
Abstract
Purpose: Two common variant alleles of the cytochrome CYP2C9 (CYP2C9*2 and CYP2C9*3) lead to reduced warfarin metabolism in vitro and in vivo. The study objective was to examine the strength and quality of existing evidence about CYP2C9 gene variants and clinical outcomes in warfarin-treated patients.
Methods: The study was a systematic review and meta-analysis. Multiple electronic databases were searched, references identified from bibliographies were sought, and experts and authors of primary studies were also contacted. Strict review inclusion criteria were determined. Three reviewers independently extracted data using prepiloted proformas.
Results: In all, 11 studies meeting review inclusion criteria were identified (3029 patients). Nine were included in the meta-analyses (2775 patients). Random effects meta-analyses were performed; statistical heterogeneity and inconsistency was assessed. Twenty percent of patients studied carry a variant allele: CYP2C9*2 12.2% (9.7%–15.0%) and CYP2C9*3, 7.9% (6.5%–9.7%). Mean difference in daily warfarin dose: for CYP2C9*2, the reduction was 0.85 mg (0.60–1.11 mg), a 17% reduction. For CYP2C9*3, the reduction was 1.92 mg (1.37–2.47 mg), a 37% reduction. For CYP2C9*2 or *3, the reduction was 1.47 mg (1.24–1.71 mg), a 27% reduction. The relative bleeding risk for CYP2C9*2 was 1.91 (1.16–3.17) and for CYP2C9*3 1.77 (1.07–2.91). For either variant, the relative risk was 2.26 (1.36–3.75).
Conclusions: Patients with CYP2C9*2 and CYP2C9*3 alleles have lower mean daily warfarin doses and a greater risk of bleeding. Testing for gene variants could potentially alter clinical management in patients commencing warfarin. Evidence for the clinical utility and cost-effectiveness of genotyping is needed before routine testing can be recommended.
Similar content being viewed by others

Main
The cytochrome P450 complex is a group of hepatic microsomal enzymes responsible for the oxidative metabolism of various substrates and the synthesis of cholesterol and other lipids.1 The CYP2C9 isoenzyme is primarily responsible for the metabolism of a number of important drugs, including warfarin, phenytoin, losartan, tolbutamide, glipizide, and diclofenac. The gene coding for CYP2C9 has been mapped to the long arm of chromosome 10 (10q24.2), within a cluster of cytochrome P450 genes.2
GENE VARIANTS
Around 12 CYP2C9 variants have now been identified (http://www.imm.ki.SE/CYPalleles/). The most common variant is considered to be the wild-type allele, CYP2C9*1. Two variants are known to reduce the metabolism of warfarin: CYP2C9*2 by 30% to 50% and CYP2C9*3 by around 90%.1,3 The functional significance of the other alleles has yet to be fully determined. Over 30% of European and Caucasian populations have one or both of the CYP2C9*2 or CYP2C9*3 alleles, with allele frequencies of 0.1 and 0.08, respectively.3 However, these two variants are extremely rare in Asian and African American populations, with over 95% of these populations expressing the wild-type genotype. Other variant alleles (CYP2C9*4-*6 and CYP2C9*11) have population allele frequencies of 0.01 or less, with the frequencies of other alleles (CYP2C9*7-*10) still to be established.1
CLINICAL CONTEXT
Warfarin is now commonly used for the prevention of arterial and venous thromboembolism.4,5 It is a difficult drug to manage because of its narrow therapeutic index and because patients' response to warfarin is highly variable: it is influenced by ageing, coprescribed drugs, diet, alcohol consumption, and comorbid conditions.
Bleeding remains the most serious complication despite the adoption of less intensive anticoagulation target levels, specialist anticoagulant clinics, and computerized systems for dose adjustment. In the ISCOAT prospective study of bleeding risk on warfarin therapy, bleeding complications occurred at a rate of 8 per 100 patient years.6
Several studies have examined the effect of CYP2C9 variants on warfarin dose requirements, measures of anticoagulation control, and bleeding risk. Some studies have shown that patients with gene variants require lower maintenance doses and have a greater risk of bleeding than wild type. The purpose of this study is to examine the strength and quality of existing evidence about the relationship between common CYP2C9 gene variants and clinical outcomes in warfarin-treated patients. This study is the first systematic review and meta-analysis of this topic.
SYSTEMATIC REVIEW AND META-ANALYSIS METHODS
This review was conducted using guidance from the Cochrane Collaboration and the Centre for Reviews and Dissemination, with reference to recently published guidance from the Human Genome Epidemiology Network for reporting gene-disease associations.7–9
Review inclusion criteria
Studies were included that recruited patients commencing or established on warfarin who were tested for CYP2C9 variants from anticoagulant clinics or their equivalent. A study had to report at least one of the following outcome measures: drug dose, indicators of anticoagulation control, and bleeding events.
A number of studies used the Fihn criteria for classifying anticoagulant-related bleeding events, although they were not used in all studies.10 We therefore combined bleeding events from studies however they were defined. We did not analyze the severity of bleeding events because of differences in classification between studies, the small number of studies reporting bleeding events, and the small number of events reported in total.
Search strategy
PUBMED (Medline, using MeSH headings and text words) was searched from 1980 (the year that CYP2C9 gene was sequenced) to 2003; EMBASE (subject headings and text words) was searched from 1980 to 2003. The search terms are contained in the Appendix. The Human Genome Epidemiology network database, the Cochrane Library, and the Database of Abstracted Reviews of Effects were also systematically searched. All databases were searched between January 21 and 23, 2003. Reference lists of nonsystematic reviews and primary studies were scrutinized. Study authors and experts were contacted in an attempt to find unpublished studies, to obtain additional data, or to answer specific questions about study methodology or results.
Data extraction
Two reviewers (S.S. and J.E.) independently extracted data from identified studies using prepiloted proformas. Reviewers compared results and resolved any differences by discussion. A third reviewer (J.H.) also extracted numerical data required for meta-analysis, which were then confirmed by S.S.
Assessment of study quality
No quantitative methods were used to rate quality but the following quality indicators were abstracted7–9,11: (1) adequate description of the study population; (2) a clear description of study design and recruitment methods; (3) case and/or control group definitions, inclusion and exclusion criteria; (4) the proportion of recruited subjects included in the analysis and how excluded subjects were dealt with; (5) description of genotyping methods used and quality control measures; (6) appropriate blinding of investigators to study outcomes; (7) a statement of how ethnicity was dealt with in study populations; and (8) data ascertainment methods (e.g., medical records, self-report).
Statistical analysis
Hardy Weinberg equilibrium (HWE) for the six genotypes was tested within each study using Pearson chi-squared goodness-of-fit test, treating 2C9*2 and *3 as different alleles at the same locus. HWE was tested across studies for each polymorphism separately using the Wald-type test proposed by Troendle and Yu.12 Random effect meta-analyses were conducted to provide combined estimates of allele frequencies. The analyses reported below are random effects meta-analyses of the mean difference in daily warfarin dose and the relative risk of bleeding. We compared 2C9*2 carriers with non-2C9*2 carriers, 2C9*3 carriers with noncarriers and carriers of 2C9*2 or *3 (or carriers of both *2 and *3) with carriers of neither.
Statistical heterogeneity was measured using conventional methods and a newer measure, called I2. I2 is a measure of inconsistency across studies that is essentially independent of the number of studies and the choice of effect measure (unlike the Cochran q test or the among-study variance). It describes the degree of variation attributable to heterogeneity rather than sampling error and is reported as a percentage.13,14
RESULTS
Study inclusion and characteristics
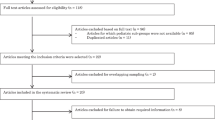
Table 1 describes the characteristics of the 11 primary studies that met the review's inclusion criteria.15–25 Details of the study setting, design, and patient profiles are included. Ten of the eleven studies were performed in Caucasian patients, so that stratification by ethnic group is not possible from the data. No unpublished studies were identified from our contact with the authors of primary studies and experts in this discipline. Leung's study in Hong Kong Chinese patients was excluded from the meta-analysis because it investigated novel CYP2C9 gene variants22 and because the nonspecific primers used in this study have been questioned.26 Freeman's research group conducted a pilot study and a larger, definitive study, with their results published separately.19,23 We have been unable to ascertain whether the pilot study results were included with the later results. We have assumed that they were and so have only used data from the later study.
The study by Ogg was a post hoc analysis of a convenience sample of subjects from the Thrombosis Prevention Trial, measuring wild-type and 2C9*3 alleles only.17 Furuya (the first known published study linking CYP2C9 and warfarin dose in vivo) measured only wild-type and 2C9*2 alleles.15 Nine separate studies investigating CYP2C9 variants and warfarin-related outcomes were therefore available for meta-analysis (2775 subjects).
Genotype and allele frequencies
Approximately one-fifth of the Caucasian warfarin-treated patients studied carried a variant allele (Table 2). The combined allele frequency for 2C9*2 is 12.2% (9.9%–15.0%) and 7.9% (6.5%–9.7%) for 2C9*3. There is some evidence of nonconformity to HWE for the Higashi study only; its impact was assessed in sensitivity analysis (see later sections).
Daily warfarin dose and genotype
Eight studies were included in this analysis16–18,20,21,23–25 (Figs. 1–3). Subjects who carry at least one copy of a variant allele have a lower mean daily dose compared to wild type: 2C9*2, 0.85 mg less (0.60–1.11, 8 studies, heterogeneity chi-squared = 5.34, I2 = 0%), a percentage reduction of 17%; 2C9*3, 1.92 mg less (1.37–2.47, 8 studies; heterogeneity chi-squared = 36.9; I2 = 81%), a percentage reduction of 37%; and 2C9*2 or *3, 1.47 mg less (1.24–1.71, 7 studies; heterogeneity chi-squared = 22.2; I2 = 73%), a percentage reduction of 27%.

Mean daily dose reduction 2C9*2.

Mean daily dose reduction 2C9*2 or 2C9*3.
Bleeding risk and genotype
Four studies measured the occurrence of bleeding events (Fig. 4).16,17,20,25 Of these, only three reported bleeding risk by genotype.17,20,25 The fourth article reported bleeding risk for patients in a predefined low-dose category, (< 1.5 mg daily) rather than by genotype and so was excluded from the meta-analysis.16 The reported relative risks (RR) are combinations of rate ratios and risk ratios.

Relative risk for bleeding.
Subjects who carry at least one copy of a variant allele have an increased relative risk of bleeding compared with noncarriers of that allele: 2C9*2 RR = 1.91 (1.16–3.17, 2 studies); 2C9*3 RR = 1.77 (1.07–2.91, 3 studies); 2C9*2 or *3 RR = 2.26 (1.36–3.75, 2 studies).
DISCUSSION
This systematic review shows that variant alleles are common in Caucasian warfarin-treated patients, with around 20% of patients carrying at least one variant. There is strong and consistent evidence for a lower maintenance dose for patients with either 2C9 variant, with on average, the lowest requirement for patients with 2C9*3. In the studies reporting bleeding events, the risk of bleeding is approximately doubled for patients with a variant allele. It is possible that the small number of studies examining bleeding events may only have been reported because of the magnitude of effect observed.
There is considerable variation in the effect of genotype on dose requirements in two of the three meta-analyses. In particular, when comparing 2C9*3 with the wild type, approximately 81% of the observed variation appears to be due to genuine differences among the studies (Fig. 2). Thus the exact degree to which a variant allele is associated with a lower warfarin dose may be unpredictable. Inconsistency in the results of gene-disease association studies is a well-known problem, especially when studies are small.27 Despite the lack of agreement in the size of the reduction in dose requirement, we have found that the direction of effect is consistent across all studies, and the high value of I2 does not affect our fundamental conclusion. Indeed, we have observed that accumulation of evidence on the association has confirmed early reported results, a valuable finding that can arise from a meta-analytic approach.28 Unfortunately, we did not have sufficient studies to examine the dependence of genotype effects on characteristics of the studies (such as design) or participants (such as ethnicity). These may be key causes of the bias or variability in results. However, methods for investigating heterogeneity are not reliable.29

Mean daily dose reduction 2C9*3.
We believe that we have identified all available studies through a comprehensive and sensitive search strategy and by seeking unpublished data from study authors. We have not used common measures of publication bias (such as funnel plots) because of the low number of studies in the review.
Most studies were conducted in Caucasian patients, with some using specific population restrictions. This is important because 2C9*2 and 2C9*3 alleles are extremely rare in African American and most Asian populations. Further study to identify new alleles in these populations is needed, particularly as many Asian patients are much more sensitive to warfarin than Caucasian patients.22
There is evidence of nonconformity to HWE for the Higashi study only. The study reported that the frequency of 2C9*3 homozygotes was four times greater than expected under HWE. Possible explanations provided by the authors are that they used direct sequencing of exons 3 and 7, compared to previous studies that used restriction enzyme techniques. Sequencing is felt to be more accurate, implying that previous studies may have underestimated the frequency of the 2C9*3 allele. However, the authors do not state whether they excluded genotyping errors from their own analysis. Another possible explanation is selection bias, with the 2C9*3 allele being overrepresented in this study population (or underrepresented in previous studies) because of local referral patterns, although the authors found no supporting evidence for this possibility. The conclusions from all meta-analyses are robust to the exclusion of this study.
Most studies provide little information to explore interactions between genotype and nongenetic factors (such as age, coprescribed drugs, coexisting disease, diet, or consumption of alcohol) on daily dose requirements or bleeding risk. These factors may modify the effect of genotype on warfarin metabolism and warfarin-related treatment outcomes, so it is possible that much of the variability of a patients response to warfarin is “environmental” rather than “genetic.”30 We were unable to investigate this further because of the limitations in the way primary studies were conducted and reported.
The evidence for the impact of genotype on risk of bleeding is less clear. Three studies contributed to the meta-analysis17,20,25 and together suggested an approximate doubling of risk.16,17,25 In addition, Aithal16 found that patients on low dose warfarin (< 1.5 mg) had a greater chance of having both a variant allele and an increased risk of bleeding.
Several studies related gene variants or risk of bleeding to intensity of anticoagulation. Higashi25 found evidence for an association between variant alleles and a higher risk of over-anticoagulation. However, the study by Margaglione20 found that the higher risk of bleeding did not coincide with raised INR results but was observed in patients with potential sources of bleeding such as fibroids or gastrointestinal polyps carrying variant alleles. The study by Taube18 did not find any relationship between over-anticoagulation and bleeding in patients with variant alleles although very few episodes of over-anticoagulation were reported and there were no bleeding events. However, the study population included only stable patients with a low target INR of 2.5.
These conflicting results could be explained by differences in treatment and monitoring regimens in different treatment centers, the selection criteria for study populations (especially whether all patients on warfarin are included, only those who are stable, or only those who have low target INRs: only four studies had unrestricted INR inclusion criteria), the distribution of interacting environmental factors in study populations, and the fact that bleeding is an uncommon adverse event. These factors may lead to an underestimation of the risk of bleeding in these studies. A risk of bleeding unrelated to the intensity of anticoagulation is not easily explained, unless the CYP2C9 locus has other (unknown) effects on hemostasis. It has been argued that once treatment is stabilized, patients with variant alleles are not more prone to over-anticoagulation and bleeding than patients without variant alleles.30
IMPLICATIONS
We would suggest that no more studies confirming the association of CYP2C9 genotype and warfarin dose requirements are required in Caucasian patients. Dosing in other ethnic groups has not been well studied and there may be other important genetic variants in these groups. Studies are needed to clarify the interaction of CYP2C9 genotypes and other factors such as age, comorbidity, drugs, and alcohol consumption.
Genotyping warfarin-treated patients who are stable is probably unnecessary because these patients can be adequately managed on the basis of phenotypic tests (INR) and relevant factors from the patient's clinical history. It is likely that the use of more rigorous warfarin nomograms and intensive monitoring during high-risk periods, with preemptive dose reductions when necessary, might be a more effective and pragmatic way of reducing the risk of adverse events without the need for genotyping.
There are two possible roles for genotyping. First, CYP2C9 testing could identify high-risk patients who might benefit from conservative induction regimens, lower maintenance doses, and more frequent clinical and laboratory monitoring. Second, genotyping may also assist the choice of drug for patients considering “elective” anticoagulation; for example, for nonrheumatic atrial fibrillation. Patients with variant genotypes (especially those with the 2C9*3 allele) may choose an alternative drug, such as aspirin. Direct thrombin inhibitors are also in development and these could provide another alternative once available.31
However, evidence presented in this review is insufficient to make a case for genotyping in routine clinical practice yet because it focuses on the association between CYP2C9 gene variants and clinical outcomes, thus providing important information on clinical validity. Specifically, we require evidence of clinical utility (the likelihood that the test will lead to an improved health outcome) and cost-effectiveness of CYP2C9 genotyping compared to current care (based on phenotypic testing).32
A randomized trial of CYP2C9 genotyping and anticoagulation may make generating this evidence difficult because of the large number of patients required to demonstrate any reduction on rare adverse events, such as bleeding and the introduction of direct thrombin inhibitors may replace warfarin in clinical practice. Also, a clearly defined intervention and a test providing rapid results are needed to enable genotyping to have an impact on clinical management.
Data presented in this review could provide a basis for modeling the impact of genotyping. However, the key outcome (the number of bleeding events prevented by genotyping before starting warfarin and altered clinical management) could only be estimated (assuming that such a benefit exists) and assessed using sensitivity analysis. Pilot studies could be used to provide such estimates for modeling.
This study provides an illustration of the potential and problems of pharmacogenetics. Although there appears to be the possibility of tailoring drugs to patients and preventing adverse reactions, it is unclear in practice whether these benefits will be achieved. These benefits could be achieved through more intensive management based on phenotypic testing. It is not clear what the added value of genotyping would be in this case, but additional studies may clarify this issue.
References
Lee CR, Goldstein JA, Pieper JA . Cytochrome P450 2C9 polymorphisms: A comprehensive review of the in-vitro and human data. Pharmacogenetics 2002; 12: 251–263.
Goldstein JA, de Morais SM . Biochemistry and molecular biology of the human CYP2C subfamily. Pharmacogenetics 1994; 4: 285–299.
Daly AK, King BP . Pharmacogenetics of oral anticoagulants. Pharmacogenetics 2003; 13: 1–6.
Hirsh J, Dalen JE, Deykin D, Poller L, Bussey H . Oral anticoagulants. Mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest 1995; 108: 231S–246S.
Guidelines on oral anticoagulation: third edition. Br J Haematol 1998; 101: 374–387.
Palareti G, Leali N, Coccheri S, Poggi M, Manotti C, D'Angelo A et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Italian Study on Complications of Oral Anticoagulant Therapy. Lancet 1996; 348: 423–428.
Alderson P, Green S, Higgins JP . The Cochrane Reviewers' Handbook; v 4.2.2. The Cochrane Collaboration, Issue 1; 2004.
Centre for Reviews and Dissemination. Undertaking Systematic Reviews of Research on Effectiveness CRD's Guidance for those Carrying Out or Commissioning Reviews CRD Report Number 4 (2nd Edition). Centre for Reviews and Dissemination; 2001.
Little J, Bradley L, Bray MS, Clyne M, Dorman J, Ellsworth DL et al. Reporting, appraising, and integrating data on genotype prevalence and gene-disease associations. Am J Epidemiol 2002; 156: 300–310.
Fihn SD, Callahan CM, Martin DC, McDonell MB, Henikoff JG, White RH . The risk for and severity of bleeding complications in elderly patients treated with warfarin. The National Consortium of Anticoagulation Clinics. Ann Intern Med 1996; 124: 970–979.
Juni P, Witschi A, Bloch R, Egger M . The hazards of scoring the quality of clinical trials for meta-analysis. JAMA 1999; 282: 1054–1060.
Troendle JF, Yu KF . A note on testing the Hardy-Weinberg law across strata. Ann Hum Genet 1994; 58: 397–402.
Higgins JP, Thompson SG, Deeks JJ, Altman DG . Measuring inconsistency in meta-analyses. BMJ 2003; 327: 557–560.
Higgins JPT, Thompson SG . Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: 1539–1558.
Furuya H, Fernandez-Salguero P, Gregory W, Taber H, Steward A, Gonzalez FJ et al. Genetic polymorphism of CYP2C9 and its effect on warfarin maintenance dose requirement in patients undergoing anticoagulation therapy. Pharmacogenetics 1995; 5: 389–392.
Aithal GP, Day CP, Kesteven PJ, Daly AK . Association of polymorphisms in the cytochrome P450 CYP2C9 with warfarin dose requirement and risk of bleeding complications. Lancet 1999; 353: 717–719.
Ogg MS, Brennan P, Meade T, Humphries SE . CYP2C9*3 allelic variant and bleeding complications. Lancet 1999; 354: 1124.
Taube J, Halsall D, Baglin T . Influence of cytochrome P-450 CYP2C9 polymorphisms on warfarin sensitivity and risk of over-anticoagulation in patients on long-term treatment. Blood 2000; 96: 1816–1819.
Freeman BD, Zehnbauer BA, McGrath S, Borecki I, Buchman TG . Cytochrome P450 polymorphisms are associated with reduced warfarin dose. Surgery 2000; 128: 281–285.
Margaglione M, Colaizzo D, D'Andrea G, Brancaccio V, Ciampa A, Grandone E et al. Genetic modulation of oral anticoagulation with warfarin. Thromb Haemost 2000; 84: 775–778.
Loebstein R, Yonath H, Peleg D, Almog S, Rotenberg M, Lubetsky A et al. Interindividual variability in sensitivity to warfarin–Nature or nurture?. Clin Pharmacol Ther 2001; 70: 159–164.
Leung AY, Chow HC, Kwong YL, Lie AK, Fung AT, Chow WH et al. Genetic polymorphism in exon 4 of cytochrome P450 CYP2C9 may be associated with warfarin sensitivity in Chinese patients. Blood 2001; 98: 2584–2587.
Tabrizi AR, Zehnbauer BA, Borecki IB, McGrath SD, Buchman TG, Freeman BD . The frequency and effects of cytochrome P450 (CYP) 2C9 polymorphisms in patients receiving warfarin. J Am Coll Surg 2002; 194: 267–273.
Scordo MG, Pengo V, Spina E, Dahl ML, Gusella M, Padrini R . Influence of CYP2C9 and CYP2C19 genetic polymorphisms on warfarin maintenance dose and metabolic clearance. Clin Pharmacol Ther 2002; 72: 702–710.
Higashi MK, Veenstra DL, Kondo LM, Wittkowsky AK, Srinouanprachanh SL, Farin FM et al. Association between CYP2C9 genetic variants and anticoagulation-related outcomes during warfarin therapy. JAMA 2002; 287: 1690–1698.
Rettie AE, Tai G, Veenstra DL, Farin FM, Srinouanprachan S, Lin YS et al. CYP2C9 exon 4 mutations and warfarin dose phenotype in Asians. Blood 2003; 101: 2896–2897.
Ioannidis JP, Ntzani EE, Trikalinos TA, Contopoulos-Ioannidis DG . Replication validity of genetic association studies. Nat Genet 2001; 29: 306–309.
Lohmueller KE, Pearce CL, Pike M, Lander ES, Hirschhorn JN . Meta-analysis of genetic association studies supports a contribution of common variants to susceptibility to common disease. Nat Genet 2003; 33: 177–182.
Thompson SG, Higgins JP . How should meta-regression analyses be undertaken and interpreted?. Stat Med 2002; 21: 1559–1573.
Baglin T . Avoiding overanticoagulation: pharmacogenomics or pragmatism?. Thromb Haemost 2001; 85: 945–946.
Hirsh J . New anticoagulants. Am Heart J 2001; 142: S3–S8.
Burke W, Atkins D, Gwinn M, Guttmacher A, Haddow J, Lau J et al. Genetic test evaluation: information needs of clinicians, policy makers, and the public. Am J Epidemiol 2002; 156: 311–318.
Author information
Authors and Affiliations
Appendices
Appendix
Search Strategies
PUBMED MeSH search
(1) Anticoagulants [exp]; (2) Warfarin [exp]; (3) 1 or 2; (4) Cytochromes [exp]; (5) Cytochrome P-450 enzyme system [exp]; (6) 4 or 5; (7) Genotype [exp]; (8) Genes [exp]; (9) Alleles [exp]; (10) Polymorphism (genetics) [exp]; (11) 7 or 8 or 9 or 10; (12) 3 and 6 and 11
PUBMED Text word search
(1) Warfarin; (2) S-warfarin; (3) 1 or 2; (4) Cytochrome*; (5) Cytochrome-P450*; (6) Cytochrome P450; (7) Cytochrome P-450; (8) CYP2C9*; (9) 4 or 5 or 6 or 7 or 8; (10) Genotyp*; (11) Gene*; (12) Allele*; (13) Polymorphism*; (14) 10 or 11 or 12 or 13; (15) 3 and 9 and 14
EMBASE Subject heading search
(1) exp Anticoagulant Agent/ (160845); (2) exp WARFARIN/ (17212); (3) 1 or 2 (160845); (4) exp Cytochrome/ (40164); (5) exp Cytochrome P450/ (21207); (6) 4 or 5 (40164); (7) exp GENOTYPE/ or exp GENOTYPE PHENOTYPE CORRELATION/ (39911); (8) exp Gene/ (140346); (9) exp Allele/ (24647); (10) exp GENETIC POLYMORPHISM/ (74357); (11) 7 or 8 or 9 or 10 (241961); (12) 3 and 6 and 11 (177); (13) from 12 keep 1–177 (177)
EMBASE Text word search
(1) warfarin.mp.; (2) seconds-warfarin.mp.; (3) 1 or 2; (4) cytochrome$.mp.; (5) cytochrome P450.mp.; (6) cytochrome P-450.mp.; (7) cytochrome-P450.mp.; (8) CYP2C9$.mp.; (9) 4 or 5 or 6 or 7 or 8; (10) genotyp$.mp.; (11) gene$.mp.; (12) allele$.mp.; (13) polymorphism$.mp.; (14) 10 or 11 or 12 or 13; (15) 3 and 9 and 14; (16) from 15 keep 1–248
Appendix 1
Rights and permissions
About this article
Cite this article
Sanderson, S., Emery, J. & Higgins, J. CYP2C9 gene variants, drug dose, and bleeding risk in warfarin-treated patients: A HuGEnet™ systematic review and meta-analysis. Genet Med 7, 97–104 (2005). https://doi.org/10.1097/01.GIM.0000153664.65759.CF
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1097/01.GIM.0000153664.65759.CF
Keywords
This article is cited by
-
Association between gene polymorphisms and initial warfarin therapy in patients after heart valve surgery
Pharmacological Reports (2024)
-
CYP2C9 Polymorphisms and the Risk of Cardiovascular Events in Patients Treated with Clopidogrel: Combined Data from the POPular Genetics and POPular AGE Trials
American Journal of Cardiovascular Drugs (2023)
-
Genetic-guided pharmacotherapy for venous thromboembolism: a systematic and critical review of economic evaluations
The Pharmacogenomics Journal (2021)
-
Incidence, preventability, and causality of adverse drug reactions at a university hospital emergency department
European Journal of Clinical Pharmacology (2021)
-
CYP450 polymorphisms and clinical pharmacogenetics of ibuprofen after lower third molar extraction
European Journal of Clinical Pharmacology (2021)
