
Abstract
Purpose
To determine the prevalence rates of refractive errors and pattern of ocular biometry in a multi-ethnic elderly Asian population.
Methods
A population-based study of 1835 residents aged 55–85 years, evaluating the refractive error and ocular biometry parameters, including axial length (AL) and anterior chamber depth.
Results
The age-standardized prevalence of myopia, hyperopia, astigmatism, and anisometropia were 30.0% (95% confidence interval (CI): 29.6, 30.4), 41.5% (95% CI: 41.1, 41.9), 43.5% (95% CI: 43.1, 44.0), and 22.1% (95% CI: 21.7, 22.4), respectively. Male gender (P=0.02), age ≥75 years (P=0.033), and higher educational level (P<0.001) were significantly associated with higher rates of myopia in multivariate analyses. The prevalence of astigmatism was higher in persons with diabetes (odds ratio (OR) 1.4, 95% CI: 1.03, 1.90, P=0.031). AL was longer in Chinese than other ethnic groups (23.7 vs23.4 mm, P=0.018), and in men compared with women (24.2 vs23.4 mm, P<0.001). AL was associated with increasing height (AL increased by 0.3 mm for every 10 cm increase in height, P<0.001).
Conclusion
There is a high prevalence of myopia in elderly Singaporeans, consistent with trends seen in younger populations in Asia. Male gender and higher education were independent risk factors for myopia. These data suggest that higher rates of myopia in East Asians compared with Caucasians may not be a recent phenomenon.
Similar content being viewed by others
Introduction
Myopia is a common treatable cause of visual impairment worldwide.1, 2 Studies in urban East Asian populations have shown a very high prevalence of myopia in Chinese in Singapore, Taiwan, and Hong Kong,3, 4, 5 while the rates of myopia are lower in Western6, 7 and other Asian countries such as India,8, 9 Bangladesh,10 and Mongolia.11
Early studies suggest that higher rates of myopia occur in younger age groups in East Asian populations.1, 8, 12 A study in Chinese aged 40–79 years in Singapore reported a prevalence of 38.7% for myopia,12 which was two times higher than similarly aged adults in the Blue Mountains Eye Study and Baltimore Eye Survey.6, 7 However, there are few studies of older adults (>65 years) in East Asia,13, 14 and a few population-based studies in Asia with biometry measures of axial length (AL).11, 15
Another unresolved issue is the role of racial variations in myopia prevalence in Asia. Although comparison of studies in different Asian countries suggest that Chinese people have higher prevalence of myopia compared with other ethnic groups,8, 9, 16 studies with similar methodology are limited. A study among 110 236 young Singapore male military conscripts showed higher rates of myopia in Chinese (48.5%) compared with Indians (30.4%), and Malays (24.5%).17 It is unclear whether these differences are seen in older Asian populations.
Our study aimed to describe the prevalence rates of refractive errors and variations in biometry among elderly Singaporeans of different ethnicities, and to evaluate risk factors associated with refractive errors, in particular, myopia.
Materials and methods
We conducted a population-based cross-sectional study in Singapore, using participants in the ongoing Singapore Longitudinal Aging Study (SLAS),18, 19 a study of 2804 adults aged 55 years or above living in a geographically defined area in the Southeast district of Singapore. Subjects were identified using door-to-door census, and all respondents signed written informed consent. The study was performed according to the guidelines of the Declaration of Helsinki and was approved by National University of Singapore Institutional Review Board. The response rate for the total of 2804 respondents was 78.5%. Interviews were conducted in the language with which the subjects were most conversant. Of the SLAS participants, 391 subjects did not have ocular examination, and another 578 subjects were excluded because of previous cataract surgery or difficulty in obtaining accurate refraction (for example, corneal scar and dense media opacity). Of the remaining 2097 subjects, 262 declined to participate in the study. Thus, data of 1835 subjects (response rate 87.5%) were available for analysis.
Eye examinations
Five consecutive refractive error (sphere, cylinder, and axis) and corneal curvature radii (CR) readings were obtained using a calibrated auto-keratorefractometer (model RK5; Canon, Tochigiken, Japan). The AL, anterior chamber depth (ACD) and CR were measured using the IOLmaster (Zeiss, Oberkochen, Germany). The AL and ACD measurements were taken as five frames automatically and averaged using the IOLmaster software, which automatically discards outliers using a custom algorithm.
Interviews
A wide range of demographical, biological, clinical, psychosocial, and behavioral characteristics were collected by interviews at specified study centers as previously described.18, 19 The regular use of vitamins A and E, history of traditional medication use, cigarette smoking, and regular alcohol consumption were studied.
Other clinical measurements and laboratory tests
Height (meter) was measured using a stadiometer, without shoes to the nearest 0.05 m, while weight (kilogram) was measured on a calibrated SECA beam balance (model 708 1314004, Vogel & Halke, Hamburg, Germany), without shoes and in lightweight clothing to the nearest 0.1 kg. Blood pressure (BP) was measured using a mercury sphygmomanometer (Accoson Dekamet, A C Cossor & Son (Surgical) Ltd, Harlow, UK). The measurement of plasma glucose has previously been described.19
Definitions and statistical analysis
The results for both eyes were analyzed separately, but because of the high correlation of spherical equivalent between the right and left eyes (r=0.867, P<0.001), data are presented for the right eye only, with the exception of anisometropia.
Spherical equivalent (SE) was calculated as the sum of spherical error and half negative cylinder. The definitions of refractive errors were: myopia, SE of at least −0.5 D; hyperopia, SE of at least +1.0 D; astigmatism, cylinder of at least −1.0 D; and ansiometropia, difference in spherical equivalent of at least 1.0 D between the two eyes.
Diagnosis of diabetes was established based on self-report, fasting blood glucose (>7 mmol/l), and the use of anti-diabetic medications, while hypertension was based on self-report, blood pressure readings of systolic BP ≥140 mm Hg or diastolic BP ≥90 mm Hg, and the use of anti-hypertensive agents.
Age, ethnicity, and gender-specific prevalence rates and 95% confidence intervals were estimated using the Poisson's distribution. Multivariate logistic regression models with myopia or other refractive error variables as the dependent variable were constructed to obtain multivariate-adjusted P-values. The statistical package for the Social Sciences (SPSS) statistical software (version 14.0; SPSS Inc., Chicago, IL, USA) was used for the analysis. Statistical significance was assumed at P<0.05.
Results
The characteristics of responders are shown in Table 1. Compared with non-respondents, the respondents were younger, included more women, and more residents in higher end housing (30.7 vs 17.3%).
Overall, the age-standardized prevalence of myopia was 30.0% (95% confidence interval (CI): 29.6, 30.4) (Table 2). The overall rate of high myopia (SE < −6.0 D) was 3.1%. Chinese had the highest prevalence rates of myopia (30.8%), compared with Indians (22.6%) and Malays (18.2%) (P=0.04). Males had significantly higher rates of refractive errors except for hyperopia. The mean refractive error varied from −0.16 D (subjects aged 55–64 years), to 0.36 D (65–74 years), and 0.08 D (subjects aged 75 years and older) (P for trend=0.001).
For all subjects, the mean AL, ACD, and AL/CR ratio decreased with successive age groups (P for trend <0.001) (Table 3). In Chinese subjects, the mean AL was 23.7 mm compared with 23.4 mm in non-Chinese (P=0.018), and the AL/CR ratio was 3.11 vs 3.08 (P=0.059). There was no significant difference in the ACD (3.02 vs 3.04 mm) and CR between Chinese and non-Chinese. Compared with females, males had a higher mean AL (24.2 vs 23.4 mm, P<0.001), ACD (3.09 vs 2.99 mm, P<0.001), corneal curvature (7.69 vs 7.58 mm, P<0.001), and AL/CR ratio (3.14 vs 3.09, P<0.001).
The risk factors for myopia and other refractive errors were analyzed using multivariate logistic regression models as shown in Table 4. Even after adjusting for all other factors in the table, males had significantly higher rates of myopia (odds ratio (OR) 1.4). Subjects aged 75 years and older had a 1.6 times risk of myopia compared with those aged 55–64 years (P=0.033), and adults with university education had 5.4 times higher risk compared with those with no education (P<0.001). Females and those with lower education had higher risks of hyperopia. The risks of astigmatism were higher in males, older adults, adults who had completed pre-university or secondary education, adults with diabetes (OR 1.4), and those who were shorter (OR 0.13). Older subjects and adults with higher levels of education had higher risks of anisometropia.
The regular use of vitamins A and E, history of traditional medication use, financial constraints, cigarette smoking, and regular alcohol use were not associated with any refractive error in multivariate analyses.
In multiple linear regression models with SE as the dependent variable, the SE was more negative in males (P<0.001), Chinese compared with Malays (P=0.021), adults aged 55–64 years compared with 65–74 years (P=0.017), taller subjects (P<0.001), and higher education compared with primary or no education (P<0.001).
Using multiple linear regression, longer AL was found in males (P=0.040), those with pre-university or university education (P<0.001), and varied with height (for every 10 cm increase in height, AL increases by 0.3 mm, P<0.001). There was no association between hypertension and AL. Age and ethnicity were not independently associated with AL.
Discussion
Our study demonstrates a high prevalence of myopia (30.1%) among elderly Singaporeans, with a higher prevalence in Chinese (30.8%) compared with Indians (22.6%) and Malays (18.2%). This corresponded to a longer mean AL in Chinese. Myopia was associated with male gender and higher education, while the risks of astigmatism were higher in adults with diabetes and those who were shorter. AL varied with gender (males), higher education, and height.
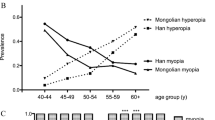
Comparisons of prevalence rates between studies must be interpreted with caution due to differences in the definitions used, measures for refractive errors, age ranges, and type of study population. The age-adjusted prevalence rate of 30.1% for myopia is higher than in many studies of same-aged adults conducted in European-derived countries, where the overall prevalence ranged from 15.5 to 26.2%.6, 7, 20, 21 The prevalence rates of myopia in Asian populations, analyzed by specific age groups, is shown in Table 5. Several studies showed higher prevalence of myopia with increasing age, including studies in Chinese,12 Indonesians,16 Indians,8, 9 Bangladeshi,10 and Mongolians.11
Our study showed a lower age-adjusted prevalence of myopia among Chinese compared with the Tanjong Pagar Study (30.8 vs 38.7%).12 This is expected because the latter included subjects aged 40–79 years. Compared with the Shihpai Eye Study,14 of elderly Chinese in Taiwan, our Chinese subjects had higher prevalence of myopia in the corresponding age groups: 31.5% (65–74 years) vs 12.8% (65–69 years) and 19.4% (70–74 years) and; 39.7% (≥75 years) vs 26.5% (75–79 years). In contrast, the Beijing Eye Study found a lower prevalence of 22.9%13 and the Mongolian eye study reported rates of 21% for those aged 60–69 years and 26.5% for those aged 70 and above.11 Studies in India8, 9 and Bangladesh10 have reported myopia rates over 40% in those aged 60 or older.
An important finding in this study is the higher prevalence rate of myopia among males compared with females (38.9 vs 25.1%, P<0.001). This finding is uncommon compared with most other studies, who have reported either a higher rate among females,12, 13, 20, 21 or no difference among the genders.6, 7, 14, 16 The Barbados Eye Study and the National Blindness and Low Vision Prevalence Survey of Bangladesh10 both reported higher rates of myopia among males, and the latter study reported that women were less likely to be emmetropic or myopic (OR 0.75). We also found on multivariate analyses that males had significantly more negative spherical equivalent (P<0.001) and longer AL compared with females (P=0.040).
In this study, we found that the risk of myopia increased progressively with education, with those with university education having 5.4 times the risk compared with those without education (P<0.001) (Table 4). Similar associations of education with myopia risk have been reported in both Western6, 7, 20, 21 and Asian studies.8, 12, 13, 14 In addition, studies have reported an association between myopia and other indicators of socio-economic status such as income,12, 16 profession,12, 21 and type of housing.12
An interesting finding in our study is the higher rates of myopia among Chinese compared with Indians and Malays, which has not previously been described in elderly Asians of varied ethnicity living within the same geographical region. An earlier study among 110 236 young Singapore males reported similar results.17 We also found a significantly more negative spherical equivalent among Chinese compared with Malays on multivariate analysis (P=0.022). Compared with the prevalence rate of myopia among Malays (18.2%), a study of refractive errors in rural Indonesian subjects16 reported a prevalence rate of 39.7% in those aged 50 and above. The prevalence rate of myopia among Singapore Indians (22.6%) was similar to Indians in an urban Indian population (Andhra Pradesh Eye Disease Study) (19.3%)8 but lower than that of the rural population (30.97%).9 The more myopic refractions in Singapore Chinese compared with Singapore Malays and Indians could be attributed to inter-ethnic, environmental, or genetic differences. Ethnicity may be a surrogate for differences in the intensity of schooling, near work or outdoor activity. However, definite conclusions cannot be made because the number of Malays and Indians in our study is small.
The increase in myopia in extreme old age is likely to be due to lens-induced refractive index changes related to increase in nuclear sclerotic cataracts. However, the Beaver Dam Eye Study used two different models to account for the effect of nuclear sclerosis, but found that although this may attenuate the shift in myopia, age was still an important factor in the increase in myopia in this group.22 The lack of definite clinical assessment and grading of cataract in our study is a potential limitation.
We studied the use of antioxidants, cigarette smoking, and alcohol consumption as possible novel risk factors for myopia. Our results found no association between these factors and the prevalence of myopia.
Our study found that astigmatism was higher in males, older, and shorter subjects, and those with higher education. Other studies have demonstrated similar associations with age,6, 14, 16 race,6 and gender.6, 16 Interestingly, our study showed that astigmatic adults were more likely to be diabetic. A study of 224 patients in Nepal found that non-diabetics had higher corneal astigmatism (0.30 D) compared with diabetics (0.07 D).23
A strength of our study is the review of both refractive errors and biometry in the same population, which is not frequently reported.11, 15 There are several interesting findings in our biometry results. Using multiple linear regression, the AL was significantly higher in males compared with females (24.2 vs 23.4 mm, P<0.001), corresponding to the significantly higher prevalence of myopia among males (38.9 vs 25.1%, P<0.001). The Tanjong Pagar Survey reported significantly higher AL among males compared with females (23.54 vs 22.98 mm, P<0.001),15 but found higher rates of myopia among females, especially high myopia.12 We also found a significant, progressive decrease in AL across successive age groups, which was also described in the Tanjong Pagar Survey,15 but not in the study of Mongolian adults.11
The AL in our population (23.77 mm) was higher compared with the Tanjong Pagar Survey15 (n=1717) of Chinese adults aged 40 to 81 years (23.2 mm) and in a cross-sectional study of Mongolian adults11 (n=1800) aged 40 years (23.1 mm). In the latter study, the prevalence of myopia was lower than in our study (17.2 vs 30.8%). In our study, an increase in height was significantly associated with longer AL. Similar findings were described in the Tanjong Pagar Survey,15 the Reykjavik Eye Study,24 and in the school children in both Singapore25 and Australia.26 However, in multivariate analysis, height was not a risk factor for myopia. Several other studies have also reported no association between height and myopia,15, 27, 28, 29 although a study of Singapore children aged 7 to 9 years found height significantly associated with refractive error in females.25 Several studies of adults have also found that AL was correlated with refractive error.11, 29 In this study, the mean AL is longer in Chinese compared with non-Chinese (23.7 vs 23.4 mm), but this difference was not significant in multivariate analysis.
The advantages of our population-based survey include a fairly large sample size, and the evaluation of a comprehensive list of possible risk factors for refractive error including vitamin use, diabetes, and hypertension. Potential limitations include the small number of Malay and Indian participants that may preclude any definite conclusions about inter-ethnic differences. Because the SLAS study was launched to evaluate neurodegenerative disorders, there is lack of precise clinical or photographic assessment and grading of cataract. This may limit our inferences on the effect of age on myopia rates.
In summary, our study has demonstrated a high prevalence of myopia in elderly Singaporeans, consistent with trends seen in younger East Asian populations. These data provide further evidence that the higher rates of myopia in East Asians compared with Caucasian population is not a recent phenomenon. Chinese had more myopic refractions compared with Malays and Indians.

References
Wong TY, Loon SC, Saw SM . The epidemiology of age related eye diseases in Asia. Br J Ophthalmol 2006; 90: 506–511.
Seet B, Wong TY, Tan DT, Saw SM, Balakrishnan V, Lee LK et al. Myopia in Singapore: taking a public health approach. Br J Ophthalmol 2001; 85: 521–526.
Lin LL, Chen CJ, Hung PT, Ko LS . Nation-wide survey of myopia among school children in Taiwan, 1986. Acta Ophthalmol 1988; 66: 29–33.
Lin LL, Shih YF, Tsai CB, Chen CJ, Lee LA, Hung PT et al. Epidemiologic study of ocular refraction among schoolchildren in Taiwan in 1995. Optom Vis Sci 1999; 76: 275–281.
Van Newkirk MR . The Hong Kong vision study: a pilot assessment of visual impairment in adults. Trans Am Ophthalmol Soc 1997; 95: 715–749.
Katz J, Tielsch JM, Sommer A . Prevalence and risk factors for refractive errors in an adult inner city population. Invest Ophthalmol Vis Sci 1997; 38: 334–340.
Attebo K, Ivers RQ, Mitchell P . Refractive errors in an older population: the Blue Mountains Eye Study. Ophthalmology 1999; 106: 1066–1072.
Dandona R, Dandona L, Naduvilath TJ, Srinivas M, McCarty CA, Rao GN et al. Refractive errors in an urban population in Southern India: the Andhra Pradesh Eye Disease Study. Invest Ophthalmol Vis Sci 1999; 40: 2810–2818.
Raju P, Ramesh SV, Arvind H, George R, Baskaran M, Paul PG et al. Prevalence of refractive errors in a rural South Indian population. Invest Ophthalmol Vis Sci 2004; 45: 4268–4272.
Bourne RR, Dineen BP, Ali SM, Noorul Huq DM, Johnson GJ . Prevalence of refractive error in Bangladeshi adults: results of the National Blindness and Low Vision Survey of Bangladesh. Ophthalmology 2004; 111: 1150–1160.
Wickremasinghe S, Foster PJ, Uranchimeg D, Lee PS, Devereux JG, Alsbirk PH et al. Ocular biometry and refraction in Mongolian adults. Invest Ophthalmol Vis Sci 2004; 45: 776–783.
Wong TY, Foster PJ, Hee J, Ng TP, Tielsch JM, Chew SJ et al. Prevalence and risk factors for refractive errors in adult Chinese in Singapore. Invest Ophthalmol Vis Sci 2000; 41: 2486–2494.
Xu L, Li J, Cui T, Hu A, Fan G, Zhang R et al. Refractive error in urban and rural adult Chinese in Beijing. Ophthalmology 2005; 112: 1676–1683.
Cheng CY, Hsu WM, Liu JH, Tsai SY, Chou P . Refractive errors in an elderly Chinese population in Taiwan: the Shihpai Eye Study. Invest Ophthalmol Vis Sci 2003; 44: 4630–4638.
Wong TY, Foster PJ, Ng TP, Tielsch JM, Johnson GJ, Seah SK . Variations in ocular biometry in an adult Chinese population in Singapore: the Tanjong Pagar Survey. Invest Ophthalmol Vis Sci 2001; 42: 73–80.
Saw SM, Gazzard G, Koh D, Farook M, Widjaja D, Lee J et al. Prevalence rates of refractive errors in Sumatra, Indonesia. Invest Ophthalmol Vis Sci 2002; 43: 3174–3180.
Au Eong KG, Tay TH, Lim MK . Race, culture and Myopia in 110 236 young Singaporean males. Singapore Med J 1993; 34: 29–32.
Ng TP, Tan CH, Kua EH, Singapore Chinese Longitudinal Aging Study. The use of Chinese herbal medicines and their correlates in Chinese older adults: the Singapore Chinese Longitudinal Aging Study. Age Ageing 2004; 33: 135–142.
Feng L, Ng TP, Chuah L, Niti M, Kua EH . Homocysteine, folate, and vitamin B-12 and cognitive performance in older Chinese adults: findings from the Singapore Longitudinal Ageing Study. Am J Clin Nutr 2006; 84: 1506–1512.
Wang Q, Klein BE, Klein R, Moss SE . Refractive status in the Beaver Dam Eye Study. Invest Ophthalmol Vis Sci 1994; 35: 4344–4347.
Wensor M, McCarty CA, Taylor HR . Prevalence and risk factors of myopia in Victoria, Australia. Arch Ophthalmol 1999; 117: 658–663.
Mutti DO, Zadnik K . Age-related decreases in the prevalence of myopia: Longitudinal change or cohort effect? Invest Ophthalmol Vis Sci 2000; 41: 2103–2107.
Paudel RP, Adhikari BN, Kaini KR . Clinical evaluation of corneal astigmatism in non diabetic and diabetic patients. Nepal Med Coll J 2006; 8: 162–165.
Eysteinsson T, Jonasson F, Arnarsson A, Sasaki H, Sasaki K . Relationships between ocular dimensions and adult stature among participants in the Reykjavik Eye Study. Acta Ophthalmol Scand 2005; 83: 734–738.
Saw SM, Chua WH, Hong CY, Wu HM, Chia KS, Stone RA et al. Height and its relationship to refraction and biometry parameters in Singapore Chinese children. Invest Ophthalmol Vis Sci 2002; 43: 1408–1413.
Ojaimi E, Morgan IG, Robaei D, Rose KA, Smith W, Rochtchina E et al. Effect of stature and other anthropometric parameters on eye size and refraction in a population-based study of Australian children. Invest Ophthalmol Vis Sci 2005; 46: 4424–4429.
Rosner M, Laor A, Belkin M . Myopia and stature: findings in a population of 106 926 males. Eur J Ophthalmol 1995; 5: 1–6.
Jacobsen N, Jensen H, Goldschmidt E . Prevalence of myopia in Danish conscripts. Acta Ophthalmol Scand 2007; 85: 165–170.
Olsen T, Arnarsson A, Sasaki H, Sasaki K, Jonasson F . On the ocular refractive components: the Reykjavik Eye Study. Acta Ophthalmol Scand 2007; 85: 361–366.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Tan, C., Chan, Y., Wong, T. et al. Prevalence and risk factors for refractive errors and ocular biometry parameters in an elderly Asian population: the Singapore Longitudinal Aging Study (SLAS). Eye 25, 1294–1301 (2011). https://doi.org/10.1038/eye.2011.144
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2011.144
Keywords
This article is cited by
-
High prevalence of refractive errors in an elderly population; a public health issue
BMC Ophthalmology (2023)
-
Global metrics on ocular biometry: representative averages and standard deviations across ten countries from four continents
Eye (2023)
-
Effect of refractive status on retinal nerve fiber layer thickness in Chinese Population
Graefe's Archive for Clinical and Experimental Ophthalmology (2023)
-
Myopia prevalence and ocular biometry: a cross-sectional study among minority versus Han schoolchildren in Xinjiang Uygur autonomous region, China
Eye (2022)
-
Prevalence and risk factors of refractive error in Qinghai, China: a cross-sectional study in Han and Tibetan adults in Xining and surrounding areas
BMC Ophthalmology (2021)
