loukopoulos D . Molecular basis of the delta thalassemia in cis to hemoglobin Knossos variant. Blood 1991; 77: 2087–2088.
Kattamis AC, Camaschella C, Sivera P, Surrey S, Fortina P . Human alpha-thalassemia syndromes: detection of molecular defects. Am J Hematol 1996; 53: 81–91.
Cao A, Rosatelli MC, Monni G, Galanello R . Screening for thalassemia: a model of success. Obstet Gynecol Clin North Am 2002; 29: 305–328, vi-vii.
Mavrou A, Kouvidi E, Antsaklis A, Souka A, Kitsiou Tzeli S, Kolialexi A . Identification of nucleated red blood cells in maternal circulation: a second step in screening for fetal aneuploidies and pregnancy complications. Prenat Diagn 2007; 27: 150–153.
Cheung MC, Goldberg JD, Kan YW . Prenatal diagnosis of sickle cell anaemia and thalassaemia by analysis of fetal cells in maternal blood. Nat Genet 1996; 14: 264–268.
Dhallan R, Guo X, Emche S, et al. A non-invasive test for prenatal diagnosis based on fetal DNA present in maternal blood: a preliminary study. Lancet 2007; 369: 474–481.
Lo YM . Recent advances in fetal nucleic acids in maternal plasma. J Histochem Cytochem 2005; 53: 293–296.
Eleftheriou A . Guidelines for the clinical management of thalassemia. Thalassemia International Federation. Available at: www.thalassaemia.org.cy. Accessed December 31, 2007.
Borgna-Pignatti C . Modern treatment of thalassaemia intermedia. Br J Hematol 2007; 138: 291–304.
Clark PR, Chua-Anusorn W, St Pierre TG . Proton transverse relaxation rate (R2) images of liver tissue; mapping local tissue iron concentrations with MRI corrected. Magn Reson Med 2003; 49: 572–575. Erratum in: Magn Reson Med, 2003; 49: 1201.
Anderson LJ, Holden S, Davis B, et al. Cardiovascular T2-star (T2*) magnetic resonance for the early diagnosis of myocardial iron overload. Eur Heart J 2001; 22: 2171–2179.
Westwood MA, Firmin DN, Gildo M, et al. Intercentre reproducibility of magnetic resonance T2* measurements of myocardial iron in thalassaemia. Int J Cardiovasc Imaging 2005; 21: 531–538.
St Pierre TG, Clark PR, Chua-anusorn W, et al. Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 2005; 105: 855–861.
Anderson LJ, Westwood MA, Holden S, et al. Myocardial iron clearance during reversal of siderotic cardiomyopathy with intravenous desferrioxamine: a prospective study using T2* cardiovascular magnetic resonance. Br J Haematol 2004; 127: 348–355.
Fischer R, Longo F, Nielsen P, Engelhardt R, Hider RC, Piga A . Monitoring long-term efficacy of iron chelation therapy by deferiprone and desferrioxamine in patients with beta-thalassaemia major: application of SQUID biomagnetic liver susceptometry. Br J Haematol 2003; 121: 938–948.
Cohen AR, Galanello R, Piga A, De Sanctis V, Tricta F . Safety and effectiveness of long-term therapy with the oral iron chelator deferiprone. Blood 2003; 102: 1583–1587.
Wanless IR, Sweeney G, Dhillon AP, et al Lack of progressive hepatic fibrosis during long-term therapy with deferiprone in subjects with transfusion-dependent beta-thalassemia. Blood 2002; 100: 1566–1569. Erratum in: Blood, 2003; 101: 2460.
Anderson LJ, Wonke B, Prescott E, Holden S, Walker JM, Pennell DJ . Comparison of effects of oral deferiprone and subcutaneous desferrioxamine on myocardial iron concentrations and ventricular function in beta-thalassaemia. Lancet 2002; 360: 516–520.
Piga A, Gaglioti C, Fogliacco E, Tricta F . Comparative effects of deferiprone and deferoxamine on survival and cardiac disease in patients with thalassemia major: a retrospective analysis. Haematologica 2003; 88: 489–496.
Borgna-Pignatti C, Cappellini MD, De Stefano P, et al. Cardiac morbidity and mortality in deferoxamine- or deferiprone-treated patients with thalassemia major. Blood 2006; 107: 3733–3737.
Ceci A, Baiardi P, Felisi M, et al. The safety and effectiveness of deferiprone in a large-scale, 3-year study in Italian patients. Br J Haematol 2002; 118: 330–336.
Pennell DJ, Berdoukas V, Karagiorga M, et al. Randomized controlled trial of deferiprone or deferoxamine in beta-thalassemia major patients with asymptomatic myocardial siderosis. Blood 2006; 107: 3738–3744.
Maggio A . Light and shadows in the iron chelation treatment of haematological diseases. Br J Haematol 2007; 138: 407–421.
Galanello R . Deferiprone in the treatment of transfusion-dependent thalassemia: a review and perspective. Ther Clin Risk Manag 2007; 3: 795–805.
Neufeld EJ . Oral chelators deferasirox and deferiprone for transfusional iron overload in thalassemia major: new data, new questions. Blood 2006; 107: 3436–3441.
Galanello R, Origa R . Once-daily oral deferasirox for the treatment of transfusional iron overload. Expert Rev Clin Pharmacol 2008; 1: 231–240.
Cappellini MD, Cohen A, Piga A, et al. A phase 3 study of deferasirox (ICL670), a once-daily oral iron chelator, in patients with beta-thalassemia. Blood 2006; 107: 3455–3462.
Wonke B, Wright C, Hoffbrand AV . Combined therapy with deferiprone and desferrioxamine. Br J Haematol 1998; 103: 361–364.
Origa R, Bina P, Agus A, et al. Combined therapy with deferiprone and desferrioxamine in thalassemia major. Haematologica 2005; 90: 1309–1314.
Tanner MA, Galanello R, Dessi C, et al. A randomized, placebo-controlled, double-blind trial of the effect of combined therapy with deferoxamine and deferiprone on myocardial iron in thalassemia major using cardiovascular magnetic resonance. Circulation 2007; 115: 1876–1884.
Porcu M, Landis N, Salis S, et al. Effects of combined deferiprone and desferrioxamine iron chelating therapy in beta-thalassemia major end-stage heart failure: a case report. Eur J Heart Fail 2007; 9: 320–322.
Tanner MA, Galanello R, Dessì C, et al. Combined deferiprone and desferrioxamine iron chelating therapy in beta-thalassemia major for the treatment of severe myocardial siderosis with left ventricular dysfunction. J Cardiovasc Magn Reson 2008; 10: 12.
Maggio A, Vitrano A, Capra M, et al. Long-term sequential deferiprone-deferoxamine versus deferiprone alone for thalassaemia major patients: a randomized clinical trial. Br J Haematol 2009; 145: 245–254.
Davis BA, O'Sullivan C, Jarritt PH, Porter JB . Value of sequential monitoring of left ventricular ejection fraction in the management of thalassemia major. Blood 2004; 104: 263–269.
Wood JC, Origa R, Agus A, Matta G, Coates TD, Galanello R . Onset of cardiac iron loading in pediatric patients with thalassemia major. Haematologica 2008; 93: 917–920.
Gaziev J, Lucarelli G . Stem cell transplantation for hemoglobinopathies. Curr Opin Pediatr 2003; 15: 24–31.
La Nasa G, Argiolu F, Giardini C, et al. Unrelated bone marrow transplan-tation for beta-thalassemia patients: the experience of the Italian Bone Marrow Transplant Group. Ann N Y Acad Sci 2005; 1054: 186–195.
Locatelli F, Rocha V, Reed W, et al. Related umbilical cord blood transplantation in patients with thalassemia and sickle cell disease. Blood 2003; 101: 2137–2143.
Walters MC, Quirolo L, Trachtenberg ET, et al. Sibling donor cord blood transplantation for thalassemia major: experience of the Sibling Donor Cord Blood Program. Ann N Y Acad Sci 2005; 1054: 206–213.
Orofino MG, Argiolu F, Sanna MA, et al. Fetal HLA typing in beta thalassaemia: implications for haemopoietic stem-cell transplantation. Lancet 2003; 362: 41–42.
Pace BS, Zein S . Understanding mechanisms of gamma-globin gene regulation to develop strategies for pharmacological fetal hemoglobin induction. Dev Dyn 2006; 235: 1727–1737.
Quek L, Thein SL . Molecular therapies in beta-thalassaemia. Br J Haematol 2007; 136: 353–365.
Bradai M, Abad MT, Pissard S, Lamraoui F, Skopinski L, de Montalembert M . Hydroxyurea can eliminate transfusion requirements in children with severe beta-thalassemia. Blood 2003; 102: 1529–1530.
Yavarian M, Karimi M, Bakker E, Harteveld CL, Giordano PC . Response to hydroxyurea treatment in Iranian transfusion-dependent beta-thalassemia patients. Haematologica 2004; 89: 1172–1178.
Sadelain M, Boulad F, Galanello R, et al. Therapeutic options for patients with severe beta-thalassemia: the need for globin gene therapy. Hum Gene Ther 2007; 18: 1–9.
Rivella S, May C, Chadburn A, Rivière I, Sadelain M . A novel murine model of Cooley anemia and its rescue by lentiviral-mediated human beta-globin gene transfer. Blood 2003; 101: 2932–2939.
Puthenveetil G, Scholes J, Carbonell D, et al. Successful correction of the human beta-thalassemia major phenotype using a lentiviral vector. Blood 2004; 104: 3445–3453.
Chang JC, Ye L, Kan YW . Correction of the sickle cell mutation in embryonic stem cells. Proc Natl Acad Sci U S A 2006; 103: 1036–1040.
Takahashi K, Tanabe K, Ohnuki M, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007; 131: 861–872.
Wernig M, Meissner A, Foreman R, et al. In vitro reprogramming of bibroblasts into a pluripotent ES-cell-like state. Nature 2007; 448: 318–324.
Hanna J, Wernig M, Markoulaki S, et al. Treatment of sickle cell anemia mouse model with iPS cells generated from autologous skin. Science 2007; 318: 1920–1923.
Acknowledgements
This study was supported by Grants from L.R.7 2007 Regione Autonoma Sardegna.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure: The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Cao, A., Galanello, R. Beta-thalassemia. Genet Med 12, 61–76 (2010). https://doi.org/10.1097/GIM.0b013e3181cd68ed
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1097/GIM.0b013e3181cd68ed
Keywords
This article is cited by
-
Base Editors-Mediated Gene Therapy in Hematopoietic Stem Cells for Hematologic Diseases
Stem Cell Reviews and Reports (2024)
-
CRISPR/Cas9, a promising approach for the treatment of β-thalassemia: a systematic review
Molecular Genetics and Genomics (2023)
-
SMPD1 gene variants in patients with β-Thalassemia major
Molecular Biology Reports (2023)
-
Vitamin D levels and left ventricular function in beta-thalassemia major with iron overload
European Journal of Pediatrics (2023)
-
Pattern and clinical correlates of renal iron deposition in adult beta-thalassemia major patients
Clinical and Experimental Medicine (2023)
