
Abstract
Purpose
To investigate the effect of prior intravitreal injections on intraoperative and postoperative complication rates associated with cataract surgery.
Methods
A retrospective cohort analysis reviewed 10 105 cataract surgery procedures performed by experienced surgeons at the Duke Eye Center from 1 January 2005 to 10 December 2012. A group of 197 eyes with prior intravitreal injections was compared with an equal number of matched control eyes without prior injection using the Fisher’s exact test of difference in proportions and the Wilcoxon rank-sum test of difference in means. Outcomes analyzed included baseline demographic information, preoperative clinical characteristics, prevalence of intraoperative complications, and postoperative intraocular pressure, glaucoma surgery, and glaucoma medication requirement through 1 year following cataract surgery.
Results
An increased rate of intraoperative complications was identified during cataract surgery in eyes with prior intravitreal injections compared with control eyes (3 vs 0%, P=0.030). Injection eyes required more glaucoma medications at 1 year, but no difference was identified if steroid injections were excluded. No difference in postoperative IOP or glaucoma surgery was identified. No cases of endophthalmitis were reported.
Conclusions
A history of intravitreal injections may be a risk factor for cataract surgery-related intraoperative complications. We hypothesize this may be due to unidentified iatrogenic lens trauma during intravitreal injections. Particular attention to the posterior capsule during preoperative assessment and intraoperatively is recommended in eyes undergoing cataract surgery with a prior history of intravitreal injections.
Similar content being viewed by others

Introduction
The development of anti-vascular endothelial growth factor (VEGF) agents administered through intravitreal injections (IVTs) has transformed clinical management of retinal diseases. IVTs and cataract surgery are the most common ophthalmologic procedures performed in the United States Medicare population.1 Although complications related to IVTs continue to be extensively investigated, analyses have generally focused on systemic complications, particularly thromboembolic events, and intraocular complications, including endophthalmitis, inflammation, retinal detachments, and elevated intraocular pressure (IOP).2, 3 To the authors’ knowledge, the impact of IVTs on subsequent cataract surgery has not been extensively investigated.
There are a priori considerations that would predict an altered safety profile in patients undergoing cataract extraction. The proximity of the intravitreal needle path to the lens may confer an increased risk of iatrogenic lenticular trauma and resulting posterior capsular rupture during cataract surgery. Anecdotal reports by cataract surgeons of IVT-related lenticular trauma are corroborated by a few published individual reports of both subclinical lenticular damage as well as cataract-inducing needle penetration into the lens.4, 5, 6, 7 A single case of ‘lens trauma’ was reported in the combined phase 3 data of the pivotal ANCHOR (Anti-VEGF Antibody for the Treatment of Predominantly Classic Choroidal Neovascularization in AMD) and MARINA (Minimally Classic/Occult Trial of the Anti-VEGF Antibody Ranibizumab in the Treatment of Neovascular AMD) trials following a total of 754 ranibizumab (Lucentis; Genentech, Inc; San Francisco, CA, USA) injections for treatment of age-related macular degeneration (AMD).8, 9 In addition, repeated IVTs may be associated with sustained elevation of the IOP, which may secondarily increase rates of open-angle glaucoma.10, 11, 12 At the same time, cataract extraction may result in a decrease in IOP13 and offset this elevation. Finally, the use of post-injection topical antibiotics has been associated with a secondary increase in antibiotic-resistant ocular flora that may result in an increase in the rate of post-cataract endophthalmitis in eyes with a history of IVTs.14, 15
We recently reported an analysis of Medicare claims data demonstrating an increase in subsequent retained lens fragment removal and endophthalmitis following cataract surgery in an elderly population with a history of prior IVTs.16 Given the limitations inherent in analysis of billing claims designed for reimbursement purposes and no documentation of clinically relevant findings, we analyzed clinical records from 2005 to 2012 at the Duke Eye Center to determine the rate of intraoperative complications, IOP and other glaucoma-related changes, and endophthalmitis associated with cataract surgery in patients with and without a history of prior IVTs. We provide evidence suggesting that IVTs may be associated with a clinically relevant increased risk of intraoperative complications during cataract surgery.
Methods
A retrospective review of clinical charts at the Duke Eye Center was performed under a Duke University institutional review board approved study that adhered to the tenets of the Declaration of Helsinki. Inclusion criteria consisted of all eyes undergoing cataract surgery from 1 January 2005 to 10 December 2012 by four experienced cataract surgeons performing >250 cataract surgeries per year;17 these eyes were identified based on query of billing records for Current Procedure Terminology-4 (CPT-4) codes 66982 and 66984. Exclusion criteria consisted of age under 18 years, a history of prior intraocular surgery or penetrating ocular trauma, and absence of baseline records. Of these eyes, query of billing records was used to identify the study group of eyes with IVT (CPT-4 67028) performed in the same eye at the Duke Eye Center prior to cataract surgery, which was confirmed through review of individual clinical records. A control group of the same number of eyes without a history of prior IVT was computer-generated with best match by surgeon and age. In this control group, eyes with a history of prior IVTs identified through chart review (eg, performed outside of the Duke Eye Center) were excluded.
Demographic data, including sex, age, and race, were collected from review of clinical records. Baseline clinical data included operated eye, preoperative visual acuity (VA), recorded cataract grade (nuclear sclerosis (NS), cortical spokes, and posterior subcapsular cataract (PSC)), IOP, glaucoma and/or glaucoma suspect status, axial length, pseudoexfoliation, phacodonesis, and diabetes. In addition, the number and type of IVTs (bevacizumab (Avastin; Genentech, Inc.), ranibizumab (Lucentis; Genentech, Inc.), aflibercept (Eylea; Regeneron, Inc., Tarrytown, NY, USA); and pegaptanib (Macugen; Valeant Pharmaceuticals, Inc., Montreal, CA, USA); triamcinolone acetonide (Kenalog; Bristol-Myers Squibb, Princeton, NJ, USA) or Triesence; Alcon, Fort Worth, TX, USA) performed prior to cataract surgery and the indications for injections (neovascular AMD, diabetic macular edema (DME), or other) were recorded.
The primary endpoint in this study was rate of intraoperative complication, which was determined through review of each operative report. Type of complication, if any, and type of intraocular lens (IOL) placed were recorded. Intraoperative complication was primarily defined as posterior capsular rupture and/or anterior vitrectomy and/or unplanned placement of a three-piece IOL without planned or simultaneous vitrectomy, which was included given the standard use of operative report templates that may not always reflect surgical complications. These criteria for defining complications were established prior to initiating data analysis. Secondary analysis was also subsequently performed defining complications as above but without inclusion of unplanned three-piece IOL placement. Postoperative data were collected at 1 year as available, including VA, IOP, and number of additional glaucoma medications. In addition, clinical charts through 1 year were reviewed as available for numbers of additional glaucoma surgical procedures and occurrence of endophthalmitis.
Statistical analysis was performed by a statistician (SS) to compare baseline, intraoperative, and postoperative data between the IVT and control groups using the Fisher’s exact test of difference in proportions and the Wilcoxon rank-sum test of difference in means. Visual acuities were converted from ETDRS to logMAR units for statistical analysis. A secondary analysis of the same outcomes was subsequently performed excluding patients with prior intravitreal corticosteroid injections.
Results
A total of 10 103 eyes underwent cataract surgery by 4 cataract surgeons at the Duke Eye Center from 1 January 2005 through 10 December 2012. Of these, 227 eyes had a history of IVT performed at the Duke Eye Center prior to cataract surgery. In all, 30 patients were excluded due to age under 18, a history of prior intraocular surgery or penetrating ocular trauma, or loss of baseline records. From the remaining 197 IVT eyes, a control group of 197 eyes without prior IVT was best matched by surgeon and age.
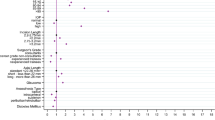
Demographic data were not different between the IVT and control groups (Table 1). Preoperatively, IVT eyes had worse VA than control eyes (mean (SD): 0.98 (0.64) logMAR vs 0.49 (0.53) logMAR, P<0.001). IVT eyes also had significantly worse NS and PSC. IVT eyes had increased prevalence of diabetes, but other preoperative clinical characteristics, including glaucoma, axial length, pseudoexfoliation, and phacodonesis were not different. The mean number of prior IVTs in the IVT group was 5.57 (range 1–49), with the majority being bevacizumab injections for neovascular AMD followed by DME.
The rate of intraoperative complications, defined a priori as posterior capsular rupture and/or anterior vitrectomy and/or unplanned three-piece IOL, was significantly higher in the IVT group (3%, n=6) vs control (0%; P=0.030; Table 2). In one of the eyes in the complications group, no report of posterior capsular rupture or anterior vitrectomy was found, but an MA60 three-piece IOL (Alcon, Fort Worth, TX, USA) was placed without simultaneous or planned vitrectomy. Given practice patterns at our institution, we correlate unplanned three-piece IOL placement with an intraoperative complication that was inadvertently not reported in the standard operative report template. Secondary analysis with exclusion of this eye resulted in a rate of complication in IVT vs control eyes that approached significance (2.5 vs 0%, P=0.061). Mean (SD) numbers of injections prior to cataract surgery were 11.83 (15.20) in eyes with complications (range 2–41) and 5.37 (6.52) in eyes without complications (range 1–49), but this difference was not statistically significant (P=0.193). Of the eyes with complications, those receiving IVTs for NVAMD (n=4) were on a fixed regimen of injections every 4–8 weeks that was not altered or discontinued for cataract surgery, which ranged from 9–28 days following the most recent IVT. Of the two eyes receiving IVTs for DME, IVTs were not performed around the time of surgery, which occurred 9 and 33 months following the most recent IVT.
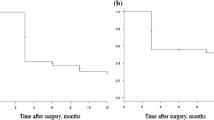
Preoperative VA was significantly lower in IVT than control eyes and remained lower at 1 year postoperatively. However, both groups achieved similar improvements in VA acuity at 1 year following cataract surgery. Although IOP was not different preoperatively or at 1 year, IVT vs control eyes required more additional glaucoma medications at 1 year following cataract surgery (mean (SD): 0.13 (0.48) vs 0.01 (0.11) additional medications, P=0.021). There was no difference in the need for additional glaucoma surgery within 1 year following cataract surgery. No cases of endophthalmitis were identified in either group.
Subsequent analysis with exclusion of eyes with prior corticosteroid injections also demonstrated a significantly higher intraoperative complication rate of 4% (n=5 of 122) with injections vs 0% (n=0 of 197) in controls (P=0.008; Table 3). This difference remained significant with exclusion of the eye with an unplanned three-piece IOL (3 vs 0%; P=0.021). Neither the improvements in VA following cataract surgery were not different between IVT and control groups, nor was the IOP preoperatively and at 1 year. With exclusion of corticosteroids, the previously noted increase in glaucoma medication burden was not found to be significant (mean (SD): 0.06 (0.30) additional medications vs 0.01 (0.11), P=0.159). Similarly, the need for glaucoma surgery remained not different.
Review of the clinical characteristics of the six eyes with intraoperative complications was performed (Table 4). Five eyes were from female patients, and five eyes were from white patients. Three eyes had PSC, and in each of these eyes, a posterior capsular defect was noted during the cataract surgeon’s preoperative evaluation. No eye had axial length longer than 26 mm or phacodonesis; 1 eye had pseudoexfoliation and 2 eyes were from patients with diabetes. Number of prior IVTs ranged from 2 to 41, primarily for neovascular AMD with bevacizumab comprising the majority of injections. One eye was left aphakic and required subsequent vitrectomy for removal of retained lens fragments. An anterior chamber IOL was placed in 1 eye, and a 3-piece IOL was placed in the other 4 eyes. Year of cataract surgery ranged from 2007 to 2012. None of the eyes had lens trauma documented at the time of IVT in the retina physician records.
Discussion
Despite anecdotal and individual reports of lenticular trauma following IVTs,4, 5 previous analyses of patients undergoing cataract surgery following injections did not identify safety concerns.18, 19, 20 Each of these prior analyses was limited to a small cohort of 30 eyes or fewer undergoing cataract surgery with prior IVT.18, 19, 20 In this series, we reviewed a cohort of 197 eyes with prior injections along with an equal number of matched control eyes without prior injections. Only eyes with prior injections performed at the Duke Eye Center were included to ensure complete retrospective analysis. To the authors’ knowledge, this series represents the largest reported analysis of eyes undergoing cataract surgery with prior IVT. Our study included eyes as early as 1 January 2005 to maximize inclusion of eyes with prior IVTs, which significantly increased following introduction of pegaptanib in 200421 and particularly bevacizumab in 2005.22, 23 Our analysis was limited to cataract surgery performed by four experienced cataract surgeons at the Duke Eye Center, excluding less-experienced surgeons to attempt to minimize variability in outcomes related to variable surgeon technique.
We identify an increase in the rate of intraoperative complications during cataract surgery in eyes with prior IVTs. In the six eyes with complications, preoperative evaluation by the cataract surgeon identified PSC in three IVT eyes; only one of these PSC eyes had been treated with intravitreal corticosteroids, and none were in patients with diabetes or DME. In all three of these eyes, a pre-existing posterior capsular defect was identified during preoperative evaluation. In the remaining three eyes, presence of PSC or a posterior capsular defect was not reported, but in this retrospective analysis, their presence cannot be excluded. We suggest that needle-induced trauma to the posterior capsule during injection resulted in violation of the posterior capsule and secondary PSC formation. Consistent with this hypothesis, eyes with complications received approximately twice as many IVTs compared with eyes without complications, although this difference did not reach statistical significance. Effects from differences in baseline characteristics, including more advanced cataract status or higher prevalence of diabetes mellitus, or effects from the underlying therapeutic agents themselves, are less likely but cannot be excluded. Of the six eyes, one eye was left aphakic and one with an anterior chamber IOL, with both resulting in deterioration of final vision compared to preoperatively. The visual impact of injection-related intraoperative complications needs to be further evaluated. The majority of IVT eyes with complications were female and treated with bevacizumab for neovascular AMD, likely consistent with the typical patient population receiving injections rather than an implication of these factors in inducing surgical complications.
Our analysis of glaucoma-related outcomes in all patients, including those treated with intravitreal corticosteroids, identified an increased glaucoma medication burden in IVT eyes following cataract surgery compared with controls. However, following exclusion of intravitreal corticosteroid injections, where the association with elevated IOP is well-known, analysis did not find any significant difference between groups in IOP, glaucoma medication requirement, or need for additional glaucoma surgery. No difference in endophthalmitis was found, but no cases were reported.
We acknowledge several important study limitations. The study is limited by its retrospective design. We were not able to match controls according to lens status, which were graded subjectively and with varying description, and detail by different providers. Similarly, pupil size, presence/absence of corneal opacities, preoperative identification of phacodonesis, pseudoexfoliation, or other risk factors, and identification of posterior lens capsule defects were variably recorded. We cannot exclude the possibility of significant effects caused by any of these factors. Complications may not have been disclosed in the operative report due to medico-legal considerations or due to the prevalent use of standard operative report templates that may inadvertently not have been adjusted. To address this potential limitation, our analysis included in the primary definition of complication unplanned three-piece IOL placement, which is typically not performed at our institution in the absence of simultaneous or planned vitrectomy or intraoperative complication.
In addition, although a large series, this study was not adequately powered to identify changes in rare outcomes. No cases of endophthalmitis were identified, and no difference in IOP or glaucoma-related management between IVT and control eyes was found after excluding prior corticosteroid injection. Further investigation with larger numbers is likely required to detect any differences, if present. Importantly, no intraoperative complications were reported in the control group, in contrast to published rates of posterior capsular rupture and anterior vitrectomy ranging from 1.6% to as high as 9%.24 The low rate in this report may be attributable to improved surgical technology and restriction of our analysis to surgeries performed by experienced surgeons only performing at least 250 cataract surgeries per year. A previous analysis of cataract surgery-related outcomes by surgeon volume demonstrated an adverse event rate of 0.4% (1 in 250) for surgeons performing 251–500 cataract surgeries per year and 0.2% (1 in 500) for surgeons performing 501–1000 cataract surgeries per year.17 Increased numbers with a prospective design will be important to accurately evaluate these complications, their true incidences, and their impact of visual and other outcomes.
Our series was limited to eyes managed at a single tertiary care academic center. It is possible that physicians-in-training (residents and/or fellows) may have been involved in the care of these patients. Specifically, needle-induced lenticular trauma may be a result of variability in technique or skill of IVTs associated with physicians at various levels of experience. Similarly, variability in surgeon participation during cataract surgery may have contributed to differences in complication rates. At our institution, the specific contributions to clinical care by physicians-in-training are typically not distinguished in the documentation, and prospective analyses would be required to fully validate these findings. In addition, it is possible that these outcomes were a result of the learning curve for IVTs as their use became prevalent in 2005. In this series, cataract surgery with complications associated with IVTs were performed from 2007 up through 2012, with 4 of the 6 cases in 2012, suggesting that these complications are not a result of early experiences by retina providers with injections. Instead, it is possible that frequency of inadvertent lenticular trauma has increased with time as precision with IVT technique, as with use of calipers to mark the appropriate incision site posterior to the limbus, has become less consistent as providers have developed greater presumed comfort with and clinical demand for injections.
We have recently published a separate, paired analysis of the 5% Medicare claims data investigating the impact of prior IVTs on cataract surgery-related outcomes in the elderly.16 This Medicare claims analysis suggests that prior IVT is associated with a 126% increased risk of retained lens fragment removal as well as increased postoperative endophthalmitis. Such claim-based analysis has inherent limitations, as such data are designed for billing and no clinical information. However, this claims-based approach provides sufficiently large numbers to detect changes in these rare outcomes and is complementary to the clinical record-based analysis, with its own inherent limitations, as reported herein. In the Medicare analysis, a rate of 0.43% retained lens fragment removal was identified in beneficiaries with a prior history of IVTs, consistent with the 0.51% rate in this clinical study. Together, these studies provide compelling evidence that prior IVTs may be a risk factor for subsequent posterior capsular rupture during cataract extraction.
Conclusions
We hypothesize that inadvertent interaction between the injection needle and the crystalline lens during IVTs may result in increased rate of subsequent cataract surgery-related complications. None of the eyes had documented lens trauma in the retina physician records, and we believe that this inadvertent interaction generally occurs unknowingly. The indications and need for IVTs continue to quickly grow, and the burden of treatment is beginning to extend beyond the retina specialist. We urge an intimate understanding by the injecting practitioner of intraocular anatomic relationships, particularly of the posterior segment and the lens, whose relationships are displaced as the eye is intentionally torqued during the injection procedure. Similarly, cataract surgeons should include a careful preoperative assessment of the posterior capsule in patients with a history of prior IVTs, particularly in the presence of any PSC, and understand precautions and surgical procedure modifications that may minimize complications associated with pre-existing posterior capsule defects.6 Increased awareness of this potential complication by injecting practitioners may increase prevention, and we urge cataract surgeons to carefully examine the posterior capsule prior to cataract surgery in these patients.

References
Centers for Medicare and Medicaid Services Part B National Summary Data File. Available at http://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/NonIdentifiableDataFiles/PartBNationalSummaryDataFile.html. accessed on 29 January 2014.
Falavarjani KG, Nguyen QD . Adverse events and complications associated with intravitreal injection of anti-VEGF agents: a review of literature. Eye 2013; 27 (7): 787–794.
Day S, Acquah K, Mruthyunjaya P, Grossman DS, Lee PP, Sloan FA . Ocular complications after anti-vascular endothelial growth factor therapy in medicare patients with age-related macular degeneration. Am J Ophthalmol 2011; 152 (2): 266–272.
Jonas JB, Spandau UH, Schlichtenbrede F . Short-term complications of intravitreal injections of triamcinolone and bevacizumab. Eye 2008; 22 (4): 590–591.
Khalifa YM, Pantanelli SM . Quiescent posterior capsule trauma after intravitreal injection: implications for the cataract surgeon. J Cataract Refract Surg 2011; 37 (7): 1364.
Saeed MU, Prasad S . Management of cataract caused by inadvertent capsule penetration during intravitreal injection of ranibizumab. J Cataract Refract Surg 2009; 35 (11): 1857–1859.
Coca-Robinot J, Casco-Silva B, Armada-Maresca F, Garcia-Martinez J . Accidental injections of dexamethasone intravitreal implant (Ozurdex) into the crystalline lens. Eur J Ophthalmol 2014; 24 (4): 633–636.
Rosenfeld PJ, Brown DM, Heier JS, Boyer DS, Kaiser PK, Chung CY et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 2006; 355 (14): 1419–1431.
Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T et al. Ranibizumab vs verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Ophthalmology 2009; 116 (1): 57–65 e55.
Hoang QV, Mendonca LS, Della Torre KE, Jung JJ, Tsuang AJ, Freund KB . Effect on intraocular pressure in patients receiving unilateral intravitreal anti-vascular endothelial growth factor injections. Ophthalmology 2012; 119 (2): 321–326.
Bakri SJ, Moshfeghi DM, Francom S, Rundle AC, Reshef DS, Lee PP et al. Intraocular pressure in eyes receiving monthly ranibizumab in 2 pivotal age-related macular degeneration clinical trials. Ophthalmology 2014; 121 (5): 1102–1108.
SooHoo JR, Seibold LK, Kahook MY . The link between intravitreal antivascular endothelial growth factor injections and glaucoma. Curr Opin Ophthalmol 2014; 25 (2): 127–133.
Slabaugh MA, Chen PP . The effect of cataract extraction on intraocular pressure. Curr Opin Ophthalmol 2014; 25 (2): 122–126.
Kim SJ, Toma HS . Ophthalmic antibiotics and antimicrobial resistance a randomized, controlled study of patients undergoing intravitreal injections. Ophthalmology 2011; 118 (7): 1358–1363.
Storey P, Dollin M, Pitcher J, Reddy S, Vojtko J, Vander J et al. The role of topical antibiotic prophylaxis to prevent endophthalmitis after intravitreal injection. Ophthalmology 2014; 121 (1): 283–289.
Hahn P, Yashkin AP, Sloan FA . Effect of prior anti-VEGF injections on the risk of retained lens fragments and endophthalmitis after cataract surgery in the elderly. Ophthalmology 2015; 123 (2): 309–315.
Bell CM, Hatch WV, Cernat G, Urbach DR . Surgeon volumes and selected patient outcomes in cataract surgery: a population-based analysis. Ophthalmology 2007; 114 (3): 405–410.
Jonas JB, Kreissig I, Degenring RF . Cataract surgery after intravitreal injection of triamcinolone acetonide. Eye 2004; 18 (4): 361–364.
Rosenfeld PJ, Shapiro H, Ehrlich JS, Wong P, Marina, Groups AS . Cataract surgery in ranibizumab-treated patients with neovascular age-related macular degeneration from the phase 3 ANCHOR and MARINA trials. Am J Ophthalmol 2011; 152 (5): 793–798.
Tabandeh H, Chaudhry NA, Boyer DS, Kon-Jara VA, Flynn HW Jr . Outcomes of cataract surgery in patients with neovascular age-related macular degeneration in the era of anti-vascular endothelial growth factor therapy. J Cataract Refract Surg 2012; 38 (4): 677–682.
Gragoudas ES, Adamis AP, Cunningham ET Jr., Feinsod M, Guyer DR, Group VISiONCT. Pegaptanib for neovascular age-related macular degeneration. N Engl J Med 2004; 351 (27): 2805–2816.
Rosenfeld PJ, Moshfeghi AA, Puliafito CA . Optical coherence tomography findings after an intravitreal injection of bevacizumab (avastin) for neovascular age-related macular degeneration. Ophthalmic Surg Lasers Imaging 2005; 36 (4): 331–335.
Stein JD, Hanrahan BW, Comer GM, Sloan FA . Diffusion of technologies for the care of older adults with exudative age-related macular degeneration. Am J Ophthalmol 2013; 155 (4): 688–696.
American Academy of Ophthalmology Cataract and Anterior Segment Panel Preferred Practice Pattern Guidelines. Cataract in the Adult Eye. American Academy of Ophthalmology: San Francisco, CA, USA, 2011 Available at http://www.aao.org/ppp.
Acknowledgements
Paul Hahn reports a consulting agreement unrelated to the submitted work with Second Sight Medical Products and Bausch and Lomb. Kim Jiramongkolchai: none. Sandra Stinnett: none. Melissa Daluvoy: none. Terry Kim reports consulting agreements unrelated to the submitted work with Alcon, Allergan, Bausch & Lomb, Kala Pharmaceuticals, NovaBay Pharmaceuticals, Ocular Systems, Inc., Ocular Therapeutix, Omerus, Powervision, Presbyopia Therapies, Shire, and TearScience.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Hahn, P., Jiramongkolchai, K., Stinnett, S. et al. Rate of intraoperative complications during cataract surgery following intravitreal injections. Eye 30, 1101–1109 (2016). https://doi.org/10.1038/eye.2016.109
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2016.109
