
Abstract
Purpose
To describe involution patterns following monotherapy with intravitreal bevacizumab injection (IVB) for type 1 retinopathy of prematurity (ROP) in zone I or zone II posterior.
Methods
A retrospective chart review of infants treated with IVB from January 2010–April 2014. Infants with minimum of 82 weeks postmenstrual age at last follow-up were included. Primary outcome was timing of involution of type 1 ROP for the first 12 weeks post treatment. Secondary outcomes were development of any recurrence and structural outcome at last follow-up. Retinal examination records, fundus, and flourescein angiography images were reviewed.
Results
Twenty-eight eyes were included. Average follow-up post treatment was 33.9±9.7 months (range 21.4–61.9). Cumulative frequency of regression of plus disease was seen in 73.3, 86.7, and 100% of eyes by days 3, 5, and 8, respectively. Regression of both stage 3 and plus disease was observed in 29, 82, 88, and 100% by weeks 1, 2, 3, and 4, respectively. Within the first 3 months, 17/28 eyes developed recurrence to stage 1 or 2 after regression. None developed recurrence of plus disease. By the end of 3 months 18% of eyes vascularized into zone III. At a mean of 24±17.3 months, 39% of eyes were not vascularized into zone III as seen on flourescein angiography with scleral indentation.
Conclusion
Our experience suggests regression of plus disease and stage 3 are expected within the first 4 weeks after bevacizumab treatment. Recurrence may occur despite initial regression and requires careful follow-up.
Similar content being viewed by others

Introduction
Anti-vascular endothelial growth factors are increasingly used in the management of retinopathy of prematurity (ROP).1 Off label use of bevacizumab has been shown to be an effective treatment for type 1 ROP.2, 3, 4, 5 Bevacizumab Eliminates the Angiogenic Threat of Retinopathy of Prematurity (BEAT-ROP) randomized trial reported significant treatment benefit with bevacizumab over laser for stage 3 plus ROP in zone I.2 However, reports of late recurrence and development of retinal detachment necessitate frequent follow-up for an extended time period post treatment.6, 7 Information on involution patterns following this treatment modality is not available. Involution patterns for non-threshold ROP were studied previously.8, 9, 10 In addition, the process of involution of threshold disease after treatment with diode laser photocoagulation was described.11 There is scarcity of evidence to guide clinicians on forms of recurrence, frequency and length of follow-up, and involution patterns that may lead to unfavorable structural outcomes following treatment with intravitreal bevacizumab (IVB). The purpose of this study is to describe timing of regression following monotherapy with IVB for type 1 ROP in zone I or zone II posterior and its relationship to structural outcomes.
Materials and methods
We performed a retrospective chart review of all infants with ROP treated at our institution with intravitreal bevacizumab injection (Avastin; Genentech Inc, San Francisco, CA, USA) from January 2010 to April 2014. The study was approved by the hospital’s research ethics board. At this institution, we now offer treatment with IVB as an alternative treatment to laser for type 1 ROP in zone I or zone II posterior. Since the use of IVB for anterior disease has not been subjected to randomized controlled trials, this treatment was only offered for sick infants that would not tolerate laser treatment under general anesthesia. These infants were not included in this study. An informed consent was obtained for each treated infant as described by our group previously.12, 13 Bevacizumab 0.625 mg/0.025 ml was injected into the vitreous cavity with a 30-gauge needle at 1.0 mm posterior to the corneoscleral junction. All injections were performed in the neonatal intensive care unit under topical anesthesia. All infants received a single injection of bevacizumab.
To capture theoretical recurrences and the latest reported recurrence of treatable ROP in the literature, a minimum of 82 weeks post-menstrual age (PMA) at last follow-up was required for inclusion in this study.6, 7, 14 Demographic data on gestational age, birth weight and PMA at time of treatment and at last follow-up were collected.
The primary outcome of the study was time to involution of type 1 ROP in the first 3 months post treatment. Secondary outcomes were development of any recurrence and structural outcome at last follow-up. Structural outcome was defined as in the Early Treatment for Retinopathy of Prematurity.15 Results of fundus examination for each visit were collected. Consensus by the two treating ophthalmologists (NT, KM) was sought for retinal examination findings including stage, zone and the presence or absence of plus disease as stated in the ROP examination record, fundus images, and flourescein angiography (FFA) (RetCam Clarity Medical Systems, Pleasanton, California). Follow-up was performed at day one post injection, then once more during the first week as per clinical need, then weekly until resolution of neovascularization. Longer term follow-up was according to response based on the follow-up screening guidelines.16 Beyond 45 weeks of PMA follow-up was individually tailored based on extent of retinal vascularization. Involution of ROP in this study was defined as regression of disease severity by at least one stage and absence of plus disease.
SAS for Windows software version 9.4, (SAS Institute, Cary, NC, USA) was used for statistical analysis. PROC MIXED with RANDOM and REPEATED statement was used for the correlation calculations between the two eyes in bilateral treated cases. Interclass correlation (ICC) was estimated using an unconditional random effect model. Findings on time to regression were described in frequency tables and cumulative frequency curves.
Results
A total of 26 infants were treated with IVB. Three were excluded because they had not reached follow-up of 82 weeks of PMA. Four had treatment for disease in anterior zone II and therefore were excluded. Two infants were excluded because we did not have complete data on each visit post treatment. Twenty eight eyes of 17 patients fulfilled the inclusion criteria and were analyzed for involution of ROP. Baseline characteristics of included infants are shown in Table 1.
ROP was diagnosed in zone I in 10 eyes and in zone II posterior in 18 eyes. All eyes had stage 3 plus ROP, except for three in zone I that had stage 3 with preplus disease.
High correlation was found between the two eyes with an ICC of 0.9 (95% CI: 0.85, 0.99). Because of high correlation, we included the eye that took longer to regress in the time to involution analysis. Cumulatively, regression by at least one stage and absence of plus disease was observed in 29%, 82%, 88%, and 100% of eyes by weeks 1, 2, 3, and 4 post treatment, respectively. Mean number of days to regression was 11±5.8 (median 8, range 3–23). Regression of plus disease was observed in 73.3%, 86.7%, and 100% of eyes by days 3, 5, and 8 post treatment, respectively. The mean number of days to regression of plus disease was 3.0±2.0 (median 2, range 1–8). Figure 1 shows the cumulative frequency curves for involution by more than 1 stage and by plus disease.

Cumulative frequency curves. Involution of retinopathy of prematurity by at least one stage and resolution of plus disease over time following monotherapy with intravitreal bevacizumab injection.
Twenty out of 28 eyes (71%) regressed to no ROP (Figure 2), while 29% regressed to stage 1 or 2. 17/28 eyes (61%) developed recurrence of stage 1 or 2 after regression. None developed recurrence of plus disease. At 3 months post-treatment, 32%, 61%, and 7% of the eyes had no ROP, stage 1, and stage 2, respectively. Five eyes (18%) had vascularized into zone III whereas the majority (82%) remained in zone II. No eye with zone I ROP before treatment had vascularized into zone III.

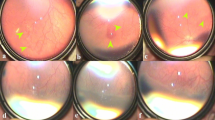
Regression of Zone 1, stage 3 retinopathy of prematurity: (a) pretreatment color fundus images and flourescein angiography showing new vessels, (b) color fundus image of the same eye 17 days post intravitreal injection with bevacizumab showing regression to no disease.
At a mean final follow-up of 33.9±9.7 months (range 21.4–61.9) all recurrences of stage 1 or 2 had regressed, none of the eyes required retreatment or had unfavorable structural outcome. 15 out of 17 infants (25 eyes) had at least 1 examination under anesthesia (EUA) (range 1–4) with indented peripheral retinal exam and FFA study over the course of follow-up. These examinations were coordinated with other surgical procedures that infants were booked for (n=9) or performed specifically for the eye examination (n=6). Additional 12 eyes (43%) were documented to have vascularized into zone III (total of 61%) as seen on flourescein angiography with scleral indentation performed at a mean of 24±17.3 months (range of 8–55) post treatment (Figure 3). Of the four infants (8 eyes) who did not fully vascularize, all had reached anterior zone II on indented examination and FFA and had no unfavorable structural outcomes at 2-3.1 years post injection. The two infants (3 eyes) who did not have an EUA, had vascularized into anterior zone II at last indented scleral exam 4 and 6 months post treatment and have remained well at 2.3 and 4 years of follow-up, respectively.

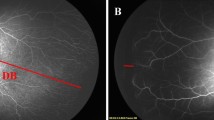
Regression of stage 3 retinopathy of prematurity in zone II posterior with plus disease: (a) pretreatment color images of the right eye, (b) flourescein angiography images 20 months post intravitreal injection of bevacizumab with vascularization into Zone III (peripheral indentation showing nasal ora).
Discussion
This paper describes patterns of involution of type 1 ROP following treatment with IVB. Regression of plus disease occurred earlier than regression of stage 3 ROP. All eyes showed involution by 4 weeks after treatment. Vascularization into zone III occurred in 18% of the eyes by the end of 3 months. Additional 43% of eyes (total 61%) vascularized into zone III by an average follow-up of 34 months post treatment. Although two thirds of the eyes developed stage 1 or 2 after involution, all eyes regressed to no ROP, and none required retreatment or developed unfavorable structural outcome at last follow-up.
The involution process following treatment with diode laser has been described.11 However, pattern of involution following treatment with IVB remains unknown. Coats et al11 reported complete involution of neovascularization in threshold ROP in 43 and 73% of the eyes at 2 and 4 weeks following treatment with laser. Compared with these findings, more eyes showed earlier involution of neovascularization in our group after IVB (82 and 100% at 2 and 4 weeks) than what has been reported following treatment with diode laser. However, complete involution in the laser study was defined as ‘absence of any active neovascular tissues and absence of residual dilatation and/or tortousity of arterioles or venules in the posterior pole without development of retinal detachment’.11 To minimize variability in the subjective interpretation of disease severity of a retrospective study, we defined involution as regression of disease severity by at least one stage and absence of plus disease. We also wanted strict criteria of involution by having both regression of disease stage and plus disease. As well, we assessed disease stage at all-time points to better understand the continuous nature of the involution process over 3 months post treatment. We were able to show that it is not uncommon to develop recurrence of stage 1 or 2 ROP after regression. Importantly, all eyes showed regression to no ROP and none of the eyes required retreatment or developed unfavorable structural outcomes at last follow-up.
Coats et al11 reported that the majority of retinal detachments (RD) were diagnosed three weeks after laser treatment and were not observed in the immediate post-operative period. They reported a cumulative diagnosis of RD in 14% of the eyes at week 9±3. On the basis of these findings, they recommended follow-up examinations should continue for at least 10 weeks post laser treatment. Currently, there are no such established guidelines for follow-up regimen following treatment with bevacizumab. Delayed recurrence of active ROP has been reported with high risk of development of RD following treatment with IVB.2, 6, 7, 14 The BEAT-ROP study recommended careful follow-up after IVB treatment until there is no active disease. The primary outcome in the BEAT-ROP trial was recurrence of neovascularization arising from retinal vessels and requiring retreatment by 54 weeks PMA. They reported a recurrence rate of 6% at a mean of 16 weeks after treatment with IVB. RD developed in two eyes that had recurrence in zone II posterior. Their paper, however, did not address the problem of eyes that are not fully vascularized. Our paper identified that 18% of eyes were fully vascularized at 3 months and the majority required careful follow-up for peripheral vascularization. Hu et al reported 17 eyes with recurrence of active disease following initial treatment with bevacizumab. Five cases progressed to develop RD. Mean time between initial treatment and recurrence requiring treatment was 14.4 weeks with a range of 4–35 weeks. Recurrence was defined as arrest of anterior progression of vascularization with the presence of a new demarcation line, ridge or extraretinal fibrovascular proliferation (EFP) or leakage on flourescein angiography with or without plus disease.6 Their definition of recurrence includes a wide range of disease severity, some of which may not meet retreatment criteria. Indeed their retreatment was not standardized but mainly performed if plus disease was present with or without EFP or EFP present with or without plus disease. Whilst presence of EFP is a worrisome sign it is still not clear whether this should qualify for retreatment without simultaneous recurrence of plus disease or at least evidence of focal traction on the retina. In this cohort, recurrence of disease did not go beyond stage 2 and there were no unfavorable structural outcomes with up to 5.0 years of follow-up. The small sample size in the current study may be one reason why we did not observe recurrence to more severe stages.
Wu et al17 reported retreating 9% of the eyes because of no response or worsening of disease at a mean of 6±3.4 weeks after initial treatment with IVB. Two percent of the eyes in their study developed RD. In our cohort of infants, we did not observe any recurrence of neovascularization within the first 3 months after treatment. In addition, after an extended follow-up, none developed neovascularization or RD. None of the above studies provided similar detail of involution or progression patterns to our paper and hence it is difficult to draw any conclusions by comparing studies. Because our results showed that recurrence can occur despite initial regression, we advise prolonged follow-up as recommended by the policy statement of the American Academy of Pediatrics until full retinal vascularization in close proximity to the ora serrata for 360°.18 This often requires scleral indentation with or without FFA under general anesthesia as babies grow older and become more difficult to examine. However, we identified that 82% of eyes were not fully vascularized at 3 months. In addition, 39% were not vascularized into zone III on angiographic evidence at a mean follow-up of 24 months. This poses a dilemma on the frequency and length of follow-up as the peripheral retina becomes progressively more difficult to visualize. At our institution if vascularization has not reached zone III, we follow children every 2 weeks until vascularization has arrested in close proximity to ora serrata, then monthly. Beyond 6 months post-treatment, we perform FFA under general anesthesia if still not vascularized into zone III to assess for peripheral extraretinal neovascularization. If the eyes are not showing signs of active disease, then we follow-up on a 3 monthly basis without scleral indentation. Parents are taught to check for obvious signs of retinal detachment through monocular testing on a weekly basis and report immediately, if poor vision is noted in between clinic visits.
Bevacizumab is also used as an adjunct to laser or surgery in the treatment of ROP.3, 5, 19 Law et al19 reported on 13 eyes of 7 infants who received initial treatment with IVB to improve visualization of retina. Definitive treatment was then performed within 72 h with either laser or surgery. In all eyes marked regression of anterior segment vascularization and improvement of pupillary dilatation was noted in the first 48 h post injection. Our study also confirms early and rapid improvement of plus disease (73% in 3 days and 100% in 8 days). However, unlike Law et al, we did not need to further treat any patients and did not experience recurrence or unfavorable structural outcomes. There may be differences in our patients’ cohort to explain this as none of our treated eyes had initial disease that prevented viewing of the fundus. Whether this represents earlier disease recognition or differences in patient characteristics is unclear. We demonstrate that although involution can be seen as early as 3 days, it took >3 weeks to observe involution in two infants. Therefore in this patient group, early retreatment may not be indicated for all cases and regression may still occur as long as disease worsening is not observed following IVB.
Our study is retrospective in nature and therefore has the limitations associated with this research method. However, we present detailed clinical information at relevant time points to describe an involution pattern following IVB injection. The relatively small number of eyes and lack of unfavorable structural outcomes does not allow us to predict which regression pattern carries a poor prognosis. By the conclusion of study period, our experience suggests that in this cohort of infants, recurrence requiring retreatment and development of unfavorable structural outcome are not common once involution occurs in the pattern described within the first 3 months post treatment.
In conclusion, involution of type 1 ROP following treatment with IVB occurred in all eyes by 1 month of treatment. Despite recurrence of stage 1 or 2 ROP within the first 3 months all regressed and no eye required retreatment or had unfavorable structural outcome at prolonged follow-up of up to 5 years.
Our cohort is the first to describe regression patterns following IVB with details on structural results. There remains a need for long-term multicenter prospective studies to fully assess favorable and unfavorable regression patterns that can predict outcome, to define standardized guidelines for follow-up, and to develop clear indications for retreatment.

References
Smith LE . Through the eyes of a child: understanding retinopathy through ROP the Friedenwald lecture. Invest Ophthalmol Vis Sci 2008; 49 (12): 5177–5182.
Mintz-Hittner HA, Kennedy KA, Chuang AZ . Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med 2011; 364 (7): 603–615.
Lalwani GA, Berrocal AM, Murray TG, Buch M, Cardone S, Hess D et al. Off-label use of intravitreal bevacizumab (Avastin) for salvage treatment in progressive threshold retinopathy of prematurity. Retina 2008; 28 (3 Suppl): S13–S18.
Mintz-Hittner HA, Kuffel RR Jr . Intravitreal injection of bevacizumab (avastin) for treatment of stage 3 retinopathy of prematurity in zone I or posterior zone II. Retina 2008; 28 (6): 831–838.
Travassos A, Teixeira S, Ferreira P, Regadas I, Travassos AS, Esperancinha FE et al. Intravitreal bevacizumab in aggressive posterior retinopathy of prematurity. Ophthalmic Surg Lasers Imaging 2007; 38 (3): 233–237.
Hu J, Blair MP, Shapiro MJ, Lichtenstein SJ, Galasso JM, Kapur R . Reactivation of retinopathy of prematurity after bevacizumab injection. Arch Ophthalmol 2012; 130 (8): 1000–1006.
Moshfeghi DM, Berrocal AM . Retinopathy of prematurity in the time of bevacizumab: incorporating the BEAT-ROP results into clinical practice. Ophthalmology 2011; 118 (7): 1227–1228.
Ni YQ, Huang X, Xue K, Yu J, Ruan L, Shan HD et al. Natural involution of acute retinopathy of prematurity not requiring treatment: factors associated with the time course of involution. Invest Ophthalmol Vis Sci 2014; 55 (5): 3165–3170.
Preslan MW, Butler J . Regression pattern in retinopathy of prematurity. J Pediatr Ophthalmol Strabismus 1994; 31 (3): 172–176.
Repka MX, Palmer EA, Tung B . Involution of retinopathy of prematurity. Cryotherapy for Retinopathy of Prematurity Cooperative Group. Arch Ophthalmol 2000; 118 (5): 645–649.
Coats DK, Miller AM, Brady McCreery KM, Holz ER, Paysse EA . Involution of threshold retinopathy of prematurity after diode laser photocoagulation. Ophthalmology 2004; 111 (10): 1894–1898.
Mireskandari K, Collins ME, Tehrani N . Intravitreal bevacizumab for retinopathy of prematurity: Considerations for informed consent. Can J Ophthalmol 2015; 50: 409–412.
Isaac M, Mireskandari K, Tehrani N . Treatment of type 1 retinopathy of prematurity with bevacizumab versus laser. J AAPOS 2015; 19 (2): 140–144.
Ittiara S, Blair MP, Shapiro MJ, Lichtenstein SJ . Exudative retinopathy and detachment: a late reactivation of retinopathy of prematurity after intravitreal bevacizumab. J AAPOS 2013; 17 (3): 323–325.
Early Treatment For Retinopathy Of Prematurity Cooperative G. Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol 2003; 121 (12): 1684–1694.
Jefferies A . Retinopathy of prematurity: Recommendations for screening. Paediatr Child Health 2010; 15 (10): 667–674.
Wu WC, Kuo HK, Yeh PT, Yang CM, Lai CC, Chen SN . An updated study of the use of bevacizumab in the treatment of patients with prethreshold retinopathy of prematurity in taiwan. Am J Ophthalmol 2013; 155 (1): 150–8 e1.
American Academy of Pediatrics, American Academy of Ophthalmology American Association for Pediatric Ophthalmology and Strabismus American Association of Certified Orthoptists. Screening examination of premature infants for retinopathy of prematurity. Pediatrics 2012; 131: 189–195.
Law JC, Recchia FM, Morrison DG, Donahue SP, Estes RL . Intravitreal bevacizumab as adjunctive treatment for retinopathy of prematurity. J AAPOS 2010; 14 (1): 6–10.
Acknowledgements
We acknowledge Brandan’s Eye Research Foundation, Concord, Ontario, Canada, for funding provided towards our department research fund. We also acknowledge XiuYan Zhao, biostatistician, clinical research services, The Hospital for Sick Children, Toronto, Ontario, Canada, for her help in data analysis. We acknowledge Leslie MacKeen, medical imaging specialist, The Hospital for Sick Children, Toronto, Ontario, Canada, for her contribution to the preparation of the images included with this manuscript.
Author contributions
Design and conduct of the study (MI, KM, NNT); collection, management, analysis, and interpretation of data (MI, KM, NNT); and preparation, review, or approval of manuscript (MI, KM, NNT).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Isaac, M., Tehrani, N. & Mireskandari, K. Involution patterns of retinopathy of prematurity after treatment with intravitreal bevacizumab: implications for follow-up. Eye 30, 333–341 (2016). https://doi.org/10.1038/eye.2015.289
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2015.289
