
Abstract
Aims
The outcomes of laser-assisted in situ keratomileusis (LASIK) operations performed with the Classic FEMTO LDV femtosecond laser using the plastic single-use suction ring (Ziemer Ophthalmic Systems) and the Allegretto Wave Concerto 500 Hz excimer laser (Wavelight AG) are presented in terms of accuracy, predictability, and safety of the operation.
Methods
A FEMTO LDV plastic suction ring was used for flap creation in 342 eyes of 179 patients. The intended flap thickness was 90 μm. The size of the suction ring varied from 9.0 to 10.0 mm. Flap dimensions were measured and correlated to preoperative characteristics.
Results
Mean flap thickness was very constant, 89.6±2.0 μm (range 84–97). In 163 bilateral operations, the second flap was 1.1 μm thinner than the one cut first (P<0.0001). Mean flap diameter was 9.4±0.2 mm (range 8.1–9.9). Mean hinge length was 3.9±0.2 mm (range 3.0–4.2). In hyperopic eyes, flap thickness correlated negatively with keratometric power K1 and flap diameter. In hyperopic eyes, flap diameter correlated positively with spherical equivalent refraction and with keratometric power K1 as well as hinge length both in myopic and hyperopic eyes. Complications were reported in 12 (3.5%) eyes. Complications were very mild and none of them prevented further refractive laser treatment. Two Snellen lines of corrected distance visual acuity were lost in one (0.3%) eye.
Conclusion
The FEMTO LDV plastic single-use suction rings yielded accurate and reproducible flaps and were safe for the creation of thin corneal flaps.
Similar content being viewed by others
Introduction
Laser-assisted in situ keratomileusis (LASIK) remains to be the most commonly used refractive surgery technique for the correction of myopia, hyperopia, and astigmatism.1 The first phase of LASIK, the creation of a corneal flap, is the most critical step of LASIK and it affects the visual outcome of the whole procedure. The technological evolution of flap creation has emerged from manually guided mechanical microkeratomes to automated microkeratomes, single-use microkeratomes, and most recently to femtosecond laser technology. There are several femtosecond lasers on the market, including Intralase (Abbot Medical Optics, Irvine, CA, USA),2, 3, 4, 5 FEMTO LDV (Ziemer Ophthalmic Systems, Port, Switzerland),6 FEMTEC (20/10 Perfect Vision, Heidelberg, Germany),7 and VisuMax (Carl Zeiss Meditec, Jena, Germany).8, 9 Femtosecond laser technology has been shown to have some advantages in comparison to microkeratome, for example, less variation in flap thickness and a more uniform flap thickness throughout the whole flap compared with microkeratome-based flap.2, 5, 10, 11, 12 In the present study, the use of disposable plastic suction ring with the Ziemer femtosecond laser FEMTO LDV was evaluated in 342 eyes in terms of accuracy, predictability, safety, and complications. Recently, disposable suction rings have gained popularity because of microbiological safety to avoid sterilization process.
Patients and methods
Study design
A retrospective, computer-based review of the records of 342 consecutive eyes of 179 patients, who underwent LASIK flap creation with the Classic FEMTO LDV femtosecond laser using the plastic disposable suction ring at Mehiläinen Hospital in Tampere (Finland) between October 2010 and April 2011, was performed. The principles of the Declaration of Helsinki and good clinical practice guidelines were followed. The Ethics Committee at the University Hospital of Tampere declared that this type of a retrospective study waived the need for the Ethics Committee approval, in accordance with the Finnish law on human clinical trials.
All eyes were operated by the same surgeon (JP). In bilateral operations of 163 patients, the right eye was operated first. The same disposable suction ring and intershield was used for the left eye. The eyes were analyzed as myopic or hyperopic groups based on the spherical equivalent refraction (SE); 285 eyes having SE <0.0 D were classified myopic and 57 eyes having SE ≥+0.0 D were classified hyperopic.
Preoperative examinations
All patients had a complete preoperative ophthalmologic examination before the LASIK surgery to exclude any severe pathology that might be a contraindication for surgery or have an effect on flap creation. The examination included determination of manifest refraction, measurement of uncorrected and corrected visual acuities, wavefront analysis (Allegro Analyzer; Wavelight AG, Erlangen, Germany), biomicroscopy, fundus examination, measurement of three-dimensional corneal topography (Allegro Oculyzer; Wavelight AG), measurement of intraocular pressure (Nidek Tonoref RKT-7700; Gamagori, Aichi, Japan), and indirect ophthalmoscopy.
Surgical technique
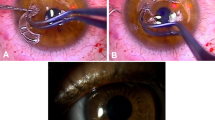
Before the surgery, topical anesthetic oxybuprocain hydrochloride (Oftan Obucain; Santen Oy, Tampere, Finland) was instilled into the operated eyes. An aspirating lid speculum (no. 15961; Geuder, Heidelberg, Germany) was used in most of the eyes. Barraquer wired lid speculum was used in eight small eyes when the cone of the FEMTO LDV femtosecond laser did not fit otherwise. Preoperative corneal thickness was measured with ultrasonic pachymetry (SP-3000; Tomey Corp., Nagoya, Japan). The mean of three pachymetry measurements before and after the flap cut was noted. The corneal flap was cut with the FEMTO LDV as described previously.6 The aimed flap thickness was 90 μm in all the eyes and was determined with the appropriate intershield. The size of the suction ring was typically 9.5 mm (331 eyes), but was 9.0 mm in 10 eyes and 10.0 mm in one eye depending on the corneal curvature. The size of the hinge width was set to 0.3 mm, which generated approximately 4.0-mm hinge length. Central stromal thickness was measured three times immediately after the flap cut without moisturizing the stromal bed. Flap thickness was then calculated by using the subtraction method. The horizontal white-to-white distance of the eye, flap diameter, and hinge length were measured by a standard caliper. The excimer laser treatment was started immediately thereafter using the Allegretto Wave Concerto 500 Hz excimer laser (Wavelight AG) because typically the FEMTO LDV did not cause any opaque bubble layer (OBL) in the interphase. All complications during the procedure and the 1-month follow-up were recorded.
Statistical analysis
Means and standard deviations for flap thickness, horizontal flap diameter, and hinge length of the operated eyes were calculated. Single variable correlation of flap thickness and preoperative spherical equivalent refraction, corneal thickness, age, keratometric power K1, flap diameter, and hinge length was evaluated using GraphPad Prism software (GraphPad, San Diego, CA, USA). Myopic and hyperopic subgroups were analyzed separately.
Results
The mean age of 342 patients was 37.7±11.3 years (range 17–66 years). Mean SE in myopic eyes was −4.24±2.19 D (range −0.13 to −12.63 D) and in hyperopic eyes +2.02±1.25 D (range 0 to +5.25 D). Other preoperative characteristics of 342 eyes are presented in Table 1.
The FEMTO LDV plastic suction ring produced very constant flap thickness (Table 2). Mean flap thickness was 89.6±2.0 μm (range 84–97 μm). Mean flap diameter was 9.4±0.2 mm (range 8.1–9.9 mm). Mean hinge length was 3.9±0.2 mm (range 3.0–4.2 mm). In bilateral operations, the second flap was 1.1 μm thinner than the first cut flap (P<0.0001). Flap diameter in eyes treated with the 9.5-mm suction ring did not differ significantly between the right and the left eye (9.4±0.2 vs 9.4±0.2 mm). However, hinge length differed significantly between the right and the left eye (4.0±0.1 vs 3.8±0.2 mm, P<0.0001).
The correlation coefficients of preoperative characteristics vs flap thickness are presented in Table 3. In hyperopic eyes, flap thickness correlated negatively with keratometric power K1 (r=−0.33, P<0.05; Figure 1a). The correlations of different flap characteristics were also analyzed and presented in Table 3. Flap diameter correlated negatively with flap thickness in 55 hyperopic eyes that were treated with the 9.5-mm suction ring for flap diameter (r=−0.29, P<0.05; Figure 1b). Moreover, in 269 myopic eyes treated with the 9.5-mm suction ring, hinge length correlated positively with flap thickness (r=0.20, P<0.01; Figure 1c). The correlation coefficients of preoperative characteristics and flap characteristics of the eyes treated with the 9.5-mm suction ring are presented in Table 4. In hyperopic eyes, flap diameter correlated positively with spherical equivalent refraction (r=0.29, P<0.05; Figure 1d). Moreover, flap diameter correlated positively with the keratometric power K1 both in myopic eyes (r=0.38, P<0.0001; Figure 1e) and hyperopic eyes (r=0.31, P<0.05; Figure 1f). Flap diameter also correlated positively with hinge length both in myopic eyes (r=0.15, P<0.0001; Figure 1g) and hyperopic eyes (r=0.30, P<0.05; Figure 1h).

(a) Keratometric power K1 and flap thickness (μm) in 57 hyperopic eyes treated with the FEMTO LDV single-use suction ring (r=−0.33, P=0.01). Mean keratometric power was 42.61±1.18 D. Increasing flap thickness was associated with flatter keratometric power K1. (b) Flap diameter (mm) and flap thickness (μm) in 55 hyperopic eyes treated with the FEMTO LDV single-use 9.5-mm suction ring (r=−0.29, P=0.03). Mean flap diameter was 9.34±0.22 mm. Increasing flap thickness was associated with smaller flap diameter. (c) Hinge length (mm) and flap thickness (μm) in 269 myopic eyes treated with the FEMTO LDV single-use 9.5-mm suction ring (r=0.20, P=0.001). Mean hinge length was 3.89±0.38 mm. Increasing flap thickness was associated with wider hinge length. (d) SE refraction (D) and flap diameter (mm) in 55 hyperopic eyes treated with the FEMTO LDV single use 9.5-mm suction ring (r=0.29, P=0.031). Mean SE was +2.02±1.26 D. Increasing flap diameter was associated with increasing spherical equivalent refraction. (e) Keratometric power K1 (D) and flap diameter (mm) in 276 myopic eyes treated with the FEMTO LDV single-use 9.5-mm suction ring (r=0.38, P<0.0001). Mean keratometric power was 43.09±1.13 D. Increasing flap diameter was associated with increasing keratometric power K1. (f) Keratometric power K1 (D) and flap diameter (mm) in 55 hyperopic eyes treated with the FEMTO LDV single-use 9.5-mm suction ring (r=0.31, P=0.022). Mean keratometric power was 42.56±1.18 D. Increasing flap diameter was associated with increasing keratometric power K1. (g) Hinge length (mm) and flap diameter (mm) in 269 myopic eyes treated with the FEMTO LDV single-use 9.5-mm suction ring (r=0.15, P<0.0001). Mean hinge length was 3.91±0.18 mm. Increasing flap diameter was associated with increasing hinge length. (h) Hinge length (mm) and flap diameter (mm) in 55 hyperopic eyes treated with the FEMTO LDV single-use 9.5-mm suction ring (r=0.30, P=0.027). Mean hinge length was 3.92±0.16 mm. Increasing flap diameter was associated with increasing hinge length.
Complications were reported in 12 eyes out of 342 (3.5%) eyes. Intershield problem was reported in two (0.6%) eyes, OBL in two (0.6%) eyes, epithelial defect in one (0.3%) eye, free cap in two (0.6%) eyes, and preserved free cap in five (1.5%) eyes. In preserved free caps, the FEMTO LDV cut a complete flap without a hinge. In those cases, the surgeon opened the free flap so that the hinge of 3–4 mm was preserved. Bleeding occurred in 38 eyes of 342 eyes operated (11.1%). All the complications were regarded as minor and did not prevent the continuation of the refractive surgery with excimer laser.
The safety analysis is based on the follow-up data of 338 eyes after 1 month at the time of the analysis. Two patients (four eyes) were lost in the follow-up. Two Snellen lines of corrected distance visual acuity (CDVA) were lost in one (0.3%) eye and two lines were gained in 2 (0.6%) eyes. In the eye that lost two lines of CDVA an OBL occurred.
Discussion
In 342 eyes treated with the FEMTO LDV plastic single-use suction ring, flap thickness was very constant and averaged 89.6±2.0 μm (range 84–97 μm). In bilateral operations, the second flap was significantly thinner than the first cut flap (right eye 90.1±2.0 μm vs left eye 89.0±1.8 μm, P<0.0001). This difference of only 1.1 μm is not, however, clinically significant. Mean hinge length averaged 3.9±0.2 mm in both eyes. In our previous study, when we used the reusable FEMTO LDV suction ring in 787 eyes, flap thickness averaged 90.0±5.0 μm.6 In it, the first and second cut flaps did not differ significantly (right eye 90.0±5.5 μm vs left eye 90.1±4.6 μm). Thus, both reusable and disposable suction rings gave similar results for flap characteristics. One limitation of our study was the use of ultrasonic pachymetry instead of online optical coherence pachymetry.13
The overall accuracy and predictability of present study was very good. Therefore, we could find some correlations in which the clinical significance obviously is not very important. Flap thickness correlated negatively with keratometric power K1 and flap diameter in hyperopic eyes. In these eyes, increasing flap thickness was associated with flatter keratometric power K1 and smaller flap diameter. In myopic eyes, flap thickness correlated positively with hinge length. Increasing flap thickness was associated with wider hinge length. Increasing flap diameter was associated with increasing hyperopia. Moreover, flap diameter correlated positively with the keratometric power K1 both in myopic and hyperopic eyes. Flap diameter also correlated positively with hinge length both in myopic and hyperopic eyes.
In our previous study with the FEMTO LDV, we found that achieved flap thickness was slightly dependent on corneal thickness and keratometric value K1.6 Increasing flap thickness was associated with increasing corneal thickness and flatter keratometric value. Furthermore, we found that increasing flap diameter was associated with thinner flap thickness in myopic eyes.6 With the reusable 9.0-mm suction ring, increasing flap diameter was associated with increasing preoperative spherical equivalent refraction in myopic eyes. In all eyes treated with the 9.0-mm suction ring, increasing flap diameter was associated with steeper keratometric value K1. In hyperopic eyes, increasing flap diameter was also associated with increasing hinge. Using femtosecond laser technology in 1000 consecutive Intralase flaps, Binder5 found that preoperative corneal thickness or keratometric power did not affect the flap thickness achieved. This difference is due to the technical differences between Intralase and FEMTO LDV not yet known in details.
In the present study, complications were reported in 12 (3.5%) eyes; intershield problem was reported in two eyes, OBL in two eyes, epithelial defect in one eye, free cap in two eyes, and preserved free cap in five eyes. The intershield problem occurred because the intershield came off the window during the flap cut or at the time when the suction was taken. The laser burned the edges afterwards. These intershield problems occurred although we used sterile water. This usually happens if balanced salt solution (BSS) is used instead of sterile water to apply the foil onto the handpiece. The adhesion force of water is smaller than that of BSS. Therefore, it is important to use sterile water to apply the foil. The OBL in two eyes occurred at the hinge outside the flap margins. These complications were very mild and none of them prevented further refractive laser treatment. In comparison to our previous FEMTO LDV study,6 the complication rate was 8.4%.
Recommendations and conclusions
Although in this study we used the 0.3-mm hinge width, we recommend changing to the 0.4-mm hinge width to avoid free caps observed in this study. In typical cases, our recommendation is to use the 9.5-mm suction ring. In the cases when the keratometric value K1 is >46 D, we recommend using the 9.0-mm suction ring. When the keratometric value K1 is ≤41 D, our recommendation is the 10.0-mm suction ring. In the hands of an experienced surgeon, the method of LASIK with the FEMTO LDV combined with plastic single-use suction rings appears to be a predictable and safe procedure that yields flap characteristics very comparable to the reusable suction ring.

References
Duffey RJ, Leaming D . US trends in refractive surgery: 2004 ISRS/AAO Survey. J Refract Surg 2005; 21: 742–748.
Binder PS . Flap dimensions created with the IntraLase FS laser. J Cataract Refract Surg 2004; 30: 26–32.
Kezirian GM, Stonecipher KG . Comparison of the IntraLase femtosecond laser and mechanical keratomes for laser in situ keratomileusis. J Cataract Refract Surg 2004; 30: 804–811.
Lim T, Yang S, Kim M, Tchah H . Comparison of the IntraLase femtosecond laser and mechanical microkeratome for laser in situ keratomileusis. Am J Ophthalmol 2006; 141: 833–839.
Binder PS . One thousand consecutive IntraLase laser in situ keratomileusis flaps. J Cataract Refract Surg 2006; 32: 962–969.
Pietilä J, Huhtala A, Jääskeläinen M, Jylli J, Mäkinen P, Uusitalo H . LASIK flap creation with the Ziemer femtosecond laser in 787 consecutive eyes. J Refract Surg 2010; 26: 7–16.
Holzer MP, Rabsilber TM, Auffarth GU . Femtosecond laser-assisted corneal flap cuts: morphology, accuracy, and histopathology. Invest Ophthalmol Vis Sci 2006; 47: 2828–2831.
Reinstein DZ, Archer TJ, Gobbe M, Johnson N . Accuracy and reproducibility of artemis central flap thickness and visual outcomes of LASIK with the Carl Zeiss Meditec VisuMax femtosecond laser and MEL 80 excimer laser platforms. J Refract Surg 2010; 26: 107–119.
Blum M, Kunert K, Gille A, Sekundo W . LASIK for myopia using the Zeiss VisuMax femtosecond laser and MEL 80 excimer laser. J Refract Surg 2009; 25: 350–356.
Talamo JH, Meltzer J, Gardner J . Reproducibility of flap thickness with IntraLase FS and Moria LSK-1 and M2 microkeratomes. J Refract Surg 2006; 22: 556–561.
Alio JL, Pinero DP . Very high-frequency digital ultrasound measurement of the LASIK flap thickness profile using the IntraLase femtosecond laser and M2 and Carriazo-Pendular microkeratomes. J Refract Surg 2008; 24: 12–23.
Sutton G, Hodge C . Accuracy and precision of LASIK flap thickness using the IntraLase femtosecond laser in 1000 consecutive cases. J Refract Surg 2008; 24: 802–806.
Zhou Y, Zhang J, Tian L, Zhai C . Comparison of the Ziemer FEMTO LDV femtosecond laser and Moria M2 mechanical microkeratome. J Refract Surg 2012; 28: 189–194.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Dr Pietilä has financial interest in the FEMTO LDV. The other authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Pietilä, J., Huhtala, A., Mäkinen, P. et al. Flap characteristics, predictability, and safety of the Ziemer FEMTO LDV femtosecond laser with the disposable suction ring for LASIK. Eye 28, 66–71 (2014). https://doi.org/10.1038/eye.2013.244
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2013.244
