
Abstract
Over the past 25 years, vitreoretinal surgery has undergone considerable change in technology, techniques, and professional organisation. Many conditions that were considered untreatable in 1988 are now treated routinely by vitreoretinal surgeons. Over the same period, vitreoretinal surgery has become a separate subspecialty with its own scientific meetings and professional organisation. This article describes a noncomprehensive selection of some of the highlights of the past 25 years, including the establishment and growth of BEAVRS (British and Eire Association of Vitreoretinal Surgeons), the revolution in the management of macular holes, the development of submacular surgery, and the introduction of sutureless vitrectomy.
Similar content being viewed by others

Introduction
Twenty-five years ago in 1988 was a remarkable time in the history of vitreoretinal surgery. It was a mere 15 years since a young Robert Machemer had announced his invention of pars plana vitrectomy.1 He had been inspired by the pioneering operation of David Kasner whom he had observed removing vitreous using an open sky approach in a case of amyloidosis.2 Thinking there must be a better way, he devised a method of removing vitreous in small quantities, with the goal of extraction without transmitting traction to the retina. He set up experiments in his garage, and succeeded in removing egg white through a small incision in the shell using a rotary cutter.1 This led to the production of the VISC (Figure 1) that was effective, but required a large port, and had a tendency to wind in strands of vitreous. The approach was refined by separating the infusion and cutter functions, and using a guillotine to cut the vitreous. Thus, three-port, 20-gauge vitrectomy was introduced in 1975.3 Hence, in 1988, the technology was still relatively new, and applications for it were being avidly explored. For example, the first use of vitrectomy in the management of retinal detachment had been described only 3 years previously in 1985.4 Ophthalmic surgeons who did not undertake vitrectomy were often fearful of it, and associated it with a high risk of serious complications, a reputation that even then was not entirely justified. Vitreoretinal surgery was carried out by a number of enthusiasts, but had not evolved into a formal subspecialty. After 25 years, vitreoretinal surgery is one of the most popular subspecialties within ophthalmology, and has considerably expanded its armamentarium of treatments and indications. This article examines some of the most significant developments in vitreoretinal surgery over the past 25 years.

Dye-assisted pealing during vitrectomy surgery for a full-thickness macular hole.
BEAVRS
The concept of a British Isles Vitreoretinal Society was conceived by David MacLeod, Tony Chignell, and Peter Leaver. It was clear to them that progress in the subspeciality would be accelerated by the establishment of a dedicated society that would organise scientific meetings solely to discuss vitreoretinal topics. There were no other practical opportunities to do so at that time. The Club Jules Gonin and the Retinal Society held meetings for members and guests, and the Vail Vitrectomy meeting was (and still remains) invitation only.5 McLeod, Chignell, and Leaver (in time-honoured manner) set their fellows to work (David Wong, Charlie James, and Paul Jacobs, respectively), and this group of six are considered to be the founder members of the society. The first meeting was held at Keeble College, Oxford, in July 1986. The initial principle for the annual meeting was that everyone who attended should present, and that problems would be discussed in an uninhibited manner. The meeting was also itinerant, being both hosted and organised locally. BEAVRS (British and Eire Association of Vitreoretinal Surgeons) is well established, and is now a significant meeting on the calendar, with a professional organisation, and attracts more than 200 delegates a year.
Macular hole
Before 1988, the condition of macular hole was considered to be a curiosity and received very little interest from clinicians and researchers, achieving only six lines in Duke Elder’s textbook.6 He considered it to be a result of ‘microcystoid degeneration’, but deeper understanding had to await the attention of Don Gass.7 Gass7 was an astute observer who had a deep understanding of pathology, having spent a year studying at the Armed Forces Institute of Pathology before becoming a founder faculty member of the Bascom Palmer Eye Institute. Therefore, he brought a pathologist's eye to the condition, and came up with a rational hypothesis for the pathogenesis,7 in which vitreous traction was strongly implicated. Horizontal traction at the fovea resulted in elevation of the retina, followed by tearing of a circular operculum of retinal tissue, with associated loss of vision. In that groundbreaking paper, he suggested that a vitrectomy in stage 1 holes might reduce the risk of progression. This resulted in a large-scale trial of vitrectomy in the prevention of macular holes.8 However, before this trial could be completed, two pioneering surgeons in the United States tried vitrectomy in established holes. Peeling the posterior hyaloid and putting a bubble of gas in the eye resulted in closure of the hole, and remarkably improvement of vision in ∼50% of cases.9 Their results were met with some incredulity in the ophthalmic establishment,10 but the technique was taken up enthusiastically by others, and subsequent trials confirmed the benefit of surgery.11 In many cases, patients with closed holes experienced improvements in visual acuity to 6/9 or better. It was the excellent visual results achieved by surgery that led Gass to question his initial theory of pathogenesis, as the good vision was not compatible with the loss of foveal tissue as an operculum. Studies of removed opercula showed that many did not contain photoreceptors,12 and he later revised his theory to suggest that the hole is a horizontal separation of the fovea without loss of tissue.13 The good results from surgery also meant that the original idea of using vitrectomy for prevention proved untenable.8 The changes in techniques since then include the introduction of ILM peeling,14 the use of vital dyes15 (Figure 1), and variation in posturing regimes.16 Macular hole surgery is now an established part of the vitreoretinal surgeon’s portfolio, with closure rates above the 90% mark.
Retinal detachment
Vitrectomy was first reported for retinal detachment in 1985,4 and in many centres has grown in popularity, so that in the United Kingdom it is the preferred primary treatment for the majority of cases.17 Results seem similar to other techniques, but comparison has been difficult between published case series because of differences in case mix, and this is one of the many areas that has suffered from a lack of high standard evidence from prospective randomised clinical trials. The most significant contribution to the literature in this area over the past 25 years has been the Scleral Buckling vs Primary Vitrectomy in Rhegmatogenous Retinal Detachments Study (SPR study).18, 19 The study consisted of two trials examining phakic and aphakic/pseudophakic patients. It was a multicentre trial including 45 surgeons from 25 centres in Europe, and compared pars plana vitrectomy (see Figure 2) and gas to scleral buckling. There were 416 patients in the phakic group and 265 patients in the aphakic/pseudophakic group. The key results are summarised in Tables 1 and 2. A higher primary success rate was found for vitrectomy in the pseudophakic/aphakic group, whereas an improved visual outcome was found with scleral buckling in the phakic group.

Treatment of a retinal detachment of the type enrolled into the SPR study with vitrectomy showing a fluid–air exchange.
However, the trial has not been without criticism. For example, in the vitrectomy group, surgeons were allowed to place supplementary scleral buckles at their discretion, and this resulted in a high proportion of patients having supplementary buckles (67% in the pseudophakic/aphakic group and 51% in the phakic group). In addition, the overall primary success rate was lower than some similar nonrandomised series. One contributing factor may have been the fact that many of the participating surgeons already had a preference for one of the two procedures, and this may have been associated with a higher success rate. This factor needs to be taken into account when interpreting all surgical trials, but particularly those with single surgeons.20 The importance of this ‘surgeon factor’ is increasingly recognised and there is now a move towards conducting ‘expertise-based’ trials,21 where the patient is randomised to an operation that is then carried out by a surgeon who is tied to that operation. These sorts of trials would certainly eliminate the ‘surgeon factor’, but have significant logistic difficulties in their organisation.
There have been many other areas of debate within vitreoretinal surgery for retinal detachment over the period in question. Among surgeons who favour scleral buckling, there is a wide range of variation in the techniques used (encircling vs segmental, radial vs circumferential and so on). The controversy surrounding pneumatic retinopexy is a case in point. Randomised trials have shown that although the primary success rate is slightly less than scleral buckling, the final visual outcome is no different,22 so it would appear to make sense to attempt pneumatic retinopexy as a first procedure, particularly for patients with ‘classic’ indications.23 Despite this, the popularity of this technique in the United States has not spread to most parts of Europe. This is indicative of the fact that there are many other factors that affect management other than evidence from clinical trials.
Small gauge surgery
The 20-gauge vitrectomy had been the ‘gold standard’ since its introduction in 1975.3 It involved reflection of the conjunctiva, and the creation of perpendicular incisions into the sclera, both of which needed suturing at the end of the case. Then, in 2001, a completely new method of carrying out vitrectomy was introduced, using 25-gauge instruments and a transconjunctival approach, obviating the need for sutures.24 This technique offered faster surgery, improved postoperative comfort, and more rapid recovery, but was originally confined to routine cases such as epiretinal membrane and macular hole.25, 26 As more experience has been gained, and instruments improved, the indications have broadened to include complex vitreoretinal conditions such as rhegmatogenous retinal detachment and diabetic traction detachment.27, 28
There were several disadvantages associated with the smaller gauge, including bending of the instruments, resulting in problems in moving the eye. The smaller bore resulted in reduced fluid flow, which meant that any time saved in opening and closing the conjunctiva was potentially lost because of the extended vitrectomy time.29 In addition, blockage of the cutter with fibrous tissue and breakage of the narrow instruments had been reported.30
There were also reports of new complications. Endophthalmitis following 20-gauge vitrectomy is very rare (0.039%).31 The first reported case of endophthalmitis following 25-gauge surgery was published in 2005,32 and other reports followed.33 A large series with a higher rate was reported by David Williams (D Williams, personal communication). Another large series from the Wills Eye Hospital showed a 12-fold increased risk in patients having 25-gauge compared with 20-gauge vitrectomy.34 Similar results were reported from the Bascom Palmer Eye Institute with a rate in 25-gauge patients of (0.84% 11/1307 eyes) compared with 20-gauge vitrectomy (0.03%; 2/6375).35 Since these reports, techniques have been modified to reduce the chance of wound leakage, and more recent series have not shown a greater risk. For example, a series of 6935 patients found only one case of endophthalmitis in each group of 20-gauge and 25-gauge patients.36 The surgeons in this latter study emphasised the importance of conjunctival irrigation, ensuring sclerotomy closure and removal of peripheral vitreous as important preventative measures.
Another potential problem is hypotony that is directly related to leaking wounds. The hypotony rate after 25 gauge has been reported in as many as 25% of cases.37 The hypotony resolves usually without sequelae, although the eye is presumably at higher risk of choroidal haemorrhage while the low pressure persists, though such cases have been reported only rarely.38, 39
Most of these issues have been addressed by changes in instruments and techniques. For example, a reduction in the incidence of hypotony to 1% has been observed when a scleral tunnel is used in combination with 25-gauge cannulae.40, 41 The benefit of angled incision construction has been shown experimentally in animal models.42
In 2005, Claus Eckardt43 introduced a modified version of the original technique using existing 23-gauge instruments through shelved transconjunctival incisions. Recent experience has suggested that the technique addresses many of the issues associated with smaller gauges, and there are suggestions that it is associated with a lower rate of hypotony and endophthalmitis than 25-gauge surgery.44 This may be related to the shelved incisions that are an essential part of the technique.
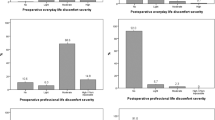
In 2007, findings from the first prospective randomised clinical trial comparing 25- and 20-gauge systems were published. The study, which reported on 60 patients, suggested that there was a significant reduction in postoperative discomfort in the 25-gauge group.29 A more recent trial from the United Kingdom had similar findings, although the absolute level of discomfort in either group was very low, with only three patients requiring any form of analgesia in the first postoperative week.45 In addition, both trials confirmed that the overall operating time was no shorter in the 25-gauge group, principally because of longer duration of the vitrectomy.
One of the potential advantages of 25-gauge surgery was that the use of cannulas might reduce trauma to the ora serrata and vitreous base, thereby reducing the incidence of entry site breaks. Unfortunately, this does not appear to be the case, with one large retrospective comparative series finding no statistically significant difference in entry site breaks between 25- and 20-gauge vitrectomy.46
The improvements in patient comfort brought about by 25- and 23-gauge systems have stimulated interest in making improvements to 20-gauge vitrectomy techniques. Various methods to avoid sutures have been described, including a valved cannula system,47 a cautery of the conjunctiva in the area of the sclerotomy,48 and other ingenious modifications.49 In spite of the early concerns, it is likely that small gauge vitrectomy is here to stay, particularly for routine vitreoretinal surgery, although it is not yet clear which of the various systems will become the future gold standard.
Submacular surgery
The past 25 years have also seen the development of a whole new domain of surgery in the subretinal space. Matt Thomas introduced a practical surgical technique for removing subretinal choroidal neovascularisation (CNV) in 1991. This minimally invasive technique was applied in two patients with CNV associated with POHS with spectacular results.50 Early success was repeated in larger series for POHS patients, but unfortunately the results were not encouraging when the technique was applied to patients with ARMD.51 Gass52 classified CNV into two types according to its relationship to the retinal pigment epithelium (RPE). Type 1 CNV lies beneath the RPE and occurs in age-related macular degeneration. Type 2 lies in front of the RPE and occurs in conditions with the common feature of a focal disturbance in Bruch’s membrane. Such conditions include punctate inner choroidopathy, multifocal choroiditis, and several other forms of uveitis. It follows that removal of type 1 membranes also removes the overlying RPE, and this was the explanation for the poor results in ARMD cases.51 The initial impressions were confirmed by a large-scale, prospective randomised clinical trial (the SST) that showed no benefit of surgery in AMRD or subretinal haemorrhage.53 However, it did show a benefit in cases with type 2 membranes presenting with poor vision (the group H trial).54 The study examined 225 patients with presumed ocular histoplasmosis syndrome and idiopathic membranes, and although we do not see POHS in the United Kingdom, it is reasonable to extrapolate the results to the common causes of type II membranes we see here (PIC, idiopathic, and MFC). Success was defined at 24 months of follow-up as vision improved, was the same or was no more than 1 line worse than at baseline. Patients with a presenting visual acuity of 20/100 or worse achieved a significant benefit from surgery, and the rate of complications was low. Surgical removal of CNV in selected cases of uveitis is effective but the increasing popularity of anti-VEGF agents and the use of photodynamic therapy mean that very few patients are now referred for surgery.
Type 2 cases represent a tiny proportion of the morbidity associated with CNV, and the real prize was discovering a treatment that worked in ARMD. In a classic example of lateral thinking, Robert Machemer conceived the idea of reestablishing contact between the foveal photoreceptors and working RPE by moving the fovea onto pigment epithelium adjacent to the defect. The technique involved creating a total retinal detachment, rotating it around the optic nerve, and re-attaching the retina using silicone oil tamponade and 360-degree laser retinopexy. He described three cases, one of which had a significant improvement in central vision, although the other two developed retinal detachment and proliferative vitreoretinopathy, and there were problems with excyclotorsion.55 The technique was taken up and modified by two pioneering surgeons, Cindy Toth and Claus Eckardt. Important modifications included making the cut in the peripheral retina as anterior as possible (to reduce the area of ischaemic retina), and carrying out extraocular muscle surgery in order to counter-rotate the globe to reduce excyclotorsion. After gathering experience with many hundreds of cases, the visual results were respectable, and the complication rate low.56, 57 For a period before the introduction of anti-VEGFs, 360-degree macular translocation, as it became known, was the most effective treatment for subfoveal CNV in ARMD. However, the surgery was lengthy and technically difficult, with a long learning curve. In an attempt to achieve similar results with a simpler operation, RPE translocation was introduced. The technique consisted of removal of the CNV, followed by cutting a full-thickness patch of RPE and choroid, and pulling it into position beneath the fovea (Figure 3).58 The procedure was relatively simple and quick, and there was no need for extraocular muscle surgery or silicone oil. Early studies showed that the patch supported visual function, but the visual angle of supported area was small, and the patches appeared to stop working after several years. Jan van Meurs, working in Rotterdam, modified the method by taking a patch from the peripheral retina.59 This had the advantage of moving the surgical trauma away from the fovea, and patches of any size could be created. However, the technique was more complicated, and it was found to be difficult to manoeuvre the patch into the subretinal space. This latter problem can been addressed by creating a 180-degree retinectomy and folding the temporal retina over the optic nerve, thereby creating a large area of exposed RPE so that the patch can be created and positioned without trauma to the retina.60 Once the RPE surgery is complete, the retina is folded back and re-attached using silicone oil. The peripheral RPE patches seem to have good long-term survival, and the visual results are reasonable.61

Autofluorescence image of a subfoveal RPE patch. The activity of the patch is in contrast to that of the surrounding defect in the RPE created by the removal of a type 1 CNV.
The introduction of anti-VEGFs revolutionised the treatment of CNV in ARMD, and the indications for vitreoretinal surgery reduced considerably. There are a few remaining indications such as RPE rips and subretinal haemorrhages, but very few cases are being done. However, this branch of surgery opened an important new frontier, and operations in the subretinal space are key to the success of two new areas of therapy, namely gene therapy62 and RPE transplantation.63 It is very likely that these two areas will be major subjects when the history of the next 25 years of vitreoretinal surgery is written.
References
Machemer R, Buettner H, Norton EWD, Parel JM . Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol 1971; 75: 813.
Kasner D . (1969) Vitrectomy: a new approach to management of vitreous. Highlights Ophthalmol 1969; 11: 304.
O’Malley C, Heintz RM . Vitrectomy with an alternative instrument system. Ann Ophthalmol 1975; 7: 585–594.
Escoffery RE, Olk RJ, Grand MG, Boniuk I . Vitrectomy without scleral buckling for primary rhegmatogenous retinal detachment. Am J Ophthalmol 1985; 99: 275–281.
Packo KH . Vail vitrectomy: controversial elitism or educational masterpiece? Retina Today 2012; 3: 22–25.
Duke-Elder S . System of Ophthalmology. Mosby: St Louis, 1941–1972.
Gass JDM . Idiopathic senile macular hole. Its early stages and pathogenesis. Arch Ophthalmol 1988; 106: 629–639.
de Bustros S . Vitrectomy for prevention of macular holes. Results of a randomized multicenter clinical trial. Vitrectomy for Prevention of Macular Hole Study Group. Ophthalmology 1994; 101: 1055–1059.
Kelly NE, Wendell RT . Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol 1991; 109: 654–659.
Fine SL . Vitreous surgery for macular hole in perspective. Is there an indication? Arch Ophthalmol 1991; 109: 635–636.
Freeman WR, Azen SP, Kim JW, el-Haig W, Mishell DR 3rd, Bailey I . Vitrectomy for the treatment of full-thickness stage 3 or 4 macular holes. Results of a multicentered randomized clinical trial. The Vitrectomy for Treatment of Macular Hole Study Group. Arch Ophthalmol 1997; 115: 11–21.
Ezra E, Munro PMG, Charteris DG, Aylward GW, Luthert PJ, Gregor ZJ . Macular hole opercula; ultrastructural features and clinicopathological correlation. Arch Ophthalmol 1997; 115: 1381–1387.
Gass JDM . Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol 1995; 119: 752–759.
Eckardt C, Eckardt U, Groos S, Luciano L, Reale E . Removal of the internal limiting membrane in macular holes: clinical and morphological findings. Ophthalmologe 1997; 94: 545–551.
Rodrigues EB, Maia M, Meyer CH, Penha FM, Dib E, Farah ME . Vital dyes for chromovitrectomy. Curr Opin Ophthalmol 2007; 18: 179–187.
Tadayoni R, Vicaut E, Devin F, Creuzot-Garcher C, Berrod JP, Le Mer Y et al. A randomized controlled trial of alleviated positioning after small macular hole surgery. Ophthalmology 2011; 118: 150–155.
Minihan M, Tanner V, Williamson TH . Primary rhegmatogenous retinal detachment: 20 years of change. Br J Ophthalmol 2001; 85: 546–548.
Heimann H, Hellmich M, Bornfeld N, Bartz-Schmidt KU, Hilgers RD, Foerster MH . Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment (SPR Study): design issues and implications. SPR Study report no. 1. Graefes Arch Clin Exp Ophthalmol 2001; 239: 567–574.
Heimann H, Bartz-Schmidt KU, Bornfeld N, Weiss C, Hilgers RD, Foerster MH et al. Scleral buckling versus primary vitrectomy in RRD. Ophthalmology 2007; 114: 2142–2154.
Brazitikos PD, Androudi S, Christen WG, Stangos NT . Primary PPV versus scleral buckle surgery for the treatment of pseudophakic RD. Retina 2005; 25: 957–964.
Devereaux PJ, Bhandari M, Clarke M, Montori VM, Cook DJ, Yusuf S et al. Need for expertise based RCTs. Br Med J 2005; 330: 88–91.
Sharma S . Meta-analysis of clinical trials comparing scleral buckling surgery to pneumatic retinopexy. Evidence-based Eye Care 2002; 3: 125–128.
Tornambe PE . Pneumatic retinopexy: the evolution of case selection and surgical technique. A twelve-year study of 302 eyes. Trans Am Ophthalmol Soc 1997; 95: 551–578.
Fujii GY, De Juan E, Humayun MS, Pieramici DJ, Chang TS, Awh C et al. The new 25 gauge instrument system for transconjunctival sutureless vitrectomy surgery. Ophthalmology 2002; 109: 1807–1812.
Fujii GY, De Juan E, Humayun MS, Chang TS, Pieramici DJ, Barnes A et al. Initial experience using the transconjunctival sutureless vitrectomy system for vitreoretinal surgery. Ophthalmology 2002; 109: 1814–1820.
Ibarra MS, Hermel M, Prenner JL, Hassan TS . Longer-term outcomes of transconjunctival sutureless 25-gauge vitrectomy. Am J Ophthalmol 2005; 139: 831–836.
Lakhanpal RR, Humayun MS, de Juan E Jr, Lim JI, Chong LP, Chang TS et al. Outcomes of 140 consecutive cases of 25-gauge transconjunctival surgery for posterior segment disease. Ophthalmology 2005; 112: 817–824.
Shimada H, Nakashizuka H, Mori R, Mizutani Y . Expanded indications for 25-gauge transconjunctival vitrectomy. Jpn J Ophthalmol 2005; 49: 397–401.
Kellner L, Wimpissinger B, Stolba U, Brannath W, Binder S . 25 gauge versus 20 gauge system for pars plana vitrectomy: a prospective randomized clinical trial. Br J Ophthalmol 2007; 91: 945–948.
Inoue M, Noda K, Ishida S, Nagai N, Imamura Y, Oguchi Y . Intraoperative breakage of a 25-gauge vitreous cutter. Am J Ophthalmol 2004; 138: 867–869.
Eifrig CW, Scott IU, Flynn HW, Smiddy WE, Newton J . Endophthalmitis after pars plana vitrectomy: incidence, causative organisms, and visual acuity outcomes. Am J Ophthalmol 2004; 138: 799–802.
Taylor SR, Aylward GW . Endophthalmitis following 25-gauge vitrectomy. Eye 2005; 19: 1228–1229.
Acar N, Unver YB, Altan T, Kapran Z . Acute endophthalmitis after 25-gauge sutureless vitrectomy. Int Ophthalmol 2007; 27: 361–363.
Kunimoto DY, Kaiser RS, Wills Eye Retina Service.. Incidence of endophthalmitis after 20- and 25-gauge vitrectomy. Ophthalmology 2007; 114: 2133–2137.
Scott IU, Flynn HW Jr, Dev S, Shaikh S, Mittra RA, Arevalo JF et al. Endophthalmitis after 25-gauge and 20-gauge pars plana vitrectomy: incidence and outcomes. Retina 2008; 28: 138–142.
Shimada H, Nakashizuka H, Hattori T, Mori R, Mizutani Y, Yuzawa M . Incidence of endophthalmitis after 20- and 25-gauge vitrectomy. Ophthalmology 2008; 115: 2215–2220.
O’Reilly P, Beatty S . Transconjunctival sutureless vitrectomy: Initial experience and surgical tips. Eye 2007; 21: 518–521.
Chen CJ, Satofuka S, Inoue M, Ishida S, Shinoda K, Tsubota K . Suprachoroidal hemorrhage caused by breakage of a 25-gauge cannula. Ophthal Surg Lasers Imaging 2008; 39: 323–324.
Kapamajian M, Gonzales CR, Gupta A, Schwartz SD . Suprachoroidal hemorrhage as an intraoperative complication of 25-gauge pars plana vitrectomy. Semin Ophthalmol 2007; 22: 197–199.
Shimada H, Nakashizuka H, Mori R, Mizutani Y, Hattori T . 25-gauge scleral tunnel transconjunctival vitrectomy. Am J Ophthalmol 2006; 142: 871–873.
Singh RP, Bando H, Brasil OF, Williams DR, Kaiser PK . Evaluation of wound closure using different incision techniques with 23-gauge and 25-gauge microincision vitrectomy systems. Retina 2008; 28: 242–248.
Taban M, Ufret-Vincenty RL, Sears JE . Endophthalmitis after 25-gauge transconjunctival sutureless vitrectomy. Retina 2006; 26: 830–831.
Eckardt C . Transconjunctival sutureless 23-gauge vitrectomy. Retina 2005; 25: 208–211.
Hikichi T, Matsumoto N, Ohtsuka H, Higuchi M, Matsushita T, Ariga H et al. Comparison of one-year outcomes between 23- and 20-gauge vitrectomy for preretinal membrane. Am J Ophthalmol 2009; 147: 639–643.
Wickham L, Bunce C, Kwan AS, Bainbridge J, Aylward GW . A pilot randomised controlled trial comparing the post-operative pain experience following vitrectomy with a 20-gauge system and the 25-gauge transconjunctival system. Br J Ophthalmol 2010; 94: 36–40.
Scartozzi R, Bessa AS, Gupta OP, Regillo CD . Intraoperative sclerotomy-related retinal breaks for macular surgery, 20- vs 25-gauge vitrectomy systems. Am J Ophthalmol 2007; 143: 155–156.
Lafeta AP, Claes C . Twenty-gauge transconjunctival sutureless vitrectomy trocar system. Retina 2007; 27: 1136–1141.
Gotzaridis EV . Three-port 20-gauge transconjunctival pars plana vitrectomy. Retina 2007; 27: 382–384.
Saad A, Assi A . Modified 20-gauge sutureless single-step sclerotomies for pars plana vitrectomy. Retina 2009; 29: 848–853.
Thomas MA, Kaplan JH . Surgical removal of subfoveal neovascularisation in the presumed ocular histoplasmosis syndrome. Am J Ophthalmol 1991; 111: 1–7.
Berger AS, Kaplan HJ . Clinical experience with the surgical removal of subfoveal neovascular membranes. Short-term postop results. Ophthalmology 1993; 100: 5–6.
Gass JDM . Biomicroscopic and histopathologic considerations regarding the feasibility of surgical excision of CNV. Am J Ophthalmol 1994; 118: 285–298.
Submacular Surgery Trials (SST) Research Group. Surgery for subfoveal choroidal neovascularization in age-related macular degeneration: ophthalmic findings, SST Report no. 11. Ophthalmology 2004; 111: 1967–1980.
Submacular Surgery Trials Research Group.. Surgical removal vs observation for subfoveal choroidal neovascularization, either associated with POHS or idiopathic. SST report no 9. Arch Ophthalmol 2004; 122: 1597–1611.
Machemer R, Steinhorst UH . Retinal separation, retinotomy, and macular relocation II. Graefes Arch Clin Exp Ophthalmol 1993; 231: 635–641.
Eckardt C, Eckardt U, Conrad HG . Macular rotation with and without counter-rotation in patients with ARMD. Graefes Arch Clin Exp Ophthalmol 1999; 237: 313–325.
Mruthyunjaya P, Stinnett SS, Toth CA . Change in visual function after macular translocation with 360 degrees retinectomy for neovascular age-related macular degeneration. Ophthalmology 2004; 111: 1715–1724.
Stanga PE, Kychenthal A, Fitzke FW, Halfyard AS, Chan R, Bird AC et al. Retinal pigment epithelium translocation and central visual function in age related macular degeneration: preliminary results. Int Ophthalmol 2001; 23: 297–307.
Joussen AM, Heussen FM, Joeres S, Llacer H, Prinz B, Rohrschneider K et al. Autologous translocation of the choroid and retinal pigment epithelium in age-related macular degeneration. Am J Ophthalmol 2006; 142: 17–30.
Cereda MG, Parolini B, Bellesini E, Pertile G . Surgery for CNV and autologous choroidal RPE patch transplantation: exposing the submacular space. Graefes Arch Clin Exp Ophthalmol 2010; 248: 37–47.
Maaijwee K, Heimann H, Missotten T, Mulder P, Joussen A, van Meurs J . Retinal pigment epithelium and choroid translocation in patients with exudative age-related macular degeneration: long-term results. Graefes Arch Clin Exp Ophthalmol 2007; 245: 1681–1689.
Bainbridge JW, Smith AJ, Barker SS, Robbie S, Henderson R, Balaggan K et al. Effect of gene therapy on visual function in Leber's congenital amaurosis. N Engl J Med 2008; 358: 2231–2239.
Ramsden CM, Powner MB, Carr AJ, Smart MJ, da Cruz L, Coffey PJ . Stem cells in retinal regeneration: past, present and future. Development 2013; 140: 2576–2585.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The author declares no conflict of interest.
Additional information
The content of this article is based on a presentation at the Annual Congress of the Royal College of Ophthalmologists, 2013.
Rights and permissions
About this article

Cite this article
Aylward, G. 25th RCOphth Congress, President's Session paper: 25 years of progress in vitreoretinal surgery. Eye 28, 1053–1059 (2014). https://doi.org/10.1038/eye.2014.142
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2014.142
This article is cited by
-
Outcomes of pars plana vitrectomy following ocular trauma at varying surgical time points
International Journal of Retina and Vitreous (2022)
-
Optimal timing of vitrectomy for severe mechanical ocular trauma: A retrospective observational study
Scientific Reports (2019)
