
Abstract
Aims
To compare methods to measure time outdoor and light levels, two possible predictors of myopia, in Singapore children.
Methods
Outdoor time from a diary and portable light meter over a 1-week period was compared in 117 Singapore children aged 6–12 years with and without myopia. All children wore a (HOBO Pendant temp/light Part # UA-002-64) light meter for 1 week and the parents filled the 7-day outdoor diary to track the outdoor activity.
Results
Mean outdoor time from diary and time with light levels was 5.44 hours per week and 7.91 hours per week, respectively, during school term and school holidays. Time spent with light levels of >1000 Lux from the light meter were 7.08 h per week and 9.81 h per week, respectively, during school term and school holidays. The intraclass correlation coefficients were 0.21 and 0.28 for outdoor time from the diary and light meter (1000 Lux cut-off) during the school term and holidays, respectively. The correlation coefficient was 0.34 (95% CI 0.05, 0.58) for a weekday during school holidays, 0.17 (−0.14, 0.45) for a weekday during school term, 0.07 (−0.16, 0.29) for a weekday during school term, and 0.25 (0.02, 0.46) for a weekend during school term.
Conclusions
The agreement between the light meter and 1-week diary was poor to fair. Both instruments measure different parameters, time outdoors and light intensity, and could therefore capture different aspects of risk in future myopia studies.
Similar content being viewed by others


Introduction
Myopia is a public health problem in East Asia, with prevalence rates in Singapore of 8% in 5-year olds1 and 36.3% in 7–9-year-old school children,2 and nearly 40% in adults ≥40 years.3
Although there have been many studies that have documented the risk factors for myopia, there is no conclusive evidence that modifying these risk factors may have an impact on the prevalence of myopia. In one study, amongst 6-year-old Chinese children, the prevalence rate was 29.1% in those living in Singapore, compared with 3.3% in those living in Sydney, Australia.4 The main difference found for this disparity was the differential in time spent outdoors between these two groups, estimated to be 13.8 h per week in Sydney compared with 3.0 h per week in Singapore. Similarly, in the Sydney Myopia Study, it was reported that an increase in time spent outdoors was significantly associated with a lower myopia prevalence in 12-year-old Australian children.4 Singapore children with increased hours of outdoor activity were less likely to be myopic.5 Few factors may underlie the relationship between outdoor time and myopia. The first is that an increased light intensity may trigger dopamine release and inhibit eye growth.6, 7, 8 Animal studies in chicks show that under light–dark cycles, light intensity is an environmental factor that modulates the process of emmetropization. Low intensity of ambient light is a risk factor for developing myopia.9 The second is that ultraviolet light exposure and increased vitamin D levels may protect from myopia.10, 11 Other postulated mechanisms for the protective effect of outdoor time on myopia are distance viewing with a clear periphery and minimal defocus that may protect from myopia.4
As a result of these observations, several randomized clinical trials of outdoor interventions to prevent myopia are being developed globally. For these to be successful, however, accurate assessments of time outdoors and exposure to high light intensities are required. Two strategies for assessing these indicators are light meters and outdoor diaries. A light meter accurately measures light intensity both inside and outside, assuming that the meter is worn as intended. The light exposure patterns were analyzed in 12 children aged 13–14 years in New Zealand using a portable light meter, and it has been shown that a small amount of time outdoors was linked to a large proportion of light exposure.12 In the United States, time outdoors from a questionnaire and light exposure patterns were evaluated in seven adults.13 Both pilot studies were limited by very small sample sizes and there were no direct prospective diary estimates of outdoor activities from the start to the end of the day. Diaries can be used to assess outdoor time but are based on self-(or parent) report, and are thus prone to measurement error and underreporting. However, for studies aiming to quantify the relationship between light intensity, outdoor time, and myopia, use of both diaries and light meters may be preferable to using either alone. The diaries can be used to identify whether high light exposure occurs indoors or outdoors and the light meter can validate the self-reported data.
The goal of this study was to compare the measurements of outdoor time using a newly developed outdoor activities diary with a more objective portable light meter measurement over a 1-week period in Singapore Chinese school children. Differential light intensity levels in outdoor conditions and outdoor/light patterns during different time periods were evaluated.
Materials and methods
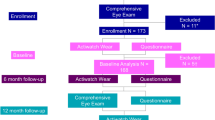
Data were analyzed for 117 children who were part of a family-based outdoor intervention trial, the Family Incentive Trial (FIT) (n=285). The FIT trial is a randomized community trial designed to evaluate whether an outdoor, physical activity, health behavior intervention will increase outdoor time and improve fitness. Myopia was defined as a spherical equivalent refraction of at least −0.50 D. Myopic and non-myopic children, aged 6–12 years were enrolled for the study. Children with medical conditions such as type 1 diabetes, severe asthma, cancer, or mental illness were excluded from the study. The study was approved by the Institutional Review Board of the National University of Singapore, and followed the tenets of the Declaration of Helsinki. Written consent was obtained from the parents after the study was explained.
Light meter
With parental guidance, all children wore a light meter (HOBO Pendant temp/light Part # UA-002-64; Microdaq.com (Ltd), Contoocook, NH, USA) continuously for 7 days. The light meter was portable, waterproof, and contained a light sensor that recorded the amount and duration of exposure to white light illuminance in lux (1 lumen per square meter) every 5 min from the beginning to the end of the day. The light meter was worn on the shirt using a safety pin, with the light sensor facing outward. Emails were sent and phone calls were made to the parents and children once during the week to ensure compliance.
Outdoor diary
The 1-week outdoor activity diary was structured to track all activities during weekdays and weekends (Supplementary Appendix). This diary is an adaptation of the Child Development Supplement-III 2007. The diary detailed the start time and end time of each activity and the type of activity. Activities that were performed outside a building, for example, park visits, walking around the neighborhood, and outdoor sports, were classified as outdoor activities. Indoor activities were those that were performed inside a building or an enclosed space and included travelling in a car, bus, or train, as the light levels in these vehicles in Singapore were low. Only daylight hours from 7 am to 7 pm were considered for the comparison of outdoor time from the diary with the light meter.
Pilot test
Two staff wore the light meter under five different testing conditions: (i) outdoors—bright sunny day, (ii) outdoors—dark cloudy day, (iii) indoor in an enclosed space, (iv) indoors—near a window with a stream of bright sunlight, and (v) indoors—light meter not worn and left on a table.
Statistical analysis
The data were analyzed using SAS version 9.2 (SAS Institute, Cary, NC, USA).
We derived the total outdoor time for each child from both the light meter and the diary from 7am to 7pm when there is sunlight. For the light meter, a low-intensity reading may be obtained even if the child was staying indoors. Therefore, for any day with all intensity readings <100 Lux, it was assumed that the child forgot to wear the light meter on that day and hence that day was not included in the analysis. The number of 5-minute intervals with light intensity larger than the cut-off value of 1000 Lux were counted to obtain total outdoor time. The average outdoor times for weekdays, weekend, and the whole week were computed. A two-samples t-test was used to compare the mean outdoor time between school term and school holiday and a paired t-test was used to compare the mean outdoor time between a weekday and a weekend. The outdoor times measured by the light meter and the diary were compared by intraclass correlation coefficient.
Results
There were 60 boys, 57 girls and 103 Chinese, 8 Indians, and 6 of other races who wore the light meter and completed the diary from both arms. The mean age was 8.3 years (SD=1.6). Around 55.6% of participants were myopic. Figure 1 depicts the light levels during the day for a child on a weekday and weekend. The indoor light intensity levels were very low and most of the time <1000 Lux whereas there was a variation outdoors from tens of thousands of Lux on a sunny day to a few thousand Lux on cloudy days with an overcast sky.


(a) Light meter and outdoor readings hour by hour on a weekday for one child. (b) Light meter and outdoor readings hour by hour on a weekend for one child.
The light meter readings in different conditions by two staff were as follows: on a bright sunny day outside, means=278919 and 30311 Lux; on a dark cloudy day outside, means=3896 and 7559 Lux; indoors in an enclosed space, means=3.5 and 8.0 Lux; indoors near a window with a stream of bright sunlight, means=1573 and 4445 Lux, and indoors with a light meter not worn and left on a table, means=54 and 129 Lux. There was an overlap with means of 3896 and 7559 for outdoors on a dark cloudy day outdoors and means of 1573 and 4445 for indoors with bright light streaming through the window.
The mean time outdoor from the diary was 5.44 h per week and 7.91 h per week, respectively, during the school term and school holidays (Table 1) (P=0.004). During the school term, the mean time outdoors was 0.58 h per day on a weekday compared with 1.27 h per day on a weekend (paired t-test P<0.001). During school holidays, the mean outdoor time was 0.96 h per day on weekday and 1.56 h per day on weekend (paired t-test P=0.005). Time spent with light levels of >1000 Lux from the light meter, during school term and school holidays were 7.08 h per week and 9.81 h per week, respectively (P<0.001). During the school term, children spent 0.88 h and 1.36 h per day on a weekday and weekend, respectively (P<0.001). During school holidays, the time spent outdoors was 1.34 h and 1.54 h per day on a weekday and weekend, respectively (P=0.296). The mean Lux levels were 702.87 Lux during the school term and 950.85 Lux during the school holidays.
During school term, the mean outdoor time from the diary (5.44 hours/week) was significantly lower compared with that from the light meter (7.08 hours/week) (P=0.0034), whereas the outdoor times from the diary (7.91 hours/week) and the light meter (9.81 hours/week) were not significantly different during school holidays (P=0.1693).
During school term weekday, the mean outdoor time from the diary (0.88 hours per day) was significantly lower compared with that from the light meter (0.58 hours per day) (P<0.0001), whilst it was not significantly different on a weekend (P=0.4475). The mean outdoor times from the diary and the light meter during school holidays were not significantly different both on a weekday (P=0.066) and a weekend (P=0.5513).
Outdoor time assessed by the diary on weekdays and weekends (P=0.23, 0.75), and light meter (P=0.19, 0.64) amongst 65 myopic and 52 non-myopic children in our study were not significant (Table 2). However, this secondary analysis was limited by a small sample size.
The intraclass correlation coefficients were 0.21 and 0.28 of outdoor time from the diary and light meter (1000 Lux cut-off) during the school term and holidays, respectively (Figures 2a and 2b). The correlation coefficient was 0.34 (95% CI 0.05, 0.58) during a weekday while school holidays, 0.17 (−0.14, 0.45) during a weekday while school term, 0.07 (−0.16, 0.29) during a weekday while school term, and 0.25 (0.02, 0.46) during a weekend while school term.

(a) Scatterplots of time outdoors from the light meter (>1000 Lux) and diary during the school term. (b) Scatterplots of time outdoors from the light meter (>1000 Lux) and diary during the school holidays.
Discussion
The agreement between the diary and light meter was only poor-to-fair as both instruments had limitations. Differences may be because of inaccurate recording of diary data or the lack of a clear-cut difference in light intensities indoors vs outdoors. The mean light levels outdoors in Singapore were, respectively, slightly lower than prior reports at 670.9 Lux and 911.9 Lux during the school term and school holidays. Our data suggest that both instruments measure different parameters and could therefore capture different aspects of risk in future myopia studies.
We set the threshold lux level for outdoor activity as 1000 Lux based on similar cut-off points of 1000 Lux and 882 Lux from previous studies.12, 13 The mean outdoor time from the diary did not compare exactly with the light meter using the best cut-off of 1000 Lux. Parents may not have accurately completed the diary, and time spent in conditions with higher light levels may not be analogous to time outdoors. Our results of poor-to-fair correlations are similar to previous studies.12, 13 However, the light meter measurements allow us to check and validate the accuracy of diary data if the light intensities do not match the reported activities.
The mean outdoor time from the diary during school term (5.44 h per week) and school holidays (7.91 h per week) was much lower compared with the outdoor time reported in Chinese children aged 6–7 years in Sydney (13.75 h per week)4 and New Zealand children aged 13–14 years (10.65 h per week).12 These studies cannot be directly compared due to the differences in age range of the study participants and study methods.
There are few hypotheses that underlie the protective effect of outdoor for myopia. Due to high light intensity outdoors, there may be less image blur and peripheral hyperopic defocus while viewing a clear distant horizon outdoors, as a result of pupillary miosis and increased depth of focus.4 Increases in blood vitamin D levels owing to an increased outdoor time may also have a protective role for myopia, but this remains unclear.11 Another hypothesis is that an excessive blue-green wavelength in outdoor scenes may be protective against myopia, whereas an excessive red wavelength may be myopigenic.14
The mean time with lux levels >1000 was 0.88 h per day on a school term weekday; 1.36 h per day on a school term weekend; 1.34 h per day on a weekday during school holiday, and 1.54 h per day on a weekend during school holidays from the light meter compared with 1.64 h per day in Caucasian young adults aged 19–23 years, for a cut-off light intensity of 882 Lux.13 The mean time with lux levels >1000 in a week from the light meter (8.08 h per week) seemed to be slightly lower compared with that reported in New Zealand children aged 13–14 years (10.65 h per week), using a cut-off light intensity >1000 Lux.12
The mean light levels throughout the week in our study were low: 702.87 Lux during the school term and 950.85 Lux during the school holidays. Light exposures of >1000 Lux accounted for a small proportion of total daylight hours in the week. A previous study has found that children spent less time outdoors (10.65±2.52 h per week or 5.88±1.39% of the total time), but these outdoor periods accounted for a large proportion of their total light exposure (4.72 × 107±1.65 × 10 7 Lux or 87.95±3.72% of their total light exposure).12 Another study has found that the average light exposure of the participants was 2200 Lux (range 300 Lux–4200 Lux) over 14 days.13 Most subjects were exposed to ≤10% of the total available light over the experimental period of 14 days.13
Increased light intensity outdoors could trigger the release of dopamine, which is an inhibitor of ocular growth.6, 7 Exposing chick eyes to laboratory light of 15 000 Lux for 5 h per day or sunlight of 30 000 Lux for 15 min per day could slow the development of myopia in chicks.6, 7 Ambient light levels as high as 18 000–28 000 Lux could retard form-deprivation myopia in infant monkeys.8
The strength of the present study is a relatively larger sample size (n=117) compared with previous studies that only included 12 children12 and 7 young adults.13 A possible limitation of the study is that the outdoor data from the diary recorded by the children may be less accurate, as the parents who filled in the diary for their children may not have monitored their children's activity throughout the day or may not have accurately recorded the activities. The light meter may not have been worn everyday or the sensor may have faced inward, and light levels may have been affected by daily weather conditions. Singapore is a country with an equatorial/tropical climate and there are no seasons. The study was conducted between April and June 2011, during the mild rainy season. All children wore the light meter during this mild rainy season. Hence, it is unlikely that seasonal changes could have affected the light meter measurements.
There may be a selection bias, as the children were volunteers who enrolled in the randomized controlled trial. Children who volunteered may have different characteristics from children who did not.
Children wore the light meter for the first week of the study, even before they participated in the weekly outdoor intervention program. Hence, it is unlikely that the intervention could have affected the light meter measurements. The light meter readings were also similar in both the control and intervention groups.
Both the outdoor diary and light meter could be used in future randomized controlled trials of outdoor interventions to evaluate the effect of the intervention on myopic refractive shifts or cohort studies to determine the effects of outdoor time and light on myopia development and progression.
In conclusion, the light meter is objective, documents light intensities, and could provide a guide to the accuracy of diary data. However, the correlation of outdoor time from the diary and high light intensities was not significantly high owing to either an inaccurate diary recording or the lack of contrast of light intensity levels outdoors vs indoors. Both instruments could be further developed and improved in future myopia epidemiological studies.

References
Dirani M, Chan YH, Gazzard G, Hornbeak DM, Leo SW, Selvaraj P et al. Prevalence of refractive error in Singaporean Chinese children: the strabismus, amblyopia, and refractive error in young Singaporean Children (STARS) study. Invest Ophthalmol Vis Sci 2010; 51: 1348–1355.
Saw SM, Goh PP, Cheng A, Shankar A, Tan DTH, Ellewin LB . Ethnicity-specific prevalences of refractive errors vary in Asian children in neighbouring Malaysia and Singapore. Br J Ophthalmol 2006; 90: 1230–1235.
Wong TY, Foster PJ, Hee J, Ng TP, Tielsch JM, Chew SJ et al. Prevalence and risk factors for refractive errors in adult Chinese in Singapore. Invest Ophthalmol Vis Sci 2000; 41: 2486–2494.
Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmol 2008; 115: 1279–1285.
Dirani M, Tong L, Gazzard G, Zhang X, Chia A, Young TL et al. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol 2009; 93: 997–1000.
Ashby RS, Schaeffel F . The effect of bright light on lens compensation in chicks. Invest Ophthalmol Vis Sci 2010; 51: 5247–5253.
Ashby RS, Schaeffel F . The effect of ambient illuminance on the development of deprivation myopia in chicks. Invest Ophthalmol Vis Sci 2009; 50: 5348–5354.
Smith EL, Hung LF, Huang J . Effects of high ambient lighting on the development of form-deprivation myopia in infant rhesus monkeys. Invest Ophthalmol vis Sci 2012; 53: 421–428.
Cohen Y, Belkin M, Yehezkel O, Solomon AS, Polat U . Dependency between light intensity and refractive development under light-dark cycles. Exp Eye Res 2011; 92: 40–46.
Wollensak G, Iomdina E, Dittert DD, Salamatina O, Stoltenbutg G . Cross-linking of scleral collagen in the rabbit using riboflavin and UVA. Acta Ophthalmol Scand 2005; 83: 477–482.
Mutti DO, Marks AR . Blood levels of vitamin D in teens and young adults with myopia. Optom Vis Sci 2011; 88: 377–382.
Backhouse S, Hannah NG, Philips J . Light exposure patterns in children: a pilot study. Abstract. International Myopia conference 2010.
Alvarez A, Wildsoet CF . Quantifying the light environments of myopes and emmetropes. Invest Ophthalmol Vis Sci 2011; 52: E-Abstract 2503.
Foulds WS, Luu CD, Barathi VA . New light on childhood myopia. Asia ARVO 2011 (abstract).
Acknowledgements
This study was funded by National Medical Research Council, EDG/NMRC/10May040.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Eye website
Supplementary information
Rights and permissions
About this article
Cite this article
Dharani, R., Lee, CF., Theng, Z. et al. Comparison of measurements of time outdoors and light levels as risk factors for myopia in young Singapore children. Eye 26, 911–918 (2012). https://doi.org/10.1038/eye.2012.49
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2012.49
Keywords
This article is cited by
-
Conjunctival ultraviolet autofluorescence as a biomarker of outdoor exposure in myopia: a systematic review and meta-analysis
Scientific Reports (2024)
-
Baseline characteristics in the Israel refraction, environment, and devices (iREAD) study
Scientific Reports (2023)
-
Light Signaling and Myopia Development: A Review
Ophthalmology and Therapy (2022)
-
Loss of Gap Junction Delta-2 (GJD2) gene orthologs leads to refractive error in zebrafish
Communications Biology (2021)
-
Time spent outdoors in childhood is associated with reduced risk of myopia as an adult
Scientific Reports (2021)
