
Abstract
Purpose: The response of academic Departments of Medicine (DOM), who train the bulk of future US internists, to the increasing importance of clinical genetics is not known.
Methods: A survey was distributed to 153 DOM chairpersons assessing the current and future roles of clinical genetics as related to internal medicine.
Results: Eighty-five (56%) surveys with complete data were returned. A minority of DOM currently employ geneticists; most genetics education and services are provided by nongeneticists; the general competency of internists to deliver genetic services is unclear.
Conclusions: Academic DOM have limited faculty expertise in clinical genetics; this may impact the ability to integrate genetics into internal medicine practice and training.
Similar content being viewed by others

Main
Continuing progress in the field of genetics impacts many areas of clinical medicine. Already there are over 920 diseases for which genetic tests are available on a clinical and research basis1 and a number of “common diseases” including certain cardiovascular diseases and cancers, for instance, have been shown to have strong genetic components. Furthermore, prestigious clinical journals now routinely publish manuscripts about genetic topics and their clinical impacts. Recently, Francis Collins and Victor McKusick wrote that, “Genomic medicine holds the ultimate promise of revolutionizing the diagnosis and treatment of many illnesses.”2 Although this “revolution” promises to affect virtually all clinical disciplines, the delivery of genetic services has historically been most active in the prenatal and pediatric arenas. The majority of current board-certified clinical geneticists (BCCG) have background training in pediatrics. Geneticists with prior formal training in adult medicine (internists and family practitioners) are a distinct minority and the integration of genomic medicine in adult clinical fields is less well established.
Internists, trained to care primarily for adult patients, are arguably less prepared to adequately meet the new challenges posed by genomic medicine. Several authors have reported that internists are less familiar with genetics and perform less well on assessments of genetic knowledge than other primary care providers (pediatricians, family practitioners, and obstetricians).3–5 The American Board of Internal Medicine (ABIM) does not offer formal subspecialty training in clinical genetics, and academic Departments of Medicine (DOM), responsible for training the bulk of future internists in the United States, are provided with limited guidance in how to best incorporate genetics into the field of adult medicine. Traditionally, genetics training programs (previously fellowship-training, and more recently residency-training) have been provided by pediatric-department based genetics departments. Overall, the current state of clinical genetics practice and education, and the future of clinical genetics in DOMs are incompletely known.
METHODS
To address some of these questions a survey tool was developed and distributed to chairpersons of 153 DOM across the United States. The mailing list of departments was provided by the Department of Medicine at the University of Colorado, which did not otherwise participate in the survey. The mailing list was generated from contact information in the Directory of American Medical Education 2000 to 2001, and included largely departments associated with residency training programs.6 The institutional review board at the University of Colorado Health Sciences Center approved the study. In addition to reporting the total number of faculty within their departments, chairpersons were asked to indicate whether their institution had a clinical genetics department/division within or external to the DOM, whether training internal medicine residents received formal didactic instruction about “specific genetic conditions,” and which type of faculty (general internists, subspecialty internists, board-certified clinical geneticists [BCCG]) coordinated the following for “adult patients with genetic conditions”: genetic diagnosis, genetic information, management of genetic disease, and family screening/counseling services. The chairpersons were asked to evaluate seven statements about the current and future role of clinical genetics in DOM; responses were scored using an adapted Likert scale (Table 1). The term “genetics” was not formally defined as the author wanted to avoid biasing the survey with either broad (“all diseases are genetic or have genetic component”) or narrow (restricted only to Mendelian diseases) definitions of the term. Finally, the chairpersons were asked whether they employed genetic counselors and whether they had any “formal plans” to hire a clinical geneticist within the “coming two years”.
RESULTS
Ninety-two (60%) DOM chairpersons returned surveys by mail or fax, of which 85 (56%) contained sufficient data for analysis and represented the sample study. The average number of reported faculty per DOM was 169 (median 125). Sixteen (19%) of respondents reported having a division of “Adult Genetics” within their DOM and eighteen (21%) reported having DOM faculty who were board certified in clinical genetics (range 1–4 for such faculty). Fifty (59%) of those surveyed indicated that their medical center had a department/division of genetics external to their DOM and twenty (24%) of the DOM employed genetic counselors.
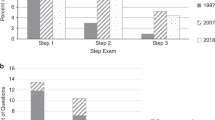
Eighty-three (98%) respondents indicated that they had a residency-training program at their center (remainder being affiliated with training program), and at sixty-four (77%) of these centers, interns and residents attended “formal didactic sessions about specific genetic conditions.” These didactic sessions were taught by general internists (28/83: 34%), internal medicine subspecialists (47/83: 57%), BCCG within the DOM (10/83; 12%), and BCCGs external to a DOM (21/83; 25%). Adult patients with genetic conditions received genetic services from a number of sources (Fig. 1): for the “diagnosis of genetic conditions,” 52% (44/85) primary care internists (PCPs), 65% (55/85) subspecialists (SS), 15% (13/85) DOM BCCG, and 61% (52/85) non-DOM BCCG; for “information about genetic conditions,” 48% (41/85) PCPs, 66% (56/85) SS, 21% (18/85) DOM BCCG, 54% (46/85) non-DOM BCCG, and 36% (31/85) Genetic Counselors (GC); for “management of genetic conditions,” 61% (52/85) PCPs, 75% (64/85) SS, 18% (15/85) DOM BCCG, and 46% (39/85) non-DOM BCCG; for “family screening/counseling of genetic conditions,” 48% (41/85) PCPs, 54% (46/85) SS, 19% (16/85) DOM BCCG, 47% (40/85) non- DOM BCCG, and 43% (37/85) GCs (numbers add to > 100% as some services were delivered from more than one source). Thirty-two (32/85, 38%) chairpersons indicated that “inpatient consultations for genetic conditions in adults” were available at their medical centers.

Genetic services adult patients: who delivers the care. Responses of chairpersons to questions of which physicians, in the DOM, is responsible for delivering the following genetic services: “genetic diagnoses,” “genetic information,” “management of genetic conditions,” and “genetic screening/counseling.” Responses sum to > 100%, as more than one provider delivered some services.
A majority (75/83, 90%) of DOM chairpersons agreed that the majority of genetic diagnoses (being made in their DOMs) were made by physicians who were not formally trained in genetics (Table 1). A similar percentage (73/83, 88%) agreed that non-BCCG physicians were delivering the bulk of the management of genetic conditions. There was less consensus about whether general internists and/or medicine subspecialists had the requisite knowledge and skills to make accurate genetic diagnoses (strongly agree 7%, somewhat agree 41%, neutral 14%, somewhat disagree 30%, and strongly disagree 7%) or to provide genetic counseling to adults with genetic conditions (strongly agree 4%, somewhat agree 27%, neutral 17%, somewhat disagree 35%, and strongly disagree 18%). Despite ambivalence about the abilities of nongeneticists to provide genetic services, the majority of chairpersons disagreed with the notion that genetic diagnoses should be made by BCCG rather than generalists and other medicine subspecialists (60% “strongly/somewhat disagree”). No clear consensus was present with the statement: “in the near future…the majority of diagnoses of genetic conditions will be made by individuals with FORMAL training in Clinical Genetics.” Finally, 77% (64/83) agreed that DOMs should include faculty with formal clinical genetics training and 32% (27/85) expressed a plan to hire a BCCG in the next two years.
DISCUSSION
The ultimate role of genetics in adult clinical medicine still remains unclear. From this survey, only a minority of DOMs employed faculty geneticists and, whereas 77% of DOMs offered formal genetics didactics, education about genetics was provided by BCCGs in less than half of cases. Only 12% of genetics didactics were taught by BCCG who were faculty within the DOM. Although not directly addressed by this survey, the effectiveness enjoining nongeneticists or BCCG from other departments (presumably most commonly Pediatric-trained geneticists) to train internal medicine residents about adult-onset genetics may be imperfect.
One potential limitation of this survey is that no allowances were made for BCCG who have appointments in more than one department (e.g., medicine and pediatrics). It is possible that some of the faculty identified by chairpersons as being BCCG in their DOM have dual appointments, but are in fact primarily appointed in other departments (e.g., pediatrics). The extent of these relationships between DOMs and non-DOM BCCG was not thoroughly explored in this survey and it is possible that DOMs with well-established relationships with pediatric-based clinical genetics programs, for instance, may have their current clinical and educational needs with respect to genetics fulfilled. It is also unknown what percentage of DOMs have clinics that focus primarily on adult genetic disorders, and what proportion of these are dedicated to disorders other than cancer genetics. The absence of an accepted model for what comprises an “adult genetics clinic” complicates efforts to obtain such data. Obviously these might be difficult entities to define as a cystic fibrosis clinic, for instance, deals with a genetic disease that affects adults, but may be predominantly dedicated to disease management and less focused on genetic testing and counseling. More published information describing different prototypes of “adult genetics clinics” is needed to help guide DOMs as they contemplate developing such efforts. This need extends beyond general genetics clinics, but must also include methods of integrating clinical genetics practice into adult subspecialty clinics.
Further exploration into the content and delivery of genetic educational material relevant to the training of internists is also warranted. As the relevance of clinical genetics to the practice of adult clinical medicine continues to broaden the onus will be at least partially placed upon DOM to prepare future internists to integrate genetics into the care of the adult population. This is especially relevant as the American Boards of Internal Medicine (ABIM) and Medical Genetics (ABMG) have approved the development of dual training programs in internal medicine and clinical genetics. The first graduates from these programs are not expected for several years, yet their progress and success is expected to play a significant role in the further development of clinical genetics in the arena of adult medical care.
The American College of Graduate Medical Education’s (ACGME) guidelines for training in internal medicine do not include specific provisions for training in medical genetics.7 The ABIM lists sixteen primary content areas and eleven cross-content areas as being covered in the certification exam for internal medicine.7 Although it is probable that some genetic-related questions may be covered under these topic headings (3% miscellaneous for instance), it appears that the genetic medicine content does not figure prominently in the makeup of this examination. The creation of combined residency programs in internal medicine and clinical genetics may increase the genetic content required for training and certification for internists. One hope is that residents training in these dual environments may function also as educators of their internal medicine and clinical genetics colleagues, further helping to connect the two fields. For those programs lacking the resources or desire to develop dual training programs in these disciplines, the integration of clinical genetics curricula into residency training may be challenging.
Most (77%; P < 0.001) chairpersons in this survey supported the notion that DOM should include BCCG faculty physicians even though there was a tendency for chairpersons to disagree that BCCGs should preferentially make “the majority of diagnoses of genetic conditions” (48% p = 0.182). Admitting an “interest” in integrating clinical geneticists into DOMs on a survey may not accurately reflect how strong of a commitment exists to actually dedicating department resources to supporting clinical geneticists. In fact, only 32% of chairpersons had plans to hire BCCG in the next two years, perhaps reflecting ambivalence about the future of this field or the limited number of physicians with backgrounds in internal medicine and genetics. It would likely be worthwhile to explore why some DOMs appear to be reluctant to embrace clinical genetics as an essential or even important aspect of clinical adult medicine. Indeed, some scientists are less enthusiastic about the robustness of current predictions, and suggest that the introduction of practical and user-friendly genomic medicine remains very theoretical.8 If, however, the views of Collins and McKusick (both trained as internists, incidentally) are to be embraced, then the road ahead for internists may be difficult to navigate without more expertise in this area. Will genetic services for adults continue to be delivered by predominantly pediatrics-trained BCCG? Research is needed to evaluate the effectiveness of pediatric-trained BCCG to engage the internal medicine community. Given that currently, only a meager 9% (84/903) of BCCG are certified also in internal medicine (Personal communication, Sharon Robinson, ABMG Administrator: 8/21/01), current resources in terms of BCCG geneticists with adult-medicine training are likely to be insufficient for meeting rising demands in adult genetic medicine. The time may now be ripe for discussion among the academic leaders of internal medicine and the ABIM to explore whether their specialty is properly prepared to “evolve”.
References
GeneTests. 2003, http://www.genetests.org.
Collins FS, McKusick VA . Implications of the Human Genome Project for medical science. JAMA 2001; 285: 540–544.
Escher M, Sappino AP . Primary care physicians’ knowledge and attitudes towards genetic testing for breast-ovarian cancer predisposition. Ann Oncol 2000; 11: 1131–1135.
Hayflick SJ, Eiff MP, Carpenter L, Steinberger J . Primary care physicians’ utilization and perceptions of genetics services. Genet Med 1998; 1: 13–21.
Hofman KJ, Tambor ES, Chase GA, Geller G, Faden RR, Holtzman NA . Physicians’ knowledge of genetics and genetic tests. Acad Med 1998; 68: 625–632.
2000-2001 Directory of American Medical Education. In. M M, ed. Washington, DC: Association of American Medical Colleges, 2000.
Education ACoGM. 2003, http://www.acgme.org.
Holtzman NA, Marteau TM . Will genetics revolutionize medicine? N Engl J Med 2000; 343: 141–144.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Taylor, M. A survey of chairpersons of departments of medicine about the current and future roles of clinical genetics in internal medicine. Genet Med 5, 328–331 (2003). https://doi.org/10.1097/00125817-200307000-00009
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1097/00125817-200307000-00009
