
Abstract
Purpose
To present four patients who developed large cystic lesions attached to the tarsal plate at the site of previously drained chalazion.
Methods
Medical records for all patients who developed cystic lesion as a complication of chalazion surgery were retrospectively reviewed for clinical and radiological findings, treatment provided, histopathological findings, and complications.
Results
Four patients (one male and three females) with a mean age of 22 years (range, 11–36 years) were enrolled in the study. A history of chalazion surgery was present in all patients at the same site of the cyst attachment to the tarsal plate. The mean interval between the presentation with the cystic lesion and the chalazion surgery was 13 weeks (range, 6–24 weeks). All patients were treated with surgical excision of the cysts, along with local triamcinolone injection. Histopathological findings of the excised cysts were consistent with chalazion. There was no evidence of recurrence or other complication observed during the follow-up visits (the minimum follow-up duration was 6 months).
Conclusions
Anterior orbital cystic formation (prolapsed chalazion) may occur as a late complication of chalazion surgery. Surgical excision along with steroid injection was effective to manage this rare complication among our patients.
Similar content being viewed by others
Introduction
Chalazion is a common chronic lipogranulomatous inflammation of the eyelid caused by plugged meibomian glands. For nonresolving chalazion, several options can be offered to the patients. These include, incision and curettage, total excision, intralesional steroid injections, and botulinum neurotoxin type A.1, 2, 3
Complications of surgical drainage of the chalazion include, eyelid margin notching, trichiasis, loss of lashes, and inadvertent globe injury.4 Incomplete chalazion drainage can result in granulation tissue prolapsing into the conjunctiva or skin. Intralesional steroid injections can be rarely complicated by eyelid depigmentation, loss of lashes, globe perforation, and vascular occlusion or anterior segment ischemia.5
Large cystic lesions extending into the anterior orbit have not yet been well described following chalazion surgical drainage. This study reports large cystic formation in four consecutive patients presented with this complication weeks after the chalazion surgery.
Materials and methods
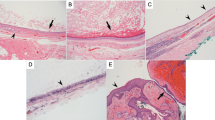
Medical records of four consecutive patients were reviewed who were presented to King Abdulaziz University Hospital, Riyadh, Saudi Arabia, with anterior orbital cystic lesions following chalazion surgery between January 2004 and August 2014. Information collected included the preoperative, intraoperative, and postoperative observations of the previously drained chalazion. Complete ophthalmologic clinical examination at presentation with anterior orbital cyst, preoperative imaging study, and ophthalmologic surgical procedures needed to manage the consequences that were recorded. Histopathological findings of the excised cyst in all included patients who were consistent with chalazion by the presence of chronic lipogranulomatous reaction, with abundant lipid-filled spaces, multinucleated giant cells, and pseudocapsule formation.
Case reports
Case 1
A 23-year-old female with right upper anterior orbital cyst appeared 6 months following chalazion surgical drainage. The cyst was attached to the tarsus at the same site of the previously drained chalazion. The patient was treated with complete surgical excision of the cysts through eyelid crease incision along with local triamcinolone injection (0.3 ml of 20 mg/ml). The patient was followed up for 9 months with no evidence of recurrence or other complication observed.
Case 2
A 38-year-old female with right upper anterior orbital cyst noticed 14 weeks following chalazion surgical drainage. The cyst was attached to the tarsus at the same site of the previously drained chalazion. Complete surgical excision of the cysts through eyelid crease incision, along with local triamcinolone injection (0.3 ml of 20 mg/ml) was done. The last follow-up was 10 months after excision of the cyst with no evidence of recurrence or other complication observed.
Case 3
An 18-year-old female with right lower anterior orbital cyst detected 2 months following chalazion surgical drainage. The cyst was attached to the tarsus at the same site of the previously drained chalazion. Orbital computer tomography showed large well-defined cyst in the anterior orbit enhancing with contrast study (Figure 1). Complete surgical excision of the cysts through subciliary incision combined with local triamcinolone injection (0.4 ml of 20 mg/ml) was done. There was no evidence of recurrence or other complication observed in the last follow-up for 7 months after surgery.

(a) An 18-year-old female presented with slowly progressive swelling in her right lower eyelid noticed 2 months after chalazion excision at the same site. (b and c) Axial and coronal orbital computer tomography scans demonstrate right anterior orbital cyst with mild contrast enhancement (white arrow).
Case 4
An 11-year-old male with left lower anterior orbital cyst noted 2 months following chalazion surgical drainage. The cyst was attached to the tarsus at the same site of the previously drained chalazion. The patient underwent complete surgical excision of the cysts through subciliary incision along with local triamcinolone injection (0.4 ml of 20 mg/ml). The patient was followed up for 6 months with no evidence of recurrence or other complication observed (Figure 2).

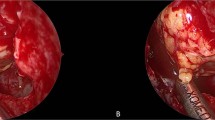
(a) An 11-year-old male presented with left lower eyelid observed by the family 6 weeks after chalazion surgery at the same site. (b) Coronal orbital computer tomography scan demonstrates a large intraorbital lesion in the anterior part of the left orbit. (c) The cyst after surgical removal through subciliary incision. (d) Six months following removal of the cyst with no evidence of recurrence.
Discussion
Granulomatous orbital inflammation is caused by different disease entities with a common histopathological feature of having epithelioid cells collections. Painless slowly growing mass is one of the presentations of this kind of inflammation.6 Anterior orbital noninfectious granulomatous inflammation is predominantly related to dermoid cyst rupture and localized orbital sarcoid.6
Here we report anterior orbital large cystic formation (prolapsed chalazion) as a late complication related to chalazion surgery. The exact pathogenesis of this complication is not well proven. We think that making an incision extending beyond the upper edge of the upper tarsus and the lower edge of the lower tarsus creates a track. Through this track, the remnant material of incompletely removed chalazion gets access into the anterior part of the orbit. Presence of the chalazion material in the anterior orbit leads to the development of the chronic lipogranulomatous reaction and pseudocapsule formation.7
Surgical excision of the cyst along with local steroid injection was a successful intervention in managing our patients. Complete excision was achieved in all patients as the presence of the pseudocapsule helped separate the mass from the rest of the orbital structures and created smooth dissection plan.

References
Goawalla A, Lee V . A prospective randomized treatment study comparing three treatment options for chalazia: triamcinolone acetonide injections, incision and curettage and treatment with hot compresses. Clin Experiment Ophthalmol 2007; 35: 706–712.
Prasad S, Gupta AK . Subconjunctival total excision in the treatment of chronic chalazia. Indian J Ophthalmol 1992; 40: 103–105.
Knezevic T, Ivekovic R, Astalos JP, Novak Laus K, Mandic Z, Matejcic A . Botulinum toxin A injection for primary and recurrent chalazia. Graefes Arch Clin Exp Ophthalmol 2009; 247: 789–794.
Smythe D, Hurwitz JJ, Tayfour F . The management of chalazion: a survey of Ontario ophthalmologists. Can J Ophthalmol 1990; 25: 252–255.
Ben Simon GJ, Rosen N, Rosner M, Spierer A . Intralesional triamcinolone acetonide injection versus incision and curettage for primary chalazia: a prospective, randomized study. Am J Ophthalmol 2011; 151: 714–718.
Satorre J, Antle CM, O'Sullivan R, White VA, Nugent RA, Rootman J . Orbital lesions with granulomatous inflammation. Can J Ophthalmol 1991; 26: 174–195.
Dithmar S, Daus W, Völcker HE . Covered rupture of periocular dermoid cysts. Clinico-histologic study. Klin Monbl Augenheilkd 1993; 203: 403–407.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Alsuhaibani, A., Al-Faky, Y. Large anterior orbital cyst as a late complication of chalazion surgical drainage. Eye 29, 585–587 (2015). https://doi.org/10.1038/eye.2014.339
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2014.339
